
Open Access, Volume 11
Refractory severe hypercalcemia in primary hyperparathyroidism: A case report
Nahlah Alreshidi; Nicholas Rozza*; Amichai Grunbaum; Richard Kremer
Department of Medicine, Department of Biochemistry, MC Gill University, Health Center, Montreal, Quebec, Canada.
Nicholas Rozza
Department of Medicine and Biochemistry, MC Gill University, Health Center, Montreal,
Quebec, Canada.
Email: nicholas.rozza@mail.mcgill.ca
Received : October 16, 2025,
Accepted : November 19, 2025
Published : November 28, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Primary Hyperparathyroidism (PHPT) is characterized by autonomous overproduction of Parathyroid Hormone (PTH), leading to hypercalcemia and its systemic effects. It is the most common cause of hypercalcemia encountered in outpatient settings. In such cases, management becomes complex and necessitates a multidisciplinary approach utilizing pharmacological agents and supportive therapy. We present a case of a 69-year-old woman with severe hypercalcemia secondary to Primary Hyperparathyroidism (PHPT), refractory to multiple lines of medical therapy. Surgical intervention was contraindicated due to significant comorbidities including cardiovascular disease, cerebrovascular risk, and recent colorectal cancer. Despite optimized use of anti-resorptive agents, hydration therapy, and calcimimetic treatment, the patient’s serum calcium levels remained persistently elevated. This case highlights the challenges in managing inoperable PHPT and supports a multimodal and sustained medical management approach.
Keywords: Refractory hyperparathyroidism; Medical management; Refractory hypercalcemia.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Rozza N (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Alreshidi N, Rozza N, Grunbaum A, Kremer R. Refractory severe hypercalcemia in primary hyperparathyroidism: A case report. Open J Clin Med Case Rep. 2025; 2394.
Introduction
Primary Hyperparathyroidism (PHPT) is characterized by autonomous overproduction of parathyroid hormone (PTH), leading to hypercalcemia and its systemic effects. It is the most common cause of hypercalcemia encountered in outpatient settings [1-6,7]. While the typical manifestations of primary hyperparathyroidism can include complications such as nephrocalcinosis, nephrolithiasis, hypercalcuria and osteoporosis, these occurrences are relatively uncommon [2,3]. It is important to note that surgical intervention is recognized as the most effective treatment for individuals with this condition. a significant number of patients do not match the predefined criteria for surgical procedures or have concomitant disorders that prevent them from undergoing surgery [4,5]. In such cases, management becomes complex and necessitates a multidisciplinary approach utilizing pharmacological agents and supportive therapy. We describe a case of medically refractory PHPT in an elderly patient where multiple anti-resorptive agents and supportive measures were used over a prolonged course.
Case Presentation
A 69-year-old woman with a medical history significant for cardiovascular disease, prior cerebrovascular accident, and recent colorectal cancer presented with symptomatic hypercalcemia. Laboratory evaluation revealed a Parathyroid Hormone (PTH) level of 22.1 pmol/L (normal: 1.50-9.30 pmol/L) and serum calcium of 2.86 mmol/L (normal: 2.12-2.62 mmol/L) ionized calcium 1.4 mmol/L (normal: 1.15-1.32 mmol/L), vitamin D 69 nmol/L (normal: 50-125 nmol/L). The hypercalcemia was complicated by nephrolithiasis. Renal function and Parathyroid Hormone-Related Peptide (PTHrP) were within normal limits. Given her significant surgical risk, parathyroidectomy was not a viable option. An FDG PET-CT ruled out osseous metastases, and secondary causes of hypercalcemia were excluded. Initial management included vitamin D supplementation, which normalized 25-hydroxyvitamin D (25(OH)D) to 130 nmol/L, elevated 1,25-dihydroxy vitamin D of 338 pmol/L (normal: 48-190 pmol/L) which possibly led further elevation of calcium levels (peak 3.5 mmol/L). Despite multiple courses of anti-resorptive therapy—IV pamidronate, IV zoledronic acid, and subcutaneous denosumab over 3 months —calcium remained persistently above 3.0 mmol/L. Recurrent symptomatic hypercalcemia was further managed with IV saline followed by loop diuretics every two weeks, which temporarily reduced serum calcium to 2.7 mmol/L. However, levels quickly rebounded. Monthly zoledronic acid infusions were resumed, and vitamin D supplementation was withheld, with 25(OH)D levels subsequently falling to 83 nmol/L. Nonetheless, calcium remained elevated at 2.9 mmol/L. Cinacalcet was initiated at 30 mg orally three times daily, with minimal effect. The patient was eventually hospitalized for symptomatic hypercalcemia presenting as generalized fatigue, weight loss, and cognitive impairment. During admission, she received continuous IV hydration and one dose of zoledronic acid, leading to temporary normalization in serum calcium to 2.5 mmol/L. Cinacalcet was up-titrated to 120 mg daily. Imaging, including CT chest, abdomen, pelvis, and brain, ruled out malignancy or acute neurological causes. Upon discharge, she continued a regimen of IV hydration and loop diuretics every two weeks, along with monthly zoledronic acid and maximum-dose cinacalcet, but calcium levels remained elevated at 2.9 mmol/L.
Key laboratory values over time
| Test | Initial | Extreme value | Final |
|---|---|---|---|
| Serum Calcium (mmol/L) | 2.86 | 3.5 | 2.9 |
| Ionized Ca | 1.41 | 1.91 | 1.58 |
| PTH (pmol/L) | 22.1 | 64.3 | 46.30 |
| 25(OH)D (nmol/L) | 69 | 130 | 83 |
| 1,25(OH)2D (pmol/L) | 384 | 531 | 531 |
| Serum Phosphate | 0.94 | 0.32 | 0.53 |
| PTHrP | <11 | - | - |
| Creatinine | 60 | 109 | 69 |
| Alkaline phosphatase | 113 | 139 | 90 |
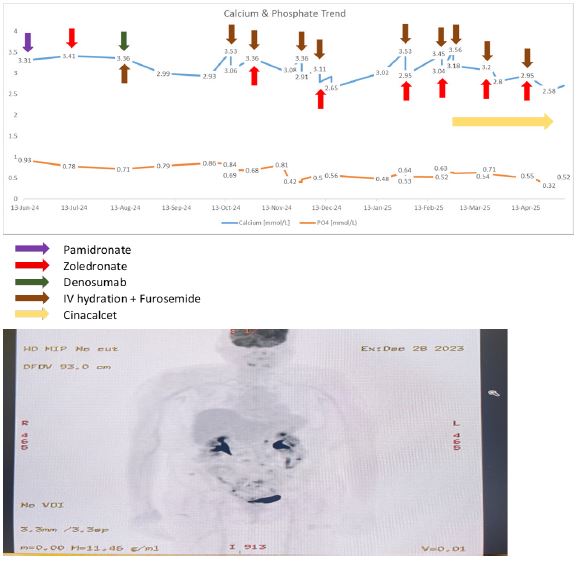
Figure 1: FDG whole body scan showed no osseous lesions or metastasis.
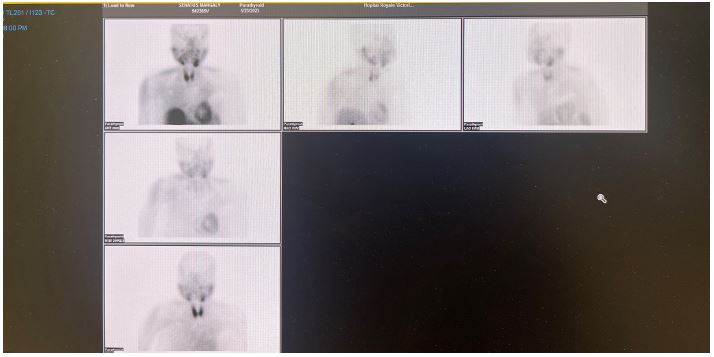
Figure 2: Parathyroid MIBI scan showed no localization for parathyroid adenoma.
Discussion
Primary Hyperparathyroidism (PHPT) is characterized by autonomous overproduction of Parathyroid Hormone (PTH), leading to hypercalcemia and its systemic effects. While parathyroidectomy is the definitive treatment, a subset of patients is deemed ineligible for surgery due to significant comorbid conditions. Our patient, with a history of recent colorectal cancer and severe cardiovascular and cerebrovascular disease, was not a surgical candidate. In such cases, medical therapy becomes the mainstay of management, although it is often challenging and may not result in sustained normocalcemia.
Initial treatment of hypercalcemia in PHPT includes intravenous hydration with isotonic saline to enhance renal calcium excretion, sometimes combined with loop diuretics to prevent volume overload in patients with comorbid cardiac disease [6,7]. Our patient responded only temporarily to IV hydration. This is not uncommon, as the underlying hypersecretion of PTH remains uncorrected.
Anti-resorptive agents such as bisphosphonates are commonly used to suppress bone resorption and lower serum calcium. Zoledronic acid has been shown to be effective, though the response may be delayed and transient [8)]. In patients with renal impairment or resistance to bisphosphonates, denosumab, a monoclonal antibody against RANKL, may serve as an alternative and has shown efficacy in refractory hypercalcemia, including PHPT cases not suitable for surgery [9,10]. Denosumab was used in our case but did not show any effect on hypercalcemia.
Cinacalcet, a calcimimetic that increases the sensitivity of the calcium-sensing receptor on parathyroid cells, suppresses PTH secretion and lowers serum calcium. It is the only medical therapy approved for the treatment of hypercalcemia in patients with inoperable PHPT [11]. However, as observed in our patient, its effect may be limited or transient. Some studies have reported that cinacalcet can normalize calcium levels in approximately 70-80% of patients, though the response is variable and often requires long-term adherence [12,13].
This case underscores the limitations of current medical therapy in managing severe PHPT when surgery is contraindicated. For patients with persistent hypercalcemia, repeated doses of antiresorptive agents or off-label use of denosumab may be needed. But in our case even repeated antiresorptive with additional dose of densoumab showed no effect.
In select cases, investigational or minimally invasive therapies such as percutaneous ethanol injection or radiofrequency ablation of parathyroid adenomas have been used with some success, particularly in patients who are not surgical candidates, though these techniques require specialized expertise and are not widely available [14,15].
Ultimately, this case highlights the importance of individualized treatment plans and ongoing reassessment of surgical risk, as medical therapy often provides only temporary biochemical control without addressing the underlying disease.
Our patient demonstrated partial and short-lived responses to each modality, with recurrent hypercalcemia despite combination therapy. The persistently elevated 1,25-dihydroxy vitamin D likely contributed to the hypercalcemia, potentially due to unregulated PTH-mediated conversion. Additionally, hydration and loop diuretics provided only temporary relief and required repeated administration. The case underscores the limited and transient efficacy of current medical therapies in severe PHPT when surgery is contraindicated.
Conclusion
In patients with severe, symptomatic PHPT who are poor surgical candidates, a multimodal approach combining hydration, anti-resorptives, and calcimimetics may be necessary to manage calcium levels. However, responses are often incomplete, requiring repeated interventions. This case highlights the need for:
• Close monitoring of calcium and vitamin D metabolites
• Judicious use of vitamin D supplementation
• Continued use of cinacalcet at maximum tolerated dose
• Periodic reassessment of surgical eligibility
• Consideration of emerging therapies such as etelcalcetide or clinical trials
Declarations
Acknowledgments: This research was funded by the Canadian Institutes of Health Research (MOP-142287) to RK.
References
- Minisola S, Arnold A, Belaya Z, et al. Epidemiology, pathophysiology and genetics of primary hyperparathyroidism. J Bone Miner Res. 2022; 37: 2315-2329.
- Bilezikian JP, Silverberg SJ, Bandeira F, et al. Management of primary hyperparathyroidism. J Bone Miner Res. 2022; 37: 2391-2403.
- Clarity Group. Tool to assess risk of bias in randomized controlled trials. Available from: href="https://www.evidencepartners.com/resources/methodological-resources/tool-to-assess-risk-of-bias-in-randomized-controlled-trials-distillersr" https://www.evidencepartners.com/resources/methodological-resources/tool-to-assess-risk-of-bias-in-randomized-controlled-trials-distillersr
- Tay Y-KD, Liu M, Bandeira L, et al. Occult urolithiasis in asymptomatic primary hyperparathyroidism. Endocr Res. 2018; 43: 106-115.
- Saponaro F, Cetani F, Mazoni L, et al. Hypercalciuria: its value as a predictive risk factor for nephrolithiasis in asymptomatic primary hyperparathyroidism. J Endocrinol Invest. 2020; 43: 677-682.
- Bilezikian JP, Brandi ML, Eastell R, et al. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the Fourth International Workshop. J Clin Endocrinol Metab. 2014; 99: 3561-3569.
- Khan AA, Hanley DA, Rizzoli R, et al. Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management in Canada. Osteoporos Int. 2017; 28: 1-19.
- Silverberg SJ, Shane E, de la Cruz L, et al. Bisphosphonate therapy in primary hyperparathyroidism. J Bone Miner Res. 1989; 4: 283-288.
- Lamy O, Gonzalez-Rodriguez E, Stoll D, et al. Severe hypercalcemia in a patient with primary hyperparathyroidism and renal insufficiency successfully treated with denosumab. J Clin Endocrinol Metab. 2013; 98: 3861-3866.
- Vargas-Poussou R, et al. Denosumab treatment of hypercalcemia due to primary hyperparathyroidism in patients unable to undergo parathyroidectomy. Bone. 2020; 136: 115380.
- Peacock M, Bilezikian JP, Bolognese MA, et al. Cinacalcet hydrochloride maintains long-term normocalcemia in patients with primary hyperparathyroidism. J Clin Endocrinol Metab. 2005; 90: 135-141.
- Marcocci C, Chanson P, Shoback D, et al. Cinacalcet reduces serum calcium concentrations in patients with intractable primary hyperparathyroidism. J Clin Endocrinol Metab. 2009; 94: 2766-2772.
- Shoback DM. Clinical practice. Hypoparathyroidism. N Engl J Med. 2008; 359: 391-403.
- Kebebew E, Siperstein AE, Clark OH, Duh QY. Surgical treatment of hyperparathyroidism in patients with multiple endocrine neoplasia type 1. Arch Surg. 2000; 135: 556-562.
- Chen H, Mack E, Starling JR. Radioguided parathyroidectomy is equally successful for hyperplasia and adenoma. Surgery. 2003; 134: 530-535.
