
Open Access, Volume 11
Hydralazine-induced lupus presenting with pleural effusion: A case report
Yasser Kailani, OMS-III1,2*; Yasir Lal, MD1,2; Jacob Seiber, MD1,2; Amer Zebi, MD1,2
1Texas College of Osteopathic Medicine, University of North Texas Health Science Center, Fort Worth, TX, USA.
2Texoma Medical Center, Denison, TX, USA.
Yasser Kailani
Texas College of Osteopathic Medicine, University of North Texas Health Science Center, Fort Worth, TX, USA & Texoma Medical Center, Denison, TX, USA.
Email: yasserkailani@gmail.com
Received : October 28, 2025,
Accepted : November 14, 2025
Published : November 28, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Drug-induced lupus is a rare autoimmune response to certain medications leading to systemic lupus erythematosus–like symptoms. While the pathogenesis of drug-induced lupus has not been fully uncovered, research has shown that certain drugs, such as hydralazine, are notorious for the development of drug-induced lupus [1-3]. Compared with idiopathic systemic lupus erythematosus, drug-induced lupus usually manifests with less severe clinical features and tends to improve within weeks to months once the offending medication is withdrawn [1,2]. We present a case of a 53-year-old male with a past medical history of end-stage renal disease on dialysis, congestive heart failure, type 2 diabetes mellitus, prostate and testicular cancer, and hyperthyroidism who was admitted for dyspnea. Initial chest X-rays demonstrated a large right- sided pleural effusion. Thoracentesis revealed blood-tinged serosanguinous fluid, with only mild reduction in symptoms. Repeat chest x-rays demonstrated persistent effusion, and the patient underwent pleurodesis. Recurrent and unresolving pleural effusions led to suspicion of drug- induced lupus and the discovery of anti-histone antibodies. Hydralazine was determined to be the culprit and subsequently discontinued. The patient was stabilized and discharged.
Keywords: Drug-induced lupus; Hydralazine; Hydralazine-induced lupus; Anti-histone antibody; Pleural effusion.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kailani Y (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Kailani Y, Lal Y, Seiber J, Zebi A. Hydralazine-Induced lupus presenting with pleural effusion: A case report. Open J Clin Med Case Rep. 2025; 2393.
Introduction
Drug-induced lupus is an uncommon autoimmune reaction triggered by specific medications, producing a spectrum of symptoms that resemble systemic lupus erythematosus [1-3]. Although the pathogenesis remains unclear, genetic predisposition and immune defects may increase risk [1]. Compared with idiopathic systemic lupus erythematosus, drug-induced lupus usually manifests with less severe clinical features and tends to improve within weeks to months once the offending medication is withdrawn [1,2]. Drug-induced lupus can present with a wide array of symptoms, including myalgia, fever, weight loss, cutaneous involvement, and serositis [1-3]. CNS involvement, glomerulonephritis, and pericarditis are rare and usually limited to severe cases [1,2].
Case Presentation
Our patient is a 53-year-old male with a past medical history of significant for end stage renal disease on dialysis, congestive heart failure, type 2 diabetes mellitus, a history of prostate and testicular cancer, and hyperthyroidism who was initially admitted for dyspnea. The patient had noted worsening shortness of breath over the past 3 months prior to admission, worse with exertion. The patient’s medications at the time of admission included Carvedilol 6.25 mg twice daily, Furosemide 80 mg twice daily, Hydralazine 50 mg three times daily, Methimazole 5 mg three times daily, and Lisinopril 10 mg three times daily.
Patient presented with elevated blood pressure at 174/88. BMP was significant for Na 133, K 4.6, BUN 29, Cr 5.3. CMP is significant for Albumin 2.5. CBC was significant for Hb 8.7, Hct 25.0. D-dimer was found elevated at 4,670. PT and INR were normal. ABG significant for pH 7.52, pCO2 31.4, HCO3 25.3. A chest x-ray on admission demonstrated a large right-sided pleural effusion, contributing to significant compressive atelectasis of the right lung and leftward deviation of the mediastinal structures. Thoracentesis was performed, which demonstrated blood- tinged serosanguinous fluid. Transthoracic echocardiogram demonstrated EF 60-65%, LV diastolic dysfunction, with trace mitral and tricuspid regurgitation, and was negative for pericardial effusion. CT Chest demonstrated a large volume right-sided pleural effusion without pneumothorax, with extensive progressive atelectasis throughout the right lung. There was also a trace left-sided pleural effusion and pleural thickening with round atelectasis in the posterior left lower lobe, as well as minimal interstitial edema in the left lung. A chest tube was placed with consistent drainage throughout admission. Repeat chest x-rays continued to demonstrate pleural effusion. Thoracotomy, decortication, and pleurodesis were performed with Video-Assisted Thoracoscopic Surgery (VATS), with significant improvement of symptoms. The pleural fluid biopsy was negative for malignancy and revealed fibrocollagenous tissue with chronic inflammation and a few reactive epithelial cells. Thorough review of the patient’s medication list led to suspicion that the patient’s 50 mg Hydralazine three times a day may be the offending agent. Anti-histone antibody titers were found to be elevated at 3.7. Free Kappa and Lambda light chains were elevated. Antinuclear Antibody (ANA) titers were found to be negative. Hydralazine was discontinued, and after chest tube removal and improved chest x-ray, the patient was discharged home. It was recommended that the patient follow up with their primary care provider and rheumatologist.

Figure 1: Chest radiographs demonstrating large right sided pleural effusion, and small left lower pleural effusion.
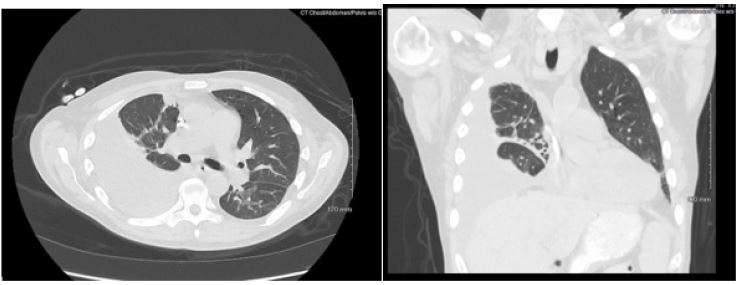
Figure 2: Axial and coronal view of chest CT with IV contrast demonstrating large right sided pleural effusion with compressive atelectasis.
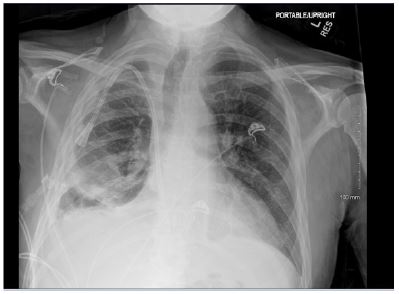
Figure 3: Chest radiographs obtained post-VATS and prior to discharge. Compared to initial presentation, there is marked interval improvement with resolution of the large right pleural effusion and re- expansion of the right lung.
Discussion
Drug-induced lupus remains a diagnostic challenge because its clinical manifestations can overlap significantly with idiopathic systemic lupus erythematosus. Hydralazine was among the first medications historically linked to drug-induced lupus and remains a well-documented cause, even though its use has declined with the availability of newer antihypertensives. The incidence of hydralazine-induced lupus is estimated to be 5-10%, with risk correlating to cumulative dose and duration of therapy [1-3]. Classic symptoms include arthralgias, fever, myalgias, rash, and serositis; however, severe or atypical presentations can also occur. In our patient, recurrent pleural effusion reflected a less common but well-described manifestation of hydralazine- induced lupus [4-6].
Our patient’s presentation highlights several diagnostic pearls. The presence of recurrent unilateral pleural effusions, despite appropriate drainage and negative cytology, raised suspicion of an autoimmune etiology. While ANA was negative, the elevated anti-histone antibody level was strongly supportive of drug-induced lupus. Importantly, ANA negativity does not rule out drug-induced lupus; rare cases of ANA-negative but anti-histone–positive hydralazine lupus have been reported [2,4]. The exclusion of other causes of pleural effusion, including infection, malignancy, and congestive heart failure, further supports hydralazine as the offending agent.
Clinical improvement and complete resolution following withdrawal of hydralazine strengthen the causal association, consistent with previously reported cases [5-7].
This case highlights the importance of heightened clinical awareness of drug-induced etiologies when evaluating unexplained pleural effusions. In patients with multiple comorbidities and polypharmacy, medication review is essential, as discontinuation of the offending agent often results in significant improvement and may prevent unnecessary interventions. Our findings contribute to the growing literature on atypical presentations of hydralazine and emphasize that serositis, including pleural effusion, should be recognized as a potential manifestation of drug- induced lupus.
Conclusion
Hydralazine is one of the most common antihypertensive agents used in end-stage renal disease. Recurrent pleural effusion is often attributed to volume overload; however, this case presents a clinical dilemma when, despite achieving volume removal with dialysis, pleural fluid continues to re-accumulate and the patient ultimately requires VATS. Hydralazine-induced drug lupus must be considered when, despite euvolemia, patients remain dyspneic with recurrent pleural effusions. Negative ANA can be misleading, and a thorough diagnostic workup must include serologies such as anti-histone antibodies. Physicians should maintain a high index of suspicion for drug-induced lupus in patients on hydralazine presenting with unexplained systemic or serosal manifestations, as early recognition and prompt withdrawal of the culprit drug are crucial to prevent morbidity and avoid unnecessary invasive procedures.
Ultimately, this case reinforces the clinical lesson that thorough medication history remains a cornerstone of medicine. Awareness of hydralazine’s lupus-inducing potential, particularly in long-term therapy, ensures timely diagnosis and appropriate management.
Declarations
Disclosures: Patient consent was obtained, and no identifying information is included in this report.
References
- He Y, Sawalha AH. Drug-induced lupus erythematosus: an update on drugs and mechanisms. Curr Opin Rheumatol. 2018; 30: 490–497.
- StatPearls. Drug-induced lupus erythematosus. NCBI Bookshelf. 2023.
- Medscape. Drug-induced lupus erythematosus overview. 2025.
- Jerome R, et al. Drug-induced systemic lupus erythematosus: a rare presentation of hydralazine-induced lupus. Cureus. 2024.
- Nogueira AR, et al. Severe presentation of drug-induced lupus erythematosus. J Med Cases. 2019; 10: 176–180.
- Paudel R, et al. Hydralazine-induced lupus after years of use. Cureus. 2025.
- Tatineni S, et al. Over the HILs: a unique presentation of hydralazine-induced lupus. SHM Abstracts. 2024.
