
Open Access, Volume 11
Novel use of daratumumab in a rare dual plasmacytoma of the humerus and pancreas: A case report
Samah Seif1*; Ahmad Assi2; Rhea Khazen3; Hampig Raphael Kourie1; Jacques Ghorayeb4; Eid Mahfouz5; Vicky Najjar3; Celina Doueihy5
1Department of Hematology and Oncology, Saint Joseph University of Beirut, Hotel-Dieu de France Hospital, Lebanon.
2Faculty of Medicine, Saint Joseph University of Beirut, Lebanon.
3Pathology Department, Saint Joseph university of Beirut, Hotel-Dieu de France Hospital, Lebanon.
4Department of Orthopedic Surgery, Saint Joseph University Hospital, Faculty of Medicine, Saint Joseph University, Beirut, Lebanon.
5Department of Gastroenterology and Hepatology, Hotel-Dieu de France Hospital, Lebanon.
Samah Seif
Department of Hematology and Oncology, Saint Joseph university of Beirut, Hotel-Dieu de France
Hospital, Lebanon.
Email: samah.seif@net.usj.edu.lb
Received : September 18, 2025,
Accepted : October 24, 20255
Published : October 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Background: Plasmacytomas are rare monoclonal plasma cell neoplasms, with extramedullary involvement being uncommon. Pancreatic plasmacytoma is exceedingly rare, and dual-site involvement remains poorly documented.
Case presentation We report a case of a 69-year-old male diagnosed with simultaneous plasmacytomas in the humerus and pancreas. Diagnosis was confirmed through imaging, histopathology, and immunohistochemistry. Given the multifocal involvement, systemic therapy with daratumumab and lenalidomide was initiated. The patient exhibited significant clinical and radiological improvement, with near-complete resolution of both lesions
Conclusion: This case highlights the diagnostic challenges of extramedullary plasmacytomas and the potential efficacy of CD38-targeted therapy.
Keywords: Extramedullary plasmacytoma; Pancreatic plasmacytoma; Daratumumab; Pancreatic tumor; Lenalidomide; CD38-targeted therapy; Dual-site plasmacytoma; Radiotherapy; Multiple myeloma; Monoclonal plasma cells.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Seif S (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Seif S, Assi A, Khazen R, Kourie HR, Ghorayeb H, et al. Novel use of daratumumab in a rare dual plasmacytoma of the humerus and pancreas: A case report. Open J Clin Med Case Rep. 2025; 2390.
Introduction
Solitary Plasmacytoma (SP) is a rare plasma cell neoplasm that accounts for less than 5% of all plasma cell dyscrasias. It presents as a localized clonal proliferation of plasma cells, classified into Solitary Bone Plasmacytoma (SBP) when affecting bone and Extramedullary Plasmacytoma (EMP) when confined to soft tissue. SBP predominantly arises in red marrow-containing bones, such as the vertebrae, ribs, and pelvis, while EMP commonly affects the head and neck region, respiratory tract, and gastrointestinal system. The primary symptom is often localized pain, but neurological deficits may occur due to compression effects. Although SP is a distinct clinical entity, a significant proportion of cases—up to 76% of SBP and 36% of EMP—progress to Multiple Myeloma (MM) over time, making long-term monitoring essential.
Radiotherapy is the cornerstone of treatment for SP, with high local control rates exceeding 80%. While chemotherapy is not routinely used, emerging data suggest potential benefits in select high-risk patients. The prognosis of SP varies, with the risk of progression to MM being influenced by factors such as minimal bone marrow involvement and lesion size. Given its rarity and variable disease course, SP requires a multidisciplinary approach to optimize outcomes.
This case report presents a unique instance of a patient diagnosed with simultaneous plasmacytomas in the humerus and pancreas, exploring the clinical presentation, diagnostic modalities, treatment approaches, and outcomes. Notably, this is the first reported case treated with Daratumumab, marking a novel therapeutic approach in this context. By detailing this uncommon manifestation, this report expands the understanding of plasmacytoma’s variability and highlights the importance of thorough investigation in cases of multifocal disease, ultimately contributing to improved management strategies for affected patients.
Case Presentation
A 69-year-old male with a significant medical history, including liposarcoma treated with surgery and radiotherapy, hypertension, cardiac arrhythmia, total thyroidectomy, and two previous surgeries for discal hernia, presented with new onset of musculoskeletal symptoms following a fall. The fall resulted in a shoulder fracture, which was surgically repaired, and the patient subsequently underwent multiple sessions of physiotherapy for rehabilitation.
During the recovery period, the patient noted the gradual onset of a cutaneous lesion on the right humerus, which progressively enlarged. Concerned by the change in the lesion’s characteristics, the patient underwent a CT scan, which revealed a suspicious expansive lytic mass located in the central right diaphysis of the humerus. The mass measured 2.5 cm by 3.5 cm transversely and extended over 8 cm in height. Radiologic findings showed posterior cortical erosion and an irregular periosteal reaction, raising concerns for a possible malignant etiology. Furthermore, the mass exhibited extension into the adjacent local and regional soft tissues, including the surrounding musculature.
Given the unusual characteristics of the mass, a biopsy of the lesion was performed. Histopathological examination revealed a monoclonal plasmocytic proliferation, which was consistent with a diagnosis of plasmacytoma. The monoclonal nature of the plasma cells and the absence of other distinguishing features of multiple myeloma prompted further investigation for possible systemic involvement.
To comprehensively assess the patient’s condition, a PET-CT scan was performed (september 2024). This imaging modality revealed an additional suspicious mass in the pancreas, which had not been identified on prior imaging studies.
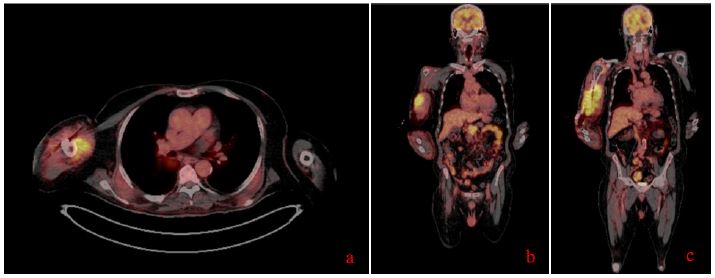
Figure 1: (A-C) Different sections of the patient’s PET CT scan showing an extensive, intensely hypermetabolic tissue lesion in the pancreatic head, along with a large, intensely hypermetabolic skeletal muscle lesion on the right side, with associated humeral involvement.
Given the unusual location and the patient’s clinical presentation, the pancreatic lesion was further evaluated using Endoscopic Ultrasound (EUS) with Fine Needle Aspiration (FNA). The pathological findings from the EUS-guided biopsy confirmed the diagnosis of Pancreatic Plasmacytoma (PP).
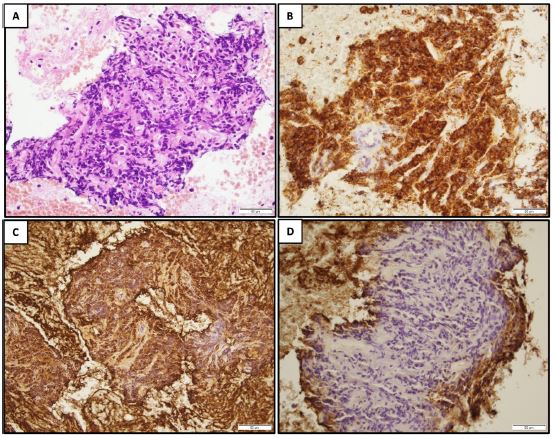
Figure 2: The proliferation is composed of atypical plamacytoid cells with hyperchromatic nuceli (A HE x400). CD138 highlights the plasma cells (B), which show a monoclonal pattern of kappa light chain expression (C). Lambda light chains are negative (D).
The patient was diagnosed with both skeletal and pancreatic plasmacytoma. Given the dual site involvement and the monoclonal nature of the disease, treatment with daratumumab, a monoclonal antibody targeting CD38, was initiated. Daratumumab has been shown to have significant efficacy in treating plasma cell malignancies, including relapsed and refractory multiple myeloma and extramedullary plasmacytomas.
The patient demonstrated a significant clinical improvement following 3 weeks of the initiation of daratumumab and lenalidomide therapy. Serial imaging studies, done in january 2025, showed a marked reduction in the size of both the humeral and pancreatic masses, with complete resolution of the lytic bone lesion and near-total disappearance of the pancreatic mass. These findings were corroborated by clinical evaluation, with the patient reporting resolution of symptoms such as pain and swelling at the site of the previous humeral mass.
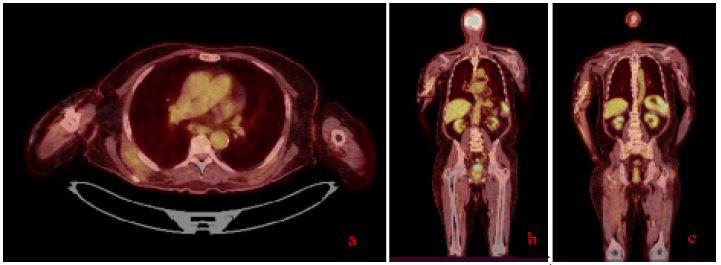
Figure 3: (A-C) Different sections of the patient’s follow up PET CT scan (January 2025) showing a complete morpho-metabolic remission of the large intensely hypermetabolic tissue mass in the pancreatic head and complete metabolic remission of the large intensely hypermetabolic skeletal muscle tissue mass in the right arm with humeral involvement, described on the PET scan of September 30, 2024.
As of the latest follow-up, the patient continues to show complete morpho-metabolic remission, with no new hypermetabolic lesions identified on PET-CT since January 2025.
Discussion/Conclusion
Plasmacytoma is a plasma cell disorder in which a plasma cell tumor emerges from the axial bones or from soft tissue [1].
The International Myeloma Foundation classifies plasmocytomas into three distinct entities: Extramedullary Plasmacytoma (EMP), Solitary Plasmacytoma of Bone (SPB), and primary or recurrent multiple plasmacytomas [1]. SPB is the most frequent, making up 3 to 5% of all plasma cell cancers [2]. SPBs appear as lytic spots in the axial skeleton, whereas EMPs can develop in any soft tissue, but are more common in the upper part of the respiratory system and the gastrointestinal tract (approximately 85% and 10%, respectively) [3,4]. SBP and EMP differ from MM in a few key aspects; namely a single location, monoclonal plasma cells accounting for fewer than 5% of the bone marrow cellularity. Also, SBP and EMP usually present with low paraprotein and without end-organ dysfunction [1].
SBPs often present with bone pain, pathological fractures, and compression of the medulla in instances of vertebral SBP [5]. Radiologic findings usually show defined osteolytic defects without substantial sclerosis. Computed Tomography (CT) scan usually shows a slightly expansive lytic lesion with possible cortex disuptions. Contrast enhanced CT shows homogenous enhancement of the lesion. Magnetic resonance imaging may reveal a hypointense lesion on T1-weighted sequences and a hyperintense lesion on SBPs often present with bone pain, pathological fractures, and compression of the medulla in instances of vertebral SBP [5]. Radiologic findings usually show defined osteolytic defects without substantial sclerosis. Computed Tomography (CT) scan usually shows a slightly expansive lytic lesion with possible cortex disuptions. Contrast enhanced CT shows homogenous enhancement of the lesion. Magnetic resonance imaging may reveal a hypointense lesion on T1-weighted sequences and a hyperintense lesion on T2-weighted sequences [6]. SPBs are histologically composed of monoclonal plasma cell sheets, with positive staining for CD38 and CD138 on immunohistochemistry [7].
EMP, when symptomatic, presents with the symptoms of a local mass in the upper respiratory or digestive tract, such as pain, congestion, dyspnea, epistaxis, dysphagia, hoarseness, and even diplopia in instances of orbital EMP [4,8,9]. EMP appears as an infiltrative lesion exhibiting soft tissue attenuation on CT imaging. T1- and T2-weighted MRI shows EMP as isointense and hyperintense, respectively. Both CT and MRI commonly demonstrate moderate to intense contrast enhancement of the lesion [9]. EMP evolves to MM in 20% to 30% of cases, especially in patients older than 50 and in patients with an EMP mass exceeding 4 cm [10].
PP is extremely rare and manifests as a primary neoplasia, or as a secondary lesion to MM. It mostly develops in the head of the pancreas, and is thus extremely challenging to distinguish from other pancreatic tumors [11].
From a clinical perspective, PP may resemble primary pancreatic tumors. Symptoms may include epigastric discomfort, jaundice, and weight loss owing to the occlusion of the bile duct or duodenum [12].
The radiological findings of pancreatic plasmocytoma are not particularly specific. Ultrasonography shows a heterogeneous, hypoechoic mass compared to neighboring tissue. CT reveals homogenous enhancement of a multilobulated mass. Diffuse pancreas hypertrophy is frequently noted [13]. PET-CT offers a morpholigic and functional assessment of a lesion, and is thus well-suited for determining the location and size of the metabolically active plasma cells within and outside of the bone marrow. PET-CT is therefore the ideal for detecting MM and EMP. MRI is another suitable imaging technique, and usually shows PP lesions as hyperintense on T2-weighted MRI and hypointense on T1-weighted sequences. MRI also allows for an accurate assessment of surrounding structures, such as the common or pancreatic bile ducts, the celiac trunk, and portal vein [11].
All these imaging modalities are not sufficient alone to prove the nature of the lesion and to guide the clinicians to a plasmocytoma diagnosis due radiologic resemblance to primary pancreatic malignancies.
EUS-guided fine needle biopsy is a safe and effective diagnostic modality for identifying the nature of pancreatic masses. It allows for a sufficient tissue sampling to perform IIHC. IHC must exhibit positivity for plasma cell markers such as CD38, heavy or light chains in a monoclonal fashion in order to confirm a plasma cell neoplasm [11].
Pancreatic plasmacytoma is an exceedingly rare entity with no standardized treatment approach, largely due to its infrequent presentation and the potential for systemic involvement [14]. Management typically relies on a multimodal strategy, leveraging the known radiosensitivity and chemosensitivity of plasma cell tumors. While surgical resection—such as distal pancreatectomy—may be considered in highly selected patients with localized disease in the pancreatic tail, it is generally avoided in cases of bulky tumors or those with high risk for dissemination. Due to its high radiosensitivity, radiotherapy remains the cornerstone of treatment, particularly with the use of modern techniques such as Intensity-Modulated Radiation Therapy (IMRT), which has demonstrated excellent local control with minimal toxicity. Mounting evidence supports the integration of systemic therapy with radiotherapy in order to address potential occult disease and delay progression to Multiple Myeloma (MM) [2]. Notably, the addition of agents such as lenalidomide-dexamethasone to IMRT has been associated with improved progression-free and MM-free survival. Similarly, proteasome inhibitors like bortezomib and monoclonal antibodies such as daratumumab have shown promising outcomes in select cases, including sustained tumor remission. Although the current data is heterogeneous and largely based on retrospective analyses and case reports, a trend favoring combined modality therapy—particularly in high-risk or extramedullary disease—has emerged. Thus, the optimal management of pancreatic plasmacytoma likely involves tailored, multidisciplinary treatment incorporating radiotherapy and systemic agents, especially in cases with aggressive features or high likelihood of systemic progression.
The distinguishing feature of our case is the occurrence of Extramedullary Plasmacytomas (EMPs) involving both the pancreas and humerus, without any clinical or laboratory evidence of multiple myeloma (MM) at any point during the disease course. This is a highly unusual presentation. A review of previously published reports identified only a small number of comparable cases of multifocal or recurrent EMPs without MM [15-19]. These cases, involving sites such as the chest wall, breast, orbit, retroperitoneum, and testis, illustrate the broad anatomical range that EMPs can affect in the absence of systemic disease. However, to our knowledge, none of these reports have described involvement of the pancreas or humerus, making our case an important addition to the existing clinical spectrum of EMPs without MM.
Treatment strategies in those cases have included local radiotherapy, conventional chemotherapy (often incorporating agents like bortezomib, thalidomide, or melphalan), and surgical interventions, with variable clinical outcomes ranging from complete remission to early mortality due to complications such as infection or organ failure.
In contrast, our patient was treated with daratumumab. This choice reflects a shift toward more targeted therapies, even in the absence of systemic MM.
Daratumumab is a human anti-CD38 monoclonal antibody that exerts its antitumor effects through multiple mechanisms, including direct cytotoxicity, Antibody-Dependent Cellular Cytotoxicity (ADCC), Complement-Dependent Cytotoxicity (CDC), and immunomodulation via depletion of CD38+ regulatory cells. CD38 is widely expressed on plasma cells, including those in most plasma cell neoplasms, making it a rational therapeutic target even in extramedullary settings [20]. While daratumumab monotherapy has generally shown limited efficacy in extramedullary disease [21], we observed an exceptional and sustained response in our patient with solitary extramedullary plasmacytoma, suggesting that in selected cases—particularly when CD38 expression is preserved—daratumumab alone may offer meaningful benefit. To the best of our knowledge, no prospective therapeutic studies have been specifically dedicated to patients with Extramedullary Myeloma (EMM), making it difficult to recommend one strategy over another [22]. Nevertheless, de novo EMM is considered a high-risk entity, and experts recommend aggressive treatment when possible. Data from trials such as the CASSIOPEIA study have reinforced the role of monoclonal antibodies, including daratumumab, in frontline therapy for transplant-eligible patients, although dedicated evaluation in the EMM population remains limited.
Given the limited data on such presentations, especially involving pancreatic or humeral sites, our experience highlights both the diagnostic challenge and evolving therapeutic landscape in managing EMPs without MM.
References
- Kyle RA, Child JA, Anderson K, et al. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Br J Haematol. 2003;121:749-757.
- Soutar R, Lucraft H, Jackson G, et al. Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma. Br J Haematol. 2004;124:717-726.
- Roh YH, Hwang SY, Lee SM, et al. Extramedullary plasmacytoma of the pancreas diagnosed using endoscopic ultrasonography-guided fine needle aspiration. Clin Endosc. 2014;47:115.
- Weber DM. Solitary bone and extramedullary plasmacytoma. Hematology. 2005;2005:373-376.
- Frassica DA, Frassica FJ, Schray MF, Sim FH, Kyle RA. Solitary plasmacytoma of bone: Mayo Clinic experience. Int J Radiat Oncol Biol Phys. 1989;16:43-48.
- Wang Y, Zhu XL, Peeroo MW, et al. Pelvic solitary plasmacytoma: computed tomography and magnetic resonance imaging findings with histopathologic correlation. Korean J Radiol. 2015;16:146-153.
- Pucca MB, Brito-Souza PA, Alexandre-Silva GM, Oliveira ACS, Tavares Mesquita K, Soares Cardoso L. Exploring solitary bone plasmacytoma: a rare case report. Int J Clin Case Rep Rev. 2021;9:1-6.
- Zhu X, Wang L, Zhu Y, et al. Extramedullary plasmacytoma: long-term clinical outcomes in a single-center in China and literature review. Ear Nose Throat J. 2021;100:227-232.
- Ching ASC, Khoo JBK, Chong VFH. CT and MR imaging of solitary extramedullary plasmacytoma of the nasal tract. AJNR Am J Neuroradiol. 2002;23:1632.
- Wen G, Wang W, Zhang Y, Niu S, Li Q, Li Y. Management of extramedullary plasmacytoma: role of radiotherapy and prognostic factor analysis in 55 patients. Chin J Cancer Res. 2017;29:438-446.
- Le M, Surapaneni BK, Jain V, Vinayek R, Dutta SK. Pancreatic extramedullary plasmacytoma presenting as a pancreatic mass. Clin Med Insights Gastroenterol. 2018;11:1179552218801603.
- Da Silva RL. Pancreatic involvement by plasma cell neoplasms. J Gastrointest Cancer. 2012;43:157-167.
- Hatem M, So B, Gray R, Wong J. Plasmocytoma presented as pancreatic head mass. Radiol Case Rep. 2015;10:81-87.
- Rizk RC, Weisberg EM, Fishman EK. Solitary plasmacytoma of the pancreas: a rare case report. Radiol Case Rep. 2024;19:1806-1809.
- Hussain A, Singh M, Singh K, Bagga H. Multiple extramedullary plasmacytoma with lytic bony lesions: a rare case report. Case Rep Med. 2013;2013:291359.
- Anukanchanavera T, Kaewsathorn C, Kiranantawat N. Endobronchial mass: a rare manifestation of multiple solitary plasmacytoma. J Belg Soc Radiol. 2023;107.
- Ahnach M, Marouan S, Rachid M, et al. Extramedullary plasmocytoma relapsing at different sites: an unusual presentation. Pan Afr Med J. 2013;14.
- Raghuram S, Faizal B, Sanjeevan KV, et al. Recurrent extramedullary plasmacytomas without multiple myeloma: a case report with review of the literature. Cancer Treat Res Commun. 2022;31:100550.
- Aznab M, Khazaei M. Multifocal extramedullary and multiple solitary bone plasmacytoma: a case report and review of the literature. Int J Cancer Manag. 2019;12.
- De Novellis D, Zeppa P, Maffei E, Giudice V, Selleri C, Serio B. Efficacy of daratumumab-based regimens for extramedullary pulmonary plasmacytoma: a case report. Cancer Rep. 2024;7.
- Moreno DF, Clapés V, Soler JA, et al. Real-world evidence of daratumumab monotherapy in relapsed/refractory multiple myeloma patients and efficacy on soft-tissue plasmacytomas. Clin Lymphoma Myeloma Leuk. 2022;22:635-642.
- Touzeau C, Moreau P. How I treat extramedullary myeloma. Blood. 2016;127:971-976.
