
Open Access, Volume 11
Integrated pathology and interventional diagnostic approach to a metastatic grade 1 pancreatic neuroendocrine tumour: A case report of diagnostic delay in a low-resource setting
Oluwaseun T Babalola1-3; Stephanie Y Damitan4,5*
1General Practice, NHS Greater Glasgow and Clyde, United Kingdom.
2Rehabilitation Medicine, NHS Education for Scotland, United Kingdom.
3Clinical Director, Phils Health Plus, Abuja, Nigeria.
4Elderly and Rehabilitation Volunteer, NHS Greater Glasgow and Clyde, United Kingdom.
5Clinical Advisor and Consultant, Phils Health Plus, Nigeria.
Stephanie Y Damitan
Elderly and Rehabilitation Volunteer, NHS Greater Glasgow and Clyde, United Kingdom.
Email: stephii.damitan@gmail.com
Received : September 03, 2025,
Accepted : October 22, 2025
Published : October 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Background: Pancreatic Neuroendocrine Tumours (PanNETs) are rare neoplasms that often go unrecognised or misdiagnosed due to nonspecific symptoms and slow growing nature. Timely diagnosis relies on integrated pathway linking clinical suspicion with targeted markers, high-quality imaging, and minimally invasive tissue acquisition for pathology to confirm lineage and grade before therapy. Apart from poor clinical recognition, diagnosis delays in Low- and Middle-Income Countries (LMICs) are often related to limited diagnostic capacity, including pathology and biochemical testing, subspecialty imaging, interventional expertise, and reliance on invasive procedures such as open surgical biopsies.
Case presentation: A 72-year-old woman from Nigeria with over six years history of epigastric and lower abdominal pain, chronic diarrhoea, early satiety, and weight loss. She has no other significant past medical history. Early care in several public and private hospitals emphasised empiric treatment for dyspepsia, malaria, or enteric infections despite negative investigations. Serial imaging studies over the years revealed inconsistent radiological interpretations of growing retroperitoneal mass with hepatic involvement. Despite multiple healthcare visits, no definitive diagnosis was made, as minimally invasive biopsy techniques were unavailable, and open surgical biopsy was declined by the patient due to her age and surgical risks. In August 2024, Ultrasound-guided core biopsy by a private interventional radiologist yielded only necrotic, poorly preserved carcinoma; a second review reported “necrotic neoplasm.” During a family visit in early 2025, at a South African tertiary center, biochemical testing showed markedly elevated 24-hour urinary 5-Hydroxyindoleacetic Acid (5-HIAA) and chromogranin A after dietary/medication restrictions, supporting a serotonin-producing process. Imaging revealed a bulky retroperitoneal mass abutting the pancreatic head with multiple liver and nodal metastases. EUS-guided fine-needle biopsy of the pancreatic head lesion obtained cores and smears. Cytology showed monomorphic cells with scant cytoplasm and finely granular “salt-and-pepper” chromatin. IHC demonstrated diffuse synaptophysin and CgA positivity with pan-cytokeratin expression; Ki-67 was <2%, consistent with a well-differentiated Grade 1 PanNET. She was started on Octreotide LAR and reported significant symptom improvement, including weight gain from 47 kg to 54 kg within three months.
Discussion: Poor clinical suspicion, limited subspecialty access (limiting options to high-risk open surgical biopsies), and inconsistent imaging readings prolonged diagnosis. Large, heterogeneous tumours are often necrotic, lowering the yield of blind percutaneous sampling; targeted EUS-guided biopsy of viable regions overcame this. The paradox of a low-grade tumour with widespread metastases further complicated diagnosis. Pathology ultimately played the pivotal role in identifying the tumour type, enabling appropriate treatment.
Conclusion: PanNETs should be suspected in patients with chronic gastrointestinal symptoms, weight loss and unexplained retroperitoneal masses. Minimal invasive interventional tissue biopsy and pathology remains the cornerstone of PanNETs diagnosis.This case underscores the need to improve clinical recognition of neuroendocrine tumours, and expand minimally invasive diagnostic capabilities in LMICs, in addition to strengthening pathology infrastructure and multidisciplinary collaboration.
Keywords: Pancreatic neuroendocrine tumour; Endoscopic ultrasound-guided biopsy; Chromogranin A; Immunohistochemistry; 5-hydroxyindoleacetic acid; Low-resource setting; Multidisciplinary care approach.
Abbreviations: GEP-NEN(s): Gastroenteropancreatic Neuroendocrine Neoplasm(s); PanNET(s): Pancreatic neuroendocrine tumour(s); NET(s): well-differentiated Neuroendocrine tumour(s); WHO: World Health Organization; EUS: Endoscopic Ultrasound; FNA: Fine-Needle Aspiration; FNB: Fine-Needle Biopsy; IHC: Immunohistochemistry; CgA: Chromogranin A; 5-HIAA: 5-Hydroxyindoleacetic Acid; SSTR: Somatostatin Receptor; PRRT: Peptide Receptor Radionuclide Therapy; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; PET/CT: Positron Emission Tomography/Computed Tomography; FDG: Fluorodeoxyglucose; SMA: Superior Mesenteric Artery; ECOG: Eastern Cooperative Oncology Group; LMIC(s): Low- and Middle-Income Country(ies); PPI(s): proton-pump inhibitor(s).
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Damitan SY (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Babalola OT, Damitan SY. Integrated pathology and interventional diagnostic approach to a metastatic grade 1 pancreatic neuroendocrine tumour: A case report of diagnostic delay in a low-resource setting. Open J Clin Med Case Rep. 2025; 2389.
Introduction
Pancreatic Neuroendocrine Tumours (PanNETs) are uncommon neoplasms, and constitute a small fraction of pancreatic neoplasms yet remain clinically important within the spectrum of Gastroenteropancreatic Neuroendocrine Neoplasms (GEP-NEN). Contemporary classification frameworks (WHO 2017 and 2022) define well-differentiated neuroendocrine tumours by characteristic morphology and an immunophenotype that includes synaptophysin and Chromogranin A (CgA) positivity, with grade assigned by mitotic rate and Ki-67 index; Grade 1 is defined by a low proliferative fraction (Ki-67< 3%). These standards enable consistent diagnosis and prognostication across centers [1]. Consensus clinical practice guidelines (ESMO, ENETS) recommend an integrated diagnostic pathway that links clinical suspicion with targeted biochemical testing, high-quality cross-sectional imaging, and minimally invasive tissue acquisition to confirm to confirm histology and grade before treatment [2,3]. Management recommendations for metastatic well differentiated GEP-NETs further emphasize symptom control and disease stabilization with somatostatin analogs, with additional options for progressive disease [4].
Imaging characteristics or features of PanNETs are heterogeneous and depend on size, grade, and vascularity. On multiphasic CT/MRI, well-differentiated tumours often demonstrate arterial hyperenhancement and may calcify; larger lesions commonly exhibit necrosis and cystic change, which complicates interpretation and can reduce biopsy yield if non-viable areas are sampled [5,6]. Functional imaging refines staging and treatment planning. Somatostatin receptor (SSTR)-based PET/CT, most commonly using 68Ga-DOTATATE, improves detection of primary and metastatic disease, guides suitability for Peptide Receptor Radionuclide Therapy (PRRT), and can outperform conventional imaging in well differentiated tumours [7]. By contrast, FDG PET/CT is variably informative in PanNETs; its utility increases with higher grade and proliferative activity, whereas well-differentiated, indolent disease may demonstrate limited avidity [8].
Ultimately, tissue diagnosis remains the linchpin. EUS-guided fine-needle aspiration or biopsy enables sampling of pancreatic masses, allows Ki-67 evaluation on cell blocks or cores, and achieves high diagnostic accuracy, with emerging data favouring fine-needle biopsy for cellularity and reproducible grading in selected scenarios [9,10]. Biochemical markers provide complementary evidence. Plasma Chromogranin A (CgA) correlates with tumour burden in many NETs but is susceptible to false positives from proton-pump inhibitors, renal impairment, and other factors; therefore, assays must be interpreted in clinical context and, when necessary, repeated after mitigation of confounders [11]. For suspected serotonin-producing tumours, 24-hour urinary 5-Hydroxyindoleacetic Acid (5-HIAA) remains a standard test; adherence to dietary and medication restrictions, such as avoidance of serotonin-rich foods and certain drugs, reduces false positives [2,3,11]. Population-based data describe incidence and survival patterns for PanNETs and support the prognostic role of grade and stage [12].
Despite clear guidance, real-world care often diverges. Multiple studies document diagnostic delays and initial misattribution of symptoms to common gastrointestinal conditions, particularly where access to subspecialty imaging, interventional endoscopy, and Immunohistochemistry (IHC) is limited [13,14]. Health-system constraints in Low- and Middle-Income Countries (LMICs), including gaps in multiphasic CT/MRI, underutilisation of nuclear medicine, and limited availability of Endoscopic Ultrasound (EUS) or image-guided biopsy, can transform a potentially straightforward work-up into a prolonged diagnostic odyssey [15-17].
This case from a low-resource setting illustrates how low initial clinical suspicion, constrained access to advanced diagnostics, and variable radiologic interpretations prolonged the diagnostic journey. It also shows how an integrated pathway; combining biomarkers, high-quality imaging, EUS-guided tissue acquisition, and expert IHC, enabled definitive diagnosis and appropriate therapy in line with contemporary guidance, while highlighting system-level opportunities to shorten time to diagnosis and improve patient experience [1-4]. The Lancet Oncology Commission calls for strategic investment in imaging and nuclear medicine to close these access gaps [18], and regional reports highlight diagnostic delays specific to West Africa [19].
Case Presentation
The patient was a 72-year-old woman from Nigeria with a history notable for more than six years of intermittent epigastric and lower abdominal pain, loose stools, early satiety, and progressive unintentional weight loss. She has no other significant past medical history. She first sought care in 2018 and was treated empirically for dyspepsia with proton-pump inhibitors and antibiotics without prior Helicobacter pylori testing. At other times she received antimalarials and antibiotics for presumed enteric fever despite negative investigations. Routine laboratory testing during these early encounters was essentially unremarkable and contributed to a false sense of reassurance for both clinicians and patient. By January 2019 she weighed 63 kg, although earlier baseline weights had not been recorded. In late 2019, an abdominal ultrasound was obtained and reported hepatomegaly and uterine enlargement with a possible left iliac fossa mass, findings considered non-specific. In early 2020 she was admitted to a teaching hospital for worsening abdominal pain. Despite inpatient evaluation, no unifying diagnosis was made, and she was discharged on symptomatic therapy. Over the subsequent months she developed a pattern of postprandial discomfort and a conditioned fear of eating due to pain, with intermittent diarrhoea and gradual weight loss.
Prompted by a medically trained relative, she underwent contrast-enhanced CT of the abdomen and pelvis in mid-2021 at a private facility. This showed a 7.2×4.5 cm retroperitoneal mass inferior to the head of the pancreas, an enlarged liver with a caudate lobe lesion measuring approximately 4.2×3.5 cm, and an incidental right adnexal complex cystic mass about 5 cm. The radiologist favoured a primary retroperitoneal tumour such as a soft-tissue sarcoma or a neurogenic neoplasm, with a solitary hepatic metastasis, and considered the ovarian lesion likely unrelated. Although the constellation of a pancreatic region mass and a liver lesion was compatible with a neuroendocrine tumour, this possibility was not actively pursued by the treating team at that time. General surgeons at a federal teaching hospital recommended an open exploratory laparotomy with surgical biopsy, citing the complexity of the findings and the lack of local percutaneous biopsy capability. No tumour markers were ordered, and the patient was not referred to a center offering image-guided biopsy. After discussion, she declined an open surgical biopsy due to age and operative risk. A conservative “watch-and-wait” approach was adopted because pain was partly controlled and her functional status remained acceptable. By December 2021 her weight was 56 kg.
Throughout 2022 the patient continued to seek outpatient care at state and teaching hospitals for persistent symptoms. Management remained largely symptomatic with analgesics and anti-diarrhoea medications. In December 2022 she acutely collapsed with transient loss of consciousness and was taken to the emergency department. Laboratory evaluation revealed marked hyponatremia, hypokalaemia, and hypocalceamia. These disturbances were corrected with intravenous therapy and were attributed to chronic diarrhoea and poor intake. A repeat contrast-enhanced CT at that time was reported as showing a large necrotic mass in the caudate lobe of the liver, approximately 5×7 cm, with extension toward the retroperitoneum. The study was interpreted as hepatocellular carcinoma with atypical retroperitoneal metastasis, a conclusion discordant with the 2021 CT which had favoured a primary retroperitoneal mass. This disagreement underscored how interpretations can vary when subspecialty radiologic expertise is limited. The surgical clinic again advised open biopsy for definitive diagnosis, which the patient declined.
In early 2023, ultrasound at a private diagnostic center identified het-“ masses het-”: heterogeneous para-umbilical/right iliac fossa mass measuring about 7.7×7.3 cm and another epigastric mass approximately 4.7×3.8 cm. These likely corresponded to the known retroperitoneal disease and a component near the pancreatic head. In late 2023, a third CT of the chest, abdomen, and pelvis demonstrated an enhancing isodense lesion in the region of the pancreatic head and caudate lobe measuring about 5.3×5.8 cm, surrounded by smaller satellite lesions suggestive of metastases. There was also an 11×5.8 cm right para-aortic retroperitoneal mass encasing branches of the superior mesenteric artery. Multiple enlarged abdominal lymph nodes were present. The differential diagnosis included a soft-tissue sarcoma, a germ cell tumour, and a neurogenic tumour. An enlarged uterus was noted, and a filling defect in the cecum was mentioned without accompanying colonic symptoms. Throughout 2023, symptoms remained dominated by abdominal pain, early satiety, and intermittent diarrhoea with progressive fatigue and recurrent electrolyte disturbance attributable to diarrhoea and malnutrition. By mid-2024, a fourth CT demonstrated further progression with a retroperitoneal mass measuring about 11×10×8.4 cm encasing the abdominal aorta and both common iliac arteries; a necrotic caudate lobe lesion and additional right hepatic lesions; and diffuse nodal disease. The radiology impression favoured lymphoma or another malignancy with bulky nodal involvement and retroperitoneal metastasis. Seeking a tissue diagnosis, the patient presented to a private specialist oncologic hospital where a multidisciplinary team, including an interventional radiologist reviewed the case. Given the extensive vascular encasement and high operative risk, the team recommended image-guided needle biopsy rather than open surgery as earlier pursued by the Federal teaching hospital.
In August 2024, ultrasound-guided core needle biopsy of an accessible anterior component of the mass near the pancreatic head was performed under local anaesthesia, with four cores obtained uneventfully. Histopathology reported a poorly differentiated carcinoma with extensive necrosis and poor preservation, limiting classification. Immunohistochemistry was non-contributory. A second opinion described only oncol-“ oncology team agreed that a repeat biopsy targeting viable tissue would be required for definitive diagnosis. The patient, having recently undergone an invasive procedure with limited yield, declined further percutaneous sampling at that time. She was managed supportively with analgesics, including low-dose morphine for chronic pain, nutritional support, and electrolyte monitoring. Her performance status remained ECOG 1-2 with analgesia, but she continued to lose weight and experienced significant pain and diarrhoea; by late 2024 she weighed 47 kg.
In early 2025 she traveled to South Africa to visit family, who facilitated evaluation at a private tertiary center with comprehensive neuroendocrine diagnostics. Biochemical testing demonstrated striking abnormalities: a markedly elevated 24-hour urinary 5-HIAA and a plasma CgA of 746 ng/L (local reference < 100 ng/L). She had received counselling to avoid serotonin-rich foods and interfering medications prior to collection, and there was no renal dysfunction or proton-pump inhibitor use to confound interpretation [2,3,11]. These results aligned with her chronic diarrhoea and suggested a functioning NET with serotonin production.
An updated CT of the abdomen and pelvis at the tertiary center confirmed the presence of large conglomerate nodal masses in the retroperitoneum from L4 to S1 (approximately 5.5 cm craniocaudal, 5.4 cm transverse, 3.7 cm anteroposterior), displacing and encasing the aorta and common iliac arteries. A separate large mesenteric soft-tissue mass approximately 12 cm in maximal dimension contained coarse calcifications and abutted the head of the pancreas while encircling the portal vein, which remained patent. Multiple liver lesions were present, with the largest in the caudate lobe measuring approximately 5 cm and demonstrating central necrosis; additional right lobe lesions measured up to about 2 cm. No lesions were seen in the spleen, kidneys, or lungs. The pancreas and stomach were displaced by the mass but maintained clear planes of separation. The overall impression favoured a metastatic neuroendocrine neoplasm in light of the biochemical profile; lymphoma remained in the differential.
Endoscopic ultrasound was carried out which identified a pancreatic head lesion amenable to tissue sampling (Figure 1). EUS-guided fine-needle biopsy provided multiple tissue cores and cytology smears. Cytology showed highly cellular samples with clusters and trabeculae of monomorphic tumour cells with scant cytoplasm and round-to-oval nuclei displaying finely granular “salt-and-pepper” chromatin; nucleoli were inconspicuous, mitotic figures were not observed, and no necrosis was identified in the sampled material. Cell-block preparation enabled immunocytochemistry and histology on core sections. Immunohistochemistry demonstrated diffuse positivity for synaptophysin and chromogranin A, confirming neuroendocrine differentiation. Tumour cells were positive for pan-cytokeratin, supporting epithelial lineage and helping exclude mesenchymal or lymphoid mimics. The Ki-67 proliferation index was quantified at less than 2%, consistent with a well-differentiated Grade 1 NET according to WHO criteria (Figure 2) [1,9,10].
With a definitive diagnosis established, the patient commenced long-acting Octreotide (Octreotide LAR) in 2025, consistent with guideline-recommended first-line therapy for metastatic well-differentiated GEPNETs aimed at symptom control and disease stabilisation [2,3]. Over subsequent months, she experienced reduced stool frequency, improved appetite, recognition of fewer flushing episodes in retrospect, stabilisation of electrolyte disturbances, and improved pain control. Her weight increased from 47 kg to 54 kg. She continues on monthly injections with clinical monitoring. Further therapy such as liver-directed approaches, targeted agents, or peptide receptor radionuclide therapy was reserved pending clinical course, somatostatin receptor imaging access, and multidisciplinary discussion [4,7].
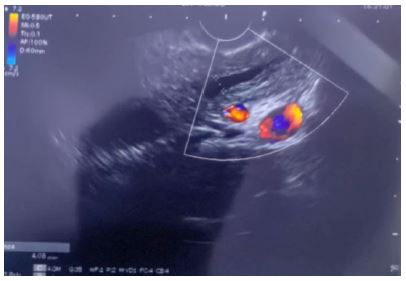
Figure 1: Endoscopic Ultrasound (EUS) still frame of the pancreatic head mass. The lesion is visualized adjacent to the portal venous confluence with internal vascular signals on color Doppler (red/blue), consistent with a hypervascular solid mass amenable to EUS-guided fine-needle biopsy.
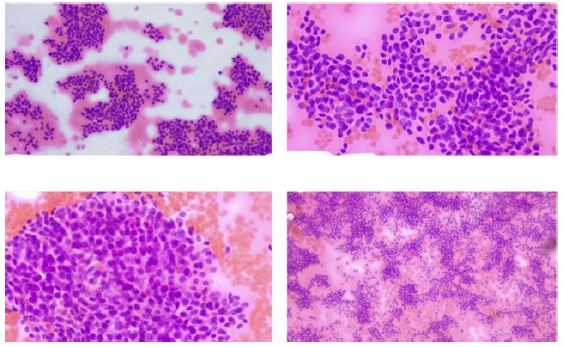
Figure 2: Representative cytology and immunocytochemistry patient report from the EUS-guided sampling. Smears show cohesive nests and trabeculae of uniform tumour cells with scant cytoplasm and finely granular “salt-and-pepper” chromatin. Cell-block immunostains demonstrate diffuse synaptophysin and chromogranin A positivity; Ki-67 labelling is virtually absent (< 2%), supporting a well-differentiated Grade 1 pancreatic neuroendocrine tumour.
Discussion
This case underscores how non-specific gastrointestinal symptoms, constrained access to subspecialty diagnostics, and variable radiologic expertise can converge to delay diagnosis of neuroendocrine tumours in LMIC settings. Although contemporary classification systems and guidelines provide clear frameworks for lineage confirmation, grading, and treatment selection, real-world implementation depends on service availability and referral networks [1-4]. As described in several series, many patients cycle through empiric therapies and fragmented evaluations before NETs are entertained, leading to prolonged morbidity and avoidable complications [13,14,19]. Our patient manage-’ management focused on common conditions, early imaging was limited and variably interpreted, and the absence of minimally invasive biopsy capability delayed tissue confirmation.
Clinical suspicion remains the critical first step. Persistent epigastric pain, chronic diarrhoea, and unintentional weight loss without laboratory explanation should prompt timely imaging and, when masses are identified, focused evaluation for neuroendocrine aetiologies. Structured triggers, such as recurrent diarrhoea with abdominal masses or unexplained weight loss with hypervascular lesions can help clinicians consider NETs earlier and request appropriate tests consistent with ESMO/ENETS recommendations [2-4].
The imaging pathway and sampling pitfalls deserves emphasis. Well-differentiated PanNETs frequently appear hypervascular and may calcify; large lesions often contain necrosis and cystic change, which can both obscure typical enhancement patterns and reduce the yield of percutaneous sampling if non-viable areas are inadvertently targeted [5,6]. Discordant reads in our case, from a retroperitoneal soft-tissue tumour to presumed hepatocellular carcinoma with atypical spread, illustrate the impact of reader variability and the value of subspecialty review or tumour board discussion. SSTR PET/CT improves detection of occult disease, informs suitability for peptide receptor radionuclide therapy, and can refine staging beyond CT or MRI in well-differentiated tumours. Whereas FDG PET/CT is variably sensitive in PanNETs and is most helpful in higher-grade or dedifferentiated disease, integrating both modalities can support comprehensive biologic characterisation when available [7,8]. Unfortunately, access to such technologies is uneven, and studies from Nigeria and the broader region document underutilisation of nuclear medicine services despite clinical need [15-18].
Tissue diagnosis is indispensable and should follow the least invasive, highest-yield route. The turning point came for our patient during a family visit to South Africa, when she underwent endoscopic ultrasound guided biopsy, a technique unavailable to in her local setting. EUS-guided sampling allows the endoscopist to select viable, enhancing regions of pancreatic masses, thereby reducing the risk of necrotic sampling that limited the initial percutaneous attempt in this case. Meta-analyses report high diagnostic performance for EUS-acquired material and reasonable concordance of Ki-67 grading with surgical specimens; accumulating data suggest that fine-needle biopsy may offer advantages over fine-needle aspiration for cellularity and reproducible grading, particularly for small lesions [9,10]. Beyond lineage confirmation with synaptophysin and chromogranin A, pan-cytokeratin positivity supports epithelial differentiation and helps exclude mesenchymal and lymphoid mimics, an important distinction in bulky retroperitoneal presentations. Application of the WHO 2022 framework then enables standardised grading; in our patient, a Ki-67 index below 3% supported Grade 1 classification despite advanced stage [1].
Biomarkers complemented tissue diagnosis, contextualised symptoms and guided management. CgA elevation paralleled tumour burden but, consistent with best practice, was interpreted alongside medication history and renal function to avoid spurious conclusions [11]. The markedly elevated 5-HIAA, obtained after adherence to dietary and drug restrictions, aligned with serotonin-mediated diarrhoea and the patient’s retrospective recognition of flushing episodes [2,3,11]. In settings without ready access to molecular imaging, such biochemical evidence can increase diagnostic confidence and guide symptom-directed therapy, while the search for tissue confirmation continues [2-4,11].
Therapeutic decisions should be anchored to grade, stage, symptom burden, and receptor status [2]. For metastatic, well-differentiated GEP-NETs, somatostatin analogs such as Octreotide LAR and Lanreotide remain first-line, providing effective control of hormone-mediated symptoms and delaying radiographic progression [2,4]. Downstream options include targeted agents (everolimus and sunitinib) for progressive disease and peptide receptor radionuclide therapy for SSTR-avid tumours; recent randomised data extend evidence to higher-grade well-differentiated disease and continue to shape sequencing strategies [4,7]. Prognosis in PanNETs depends on multiple factors, including grade, stage, tumour burden, and resectability. Population-based analyses and institutional series suggest that patients with Grade 1 tumours experience more indolent courses than those with Grade 2 disease, although metastases can occur, particularly with long-standing large primaries [4,7].
Notably, the presence of widespread metastasis despite low-grade histology reflects the known biological variability of PanNETs. While most Grade 1 tumors are considered indolent, metastatic disease can occur, particularly in the setting of delayed diagnosis and inadequate surveillance. This paradox, often overlooked, reinforces the need for timely intervention even when tumours appear histologically benign [9,10]. In our patient, the low Ki-67 index explained symptomatic improvement with somatostatin analog therapy despite widespread disease, while the tumours’ size and duration accounted for liver and nodal spread [12]. The patient’s response to octreotide LAR, a somatostatin analog, was marked. She experienced substantial symptom improvement, including resolution of diarrhoea and improved appetite, resulting in weight gain. This outcome supports the value of functional tumour management and underscores the importance of accurate and timely diagnosis to guide therapy. Treatment guidelines recommend somatostatin analogs for symptomatic control and potential tumour stabilisation in well-differentiated NETs [4,7].
The health-system context is pivotal to shortening diagnostic timelines [13]. Reports from Nigeria and other LMICs describe underutilisation of nuclear medicine, gaps in interventional radiology and advanced endoscopy, and fragmented care pathways that delay tissue diagnosis and multidisciplinary planning [15-17]. Studies from sub-Saharan Africa have highlighted how diagnostic delays in gastrointestinal cancers often result in late-stage presentations and limited treatment options [15-17]. Delays are not always due to lack of equipment but rather underutilisation of existing services, poor coordination, and limited access to specialists. In this case, interventional biopsy and pathology ultimately guided diagnosis and enabled appropriate therapy, demonstrating the central role of both in modern cancer care. The Lancet Oncology Commission advocates for strategic investment in imaging and nuclear medicine as part of comprehensive cancer control, emphasising the importance of equitable access to technologies such as multiphasic CT/MRI, EUS, image-guided biopsy, and SSTR PET/CT [18,19]. In practical terms, structured referral networks, regional tumour boards (virtual or in-person), and protocols that prioritise minimally invasive biopsy before high-risk surgery can mitigate delays and reduce patient morbidity. This case demonstrates how, once the patient accessed a center with coordinated interventional radiology, advanced endoscopy, and expert pathology, a definitive diagnosis and guideline-concordant therapy followed promptly. Earlier access to the same integrated approach would likely have prevented years of uncertainty, uncontrolled symptoms, and repeated uninformative investigations.
Conclusion
Even well-differentiated pancreatic neuroendocrine tumours can present with advanced metastatic disease when clinical suspicion is low and access to subspecialty diagnostics is constrained. This case from a low resource setting demonstrates how non-specific gastrointestinal symptoms, empiric treatment pathways, and variable radiologic interpretations can defer consideration of a neuroendocrine aetiology for years. Once an integrated pathway was implemented-targeted biochemical testing, cross-sectional imaging, and minimally invasive tissue acquisition via EUS with immunohistochemistry and Ki-67 assessment-the diagnosis of a Grade 1 PanNET became clear and directed effective first-line therapy with a somatostatin analog.
Key lessons include the value of early trigger points for NET consideration in patients with persistent diarrhoea, weight loss, and abdominal masses; the need to prioritise least-invasive, highest-yield approaches to obtain viable tissue; and the importance of multidisciplinary collaboration among clinicians, radiologists, endoscopists, interventionalists, and pathologists. Health-system strategies that expand access to EUS, image-guided biopsy, immunohistochemistry, and somatostatin receptor imaging, with regional referral pathways and tumour boards, can shorten diagnostic intervals and improve patient experience.
This case exemplifies the multifaceted barriers to timely and accurate diagnosis of NETs in LMICs and low resource settings. While pathology services and imaging may be technically available, their potential remains underutilised due to weak referral systems, insufficient procedural capacity, and low clinical suspicion. Improving physician education, interventional diagnostic capacity, and multidisciplinary collaboration is critical. Clinical recognition must be strengthened, particularly for patients presenting with gastrointestinal symptoms and unexplained abdominal masses. NETs, though rare, are increasingly recognised and treatable. Early identification, guided by pathology and supported by appropriate imaging and biopsy techniques, offers the best chance of favourable outcomes, even in low-resource settings. For patients, timely recognition and treatment can translate into symptom relief, nutritional recovery, and better quality of life even in the setting of metastatic disease. For health systems, building capacity for integrated diagnostics offers a scalable route to equity in rare cancer care.
References
- Rindi G, Mete O, Uccella S, et al. Overview of the 2022 WHO classification of neuroendocrine neoplasms. Endocr Pathol. 2022;33:115–154.
- Pavel M, Öberg K, Falconi M, et al. Gastroenteropancreatic neuroendocrine neoplasms: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31:844–860.
- Hofland J, Herrera-Martínez AD, Zandee WT, et al. European Neuroendocrine Tumor Society 2023 guidance paper for functioning pancreatic neuroendocrine tumour syndromes. J Neuroendocrinol. 2023;35:e13318.
- Del Rivero J, Perez K, Kennedy EB, et al. Systemic therapy for tumor control in metastatic well-differentiated gastroenteropancreatic neuroendocrine tumors: ASCO guideline. J Clin Oncol. 2023;41:5049–5067.
- Cozzi D, Dini C, Mungai F, et al. Pancreatic neuroendocrine neoplasms (PanNENs): spectrum of imaging findings. Gland Surg. 2020;9:S68–S81.
- Dasari A, Mehta K, Byers LA, et al. Comparative effectiveness of diagnostic imaging modalities for pancreatic neuroendocrine tumors: a retrospective study. Cancer Med. 2020;9:987–996.
- Cuthbertson D, Gupta N, Gopinath A, et al. What is the role of PET/CT in neuroendocrine neoplasms? Front Endocrinol (Lausanne). 2023;14:1117257.
- Bhatia P, Basu S. FDG PET/CT in the evaluation of pancreatic neuroendocrine tumors: current evidence and future implications. World J Radiol. 2021;13:122–134.
- Pyo JS, Cho WJ, Kang G. Diagnostic accuracy and grade concordance of Ki-67 from EUS-FNA/FNB versus surgery in pancreatic neuroendocrine neoplasms: a meta-analysis. Diagnostics (Basel). 2023;13:1512.
- Conti Bellocchi MC, Bernuzzi M, Brillo A, et al. EUS-FNA versus EUS-FNB in pancreatic solid lesions ≤15 mm: adequacy and Ki-67 assessment. Diagnostics (Basel). 2024;14:427.
- Manomaivibool S, Duvvuri A, Koopmans KP, et al. Biochemical testing for neuroendocrine neoplasms: pitfalls of chromogranin A. Arch Pathol Lab Med. 2021;145:188–200.
- Sonbol MB, Halperin DM, Kopetz S, et al. Survival and incidence patterns of pancreatic neuroendocrine tumors: a SEER analysis. Oncologist. 2022;27:573–582.
- Basuroy R, Bouvier C, Ramage JK, et al. Delays and routes to diagnosis of neuroendocrine tumours. BMC Cancer. 2018;18:1122.
- Clarke CN, Patel SH, Tran Cao HS, et al. Real-world analysis of neuroendocrine tumor misdiagnosis and delays in diagnosis. Surg Oncol Insights. 2024;100105.
- Orunmuyi AT, Adeniji-Sofoluwe AT, Balogun BO, et al. Underutilisation of nuclear medicine scans in a regional hospital in Nigeria. Ecancermedicalscience. 2020;14:1093.
- Igbinoba F, Fawole AO, Ayandipo O, et al. Current trends in interventional radiology in Nigeria: gaps, barriers, and future directions. West Afr J Radiol. 2020;27:10–16.
- Oladele AO, Nwogu CM, Arogundade FA. Medical decision-making in Nigerian oncology care: a review of diagnostic pathways and outcomes. Niger J Clin Pract. 2021;24:659–665.
- Hricak H, Abdel-Wahab M, Atun R, et al. Medical imaging and nuclear medicine in global health care: a Lancet Oncology Commission. Lancet Oncol. 2021;22:e306–e347.
- Adebayo O, Okoye CS, Ahmed R. Diagnostic delays in gastrointestinal neuroendocrine tumors in West Africa: a regional perspective. Afr J Med Med Sci. 2023;52:15–21.
