
Open Access, Volume 11
Finite element modeling in pediatric ocular trauma: Insights into abusive head trauma mechanisms
Shrayash Khare, MD, FAAP*
Assistant Professor of Clinical Pediatrics, Weill Cornell Medicine, Child Abuse Prevention and Treatment Team, NYC Health + Hospitals, Lincoln, USA.
Shrayash Khare
Assistant Professor of Clinical Pediatrics, Weill Cornell Medicine, Child Abuse Prevention and Treatment Team, NYC Health + Hospitals, Lincoln, USA.
Email: khares1@nychhc.org
Received : September 15, 2025,
Accepted : October 20, 2025
Published : October 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Purpose: To review the use of Finite Element Method (FEM) computer modeling in pediatric ocular trauma research, with emphasis on abusive head trauma (AHT, e.g. shaken baby syndrome) and comparisons to accidental injury scenarios.
Methods: The author performed a comprehensive literature search (2009-2024) and hand-selected relevant peer-reviewed FEM studies investigating infant and child eye injuries. Key findings from these computational models – including infant eye shaking, blunt impacts, blast waves, neonatal head compression during birth, and protective eyewear interventions – were critically appraised and synthesized.
Results: FEM simulations consistently indicate that repetitive acceleration-deceleration forces (shaking) can generate extreme intraocular stresses, especially at the retina and optic nerve junction, greatly exceeding those from comparable accidental impacts. Virtual shaking of infant models reproduced the distinctive retinal hemorrhage patterns seen in abusive injuries: numerous, multi-layer retinal hemorrhages extending to the far peripheral retina (ora serrata), consistent with vigorous vitreoretinal traction as the primary mechanism. By contrast, FEM analysis of neonatal birth trauma (cyclic compressive forces during labor) showed only localized posterior retinal stress with no progressive accumulation over cycles, mirroring the benign, self-limited nature of newborn retinal hemorrhages. FEM studies of blunt ocular impacts in older children (e.g. soccer ball injuries) demonstrated that appropriate protective eyewear can reduce peak retinal stress by over 60% and significantly limit globe deformation.
Conclusion: Finite element modeling has emerged as a valuable tool for investigating pediatric ocular injury mechanics that cannot be directly tested in vivo. These models support that shaking alone can directly cause severe retinal and orbital injuries in infants, helping to fill an important gap in forensic biomechanics. They also help distinguish abusive trauma from other causes by their biomechanical signatures, and they aid in evaluating preventive strategies. Continued improvements in pediatric-specific tissue properties, anatomical model fidelity, and model validation are needed to increase the predictive value of FEM in both clinical and legal contexts.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Khare S (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Khare S. Finite element modeling in pediatric ocular trauma: Insights into abusive head trauma mechanisms. Open J Clin Med Case Rep. 2025; 2388.
Introduction
Abusive Head Trauma (AHT) in infants often presents with distinctive ocular findings, most notably Retinal Hemorrhages (RH) [1]. RH are a hallmark sign of AHT – found in roughly 85% of diagnosed cases – whereas such extensive hemorrhages are rarely seen in accidental injuries or other medical conditions [2,3]. In particular, numerous hemorrhages involving multiple retinal layers all the way to the ora serrata (the far peripheral retina) are considered virtually pathognomonic for violent shaking, especially when accompanied by perimacular folds or macular retinoschisis (splitting of the retina) [2,4]. Postmortem ophthalmic examinations have reinforced that the pattern of ocular injury in AHT differs fundamentally from that in accidental trauma: infants who suffer abusive shaking show widespread hemorrhages throughout the eyes and orbits – including along the optic nerve sheath and even in the ocular muscles – whereas accidental head injuries only rarely produce such diffuse ocular bleeding. For example, one autopsy series found optic nerve sheath hemorrhages in 78% of shaken baby cases but in only ~39% of accidental cases [5]. These distribution differences indicate that the mechanism in AHT is not a simple direct impact. Instead, the unique repetitive acceleration–deceleration forces of shaking appear to cause internal shearing damage that does not occur in ordinary household falls or short drops.
The prevailing hypothesis is that rapid angular shaking of an infant’s head induces vitreoretinal traction. In infants, the gel-like vitreous is firmly attached to the retina in specific areas (especially around the posterior pole near the optic disc, and at the peripheral vitreous base). Sudden back-and-forth head motion causes these attachment points to tug forcefully on the retina, leading to tears in delicate retinal blood vessels. In contrast, alternative explanations (such as acute spikes in intracranial or intrathoracic pressure akin to severe coughing, or other factors like hypoxia) have not been able to reproduce the widespread, multilayer retinal hemorrhages seen in abusive shaking. Animal experiments support this: adult rabbits or piglets subjected to greatly elevated intracranial pressure or intense chest compression develop at most small, isolated retinal bleeds, and lab rodents vigorously shaken (without impact) show no significant retinal hemorrhages. These observations highlight the special vulnerability of the infant eye to repetitive acceleration forces, lending credence to the vitreoretinal traction mechanism in AHT. However, because we cannot ethically perform controlled shaking experiments on infants, researchers have turned to biomechanical modeling to test these ideas in silico.
Finite Element Modeling (FEM) has become a key tool to probe the mechanics of infant head and eye injuries. In brief, FEM is a computer simulation technique in which complex structures are divided into many small elements, and the response of each element to applied forces is calculated. For example, an eye model can be partitioned into thousands of tiny blocks or shells, and by assigning realistic material properties to each part (sclera, retina, vitreous, etc.), one can apply forces (like a shaking motion or an impact) and compute the resulting stresses and strains in each region. Compared to animal or dummy experiments, FEM is relatively inexpensive and allows precise control and measurement of biomechanical variables (pressure, stress, strain, energy) throughout the eye. Over the past two decades, advances in computing power and pediatric anatomical data have enabled increasingly sophisticated FEM studies – from early generic eye models on supercomputers to modern infant-specific simulations – all aimed at understanding how abusive shaking causes ocular injuries and how those injuries differ from other trauma. This review assembles the findings of those studies to clarify the injury mechanisms underlying retinal hemorrhages in AHT. By synthesizing results across multiple models and scenarios, we illustrate how FEM research has enhanced our understanding of AHT pathophysiology and helped differentiate abusive injury from accidental trauma. In doing so, we underscore the importance of rigorous biomechanical evidence in what has at times been a controversial field, and why this body of work is crucial for improving both diagnostic specificity and preventive strategies.
Methodology
Literature search and study selection
This review was conducted as an independent, author-driven project. The author personally performed a comprehensive literature search in 2024 using databases such as PubMed and Google Scholar to identify finite element modeling studies related to pediatric eye injuries and abusive head trauma. Search terms included combinations of keywords like finite element, computational model, retinal hemorrhage, shaken baby, abusive head trauma, ocular trauma, pediatric, and infant eye. The search was supplemented by examining reference lists of key articles and prior reviews to ensure all relevant studies were captured. The author hand-selected each article and read them in full, emphasizing quality and relevance to the topic of retinal injury mechanisms.
Inclusion and exclusion criteria
The review focused on peer-reviewed studies (approximately 2000-2025) that utilized finite element analysis to simulate ocular or head injuries in infants and children, particularly those addressing retinal hemorrhages or related ocular findings. Both studies dedicated to eye-specific models and those integrating the eye within whole-head models were included, provided they reported outcomes pertinent to retinal injury or vitreoretinal mechanics. Clinical and autopsy studies were not the primary targets, but high-impact clinical studies are cited to provide context for the modeling results. Non-English articles, studies using purely analytical or other computational methods (without FEM), and models not involving pediatric subjects or not reporting ocular outcomes were excluded. Where multiple articles came from the same research group or model, the most comprehensive or recent findings were prioritized to avoid redundancy.
Critical appraisal and thematic synthesis
Each included article was critically appraised by the author, with attention to model construction (e.g. anatomical fidelity, material properties), loading scenarios (shaking, impact, etc.), and reported outcome measures (stress, strain, pressure distributions in ocular tissues). Key data and conclusions were extracted from each study. Rather than simply cataloging studies chronologically, the author organized the synthesis around major themes that emerged across the literature. These themes shaped the structure of the discussion: for example, how FEM studies elucidate the mechanism of retinal hemorrhage in shaking, how findings differ between abusive and accidental trauma, and how modeling has been applied to prevention (protective eyewear) and broader injury patterns. Grouping the evidence by concept (rather than by individual paper) allows for a more accessible narrative for readers, highlighting consensus findings and differences between scenarios. Throughout the writing, the author cross-verified that all factual statements are directly supported by the sources cited.
Scholarly integrity
A strong emphasis was placed on accuracy and transparency in this review. All statements and quantitative values drawn from the literature are accompanied by appropriate citations to the original studies. The reference list was carefully compiled to match in-text citations in AMA style, and each reference was checked to ensure it supports the context for which it is cited. The author made a conscious effort to avoid overinterpretation of modeling results, sticking closely to the data and conclusions presented by the study authors. In cases of controversy or uncertainty, this is acknowledged in the text rather than glossed over. By adhering to these practices, the review upholds scholarly integrity and provides a reliable summary of the current state of FEM research on pediatric retinal injury mechanisms.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only
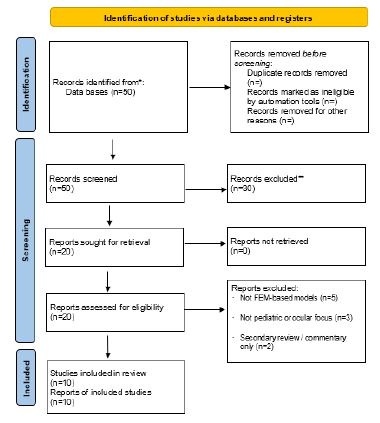
Figure 1: Literature search and study selection flowchart. A total of 50 records were identified; after screening and eligibility assessment, 10 primary studies of pediatric ocular FEM models were included in the review.
Source: Page MJ, et al. BMJ 2021; 372: n71. doi: 10.1136/bmj.n71.
Source: Page MJ, et al. BMJ 2021; 372: n71. doi: 10.1136/bmj.n71.
Discussion
FEM insights into retinal hemorrhage mechanisms in shaking
Finite element studies have provided valuable insight into how violent shaking can damage the infant eye in ways that align with clinical findings of retinal hemorrhages. Early computational models laid the groundwork by exploring general eye biomechanics. For instance, Liu et al. modeled an infant eye subjected to a shockwave blast – a scenario with no direct impact – and found that the highest stresses occurred at the back of the globe near the optic nerve insertion [7]. This result was striking because it suggested that a sudden acceleration of the whole eye (even from an air-blast) preferentially strained the posterior ocular structures rather than the anterior parts. In other words, inertial forces alone (without a blunt hit) could concentrate stress at the optic nerve head and retina [7]. This finding foreshadowed the kind of shearing damage later implicated in shaken infants, where global acceleration of the head causes the eye to deform within the orbit.
As researchers began applying FEM specifically to abusive head trauma scenarios, they encountered significant knowledge gaps. In 2009, Margulies et al. pointed out that pediatric-specific tissue properties were not well established at the time, forcing early modelers to make educated guesses for critical parameters [8]. For example, in one early model the elasticity of an infant’s sclera was assumed to be on the order of only a few MPa (much softer than adult sclera, which is ~300 MPa) because no direct measurements from infants existed [8]. Uncertainties like these limited the ability to draw firm conclusions from those first models. Nonetheless, even the initial FEM attempts were useful for illustrating possible injury mechanisms.
A major advance came with development of anatomically detailed infant eye models for shaking simulations. Rangarajan et al. (2009) produced one of the first high-fidelity FEM models of a 6-month-old infant’s eye and orbit specifically to simulate shaking forces [9]. Their model included realistic structures: a deformable eyeball (sclera, lens, vitreous, retina) within an orbital cavity, along with the extraocular muscles and surrounding orbital fat. Crucially, they modeled the vitreoretinal interface to reflect infant anatomy – meaning the vitreous was strongly attached to the retina at the posterior pole (around the macula) and at the peripheral retina near the ora serrata. This allowed the simulation to capture the tethering effect of the vitreous on the retina during movement. When the model eye was subjected to angular acceleration pulses representative of vigorous shaking (approximately 5 Hz oscillatory whiplash motion), the results showed that vitreous dynamics dominated retinal stress responses. In particular, treating the vitreous humor as a nearly fluid mass that can move relative to the eye wall – except at those attachment points where it was “tied” to the retina – led to much higher retinal strain than if the vitreous were modeled as a solid gel moving with the eye. Under these conditions, repetitive shaking caused a progressive build-up of stress in the retina with each back-and-forth cycle. The peak stresses localized at the exact sites of firm vitreous attachment: the peripheral retina (vitreous base region) and the posterior pole around the optic disc. This pattern is remarkable because it mirrors what ophthalmologists see in abusive head trauma: the most severe retinal hemorrhages tend to cluster around the ora serrata in the periphery and the optic nerve head centrally. The FEM results thus provided biomechanical evidence for the vitreoretinal traction hypothesis, showing that with each shake, the cumulative “tugging” strain on the retina could plausibly reach tissue failure thresholds in those vulnerable areas. This repetitive or “stress stacking” effect offers an explanation for why a series of shakes can cause retinal damage that a single sudden jolt might not – each oscillation adds strain on partially damaged tissues until blood vessels finally rupture.
Subsequent models refined these insights with even greater anatomical detail. Suh et al. (2021) developed a high-resolution FEM of a young child’s eye that explicitly divided the retina into three separate layers (representing preretinal, intraretinal, and subretinal tissues) [10]. They also implemented discrete vitreous attachment points at known adhesion sites: the macula (center of the retina), the major retinal vessel branch points, and the peripheral vitreous base. Using shaking inputs around 2-3 Hz (based on observed kinematics from doll-shaking experiments), this model calculated that peak stresses on the retina reached on the order of 9-11 kPa. The highest stresses again appeared at the macula and along the peripheral retina where the vitreous was firmly tethered. Importantly, once the shaking motion reached its peak velocity, the stress became uniformly elevated across all retinal layers in those attached regions. In practical terms, this means a severe shaking event could produce hemorrhages that span all layers of the retina (preretinal, intraretinal, subretinal) in the areas of strongest vitreoretinal adhesion. Clinically, that corresponds to the multilayered hemorrhages often seen in AHT cases. By contrast, when Suh et al. ran a simulation in the same model with an increased intracranial pressure (to mimic a swelling brain or severe cough), the resulting retinal stress pattern was much more localized – mainly around the optic nerve head – and did not elevate stresses uniformly through all retinal layers. This directly addresses the debate about mechanism: diffuse, multilayer retinal hemorrhages are a signature of repetitive traction from shaking rather than a transient spike in pressure. The FEM evidence thus strongly supports that vitreoretinal traction is the primary driver of retinal hemorrhage in shaking trauma, whereas pure pressure alone is unlikely to cause the widespread hemorrhagic retinopathy characteristic of abuse.
Abusive vs. accidental head trauma: Biomechanical differences
In addition to illuminating the mechanism of retinal injury, finite element models allow direct comparisons between abusive shaking and accidental injury scenarios under controlled conditions. One of the most comprehensive comparative studies was by Nadarasa et al. (2018), who developed a detailed FEM of a 5-month-old infant’s head and eyes, then subjected it to two different real-world trauma inputs: violent shaking vs. a short fall impact [11]. The model included all major ocular and orbital structures (retina, choroid, sclera, optic nerve, eye muscles, orbital fat), scaled to infant dimensions with about 45,000 finite elements for high resolution. For the abusive scenario, they used angular acceleration data recorded from a dummy being vigorously shaken (~5-6 Hz shaking, peaking around 5000 rad/s²); for the accidental scenario, they used acceleration profiles from an infant dummy being dropped from up to 1.3 meters onto a hard surface. The side-by-side results were telling: even the mildest shaking simulation produced several-fold higher retinal stress and strain than the most severe fall simulation. Quantitatively, the peak retinal strain during shaking was roughly 14 times greater than that seen in the highest-impact fall case. Shaking not only generated higher magnitude forces in the eye, but it also induced a different pattern of stress distribution: diffuse stress throughout the globe, including both posterior and peripheral retina, for the shaking event, versus stress mainly confined to the posterior pole (back of the eye) in the fall events. This directly reflects clinical observations – a violent shake leads to widespread, multi-quadrant retinal hemorrhages (often extending to the periphery and sometimes with retinal folds or detachments), whereas even a high-height isolated fall, while it may cause serious head injury, rarely produces the kind of extensive retinal bleeding seen in AHT.
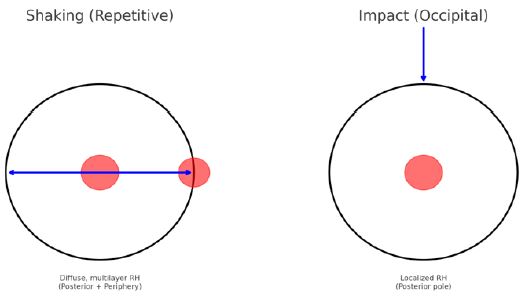
Figure 2: Conceptual illustration of how finite element models differentiate shaking vs. impact injury to the infant eye. Left: During repetitive shaking, inertial forces cause high stress at both the posterior pole (around the optic nerve head) and the retinal periphery (ora serrata), corresponding to the widespread, multi-layer hemorrhages observed in abusive head trauma. The cyclic nature of shaking allows stresses to compound with each shake, reaching levels that tear blood vessels in multiple retinal layers. Right: In a single occipital impact (fall onto the back of the head), stress is mostly confined to the back of the eye; the retinal periphery experiences little strain. This aligns with clinical findings that accidental impacts (even severe) tend to cause only localized or posterior pole retinal hemorrhages, if any. (Red shaded areas indicate regions of highest stress in the model; blue arrows depict the direction of head motion or impact force).
Beyond the eye itself, these FEM comparisons underscored a broader point: traditional head injury metrics developed for impact (like the Head Injury Criterion, HIC) can be misleading when applied to shaking. In Nadarasa et al.’s simulations, the fall scenarios registered very high HIC values (indicating a very severe impact), while the shaking scenarios had low HIC values – yet it was the shaking that caused far more ocular injury and stress on the retinal structures. In essence, the rotational, whiplash-like kinematics of shaking, especially when repetitive, are far more injurious to the eye than a single translational head impact, even if that impact involves high force. Their simulations confirmed that shaking alone, without any head contact, can readily exceed the mechanical thresholds for retinal and optic nerve damage in an infant. This finding is biomechanical evidence refuting the argument that only a hard impact could cause the retinal and intracranial findings seen in abuse. It quantitatively demonstrated that a purely shaking event is sufficient to produce the classic ocular injuries of SBS/AHT, whereas a single short fall is very unlikely to do so.
Building on earlier FEM studies, Hans et al. constructed a detailed finite element model of the infant eye to directly compare shaking and impact dynamics [12]. Their analysis showed that shaking produced more sustained and higher posterior retinal forces than impact, with impulses up to 13 times greater, strongly implicating inertial stresses at the optic nerve head as a driver of hemorrhage risk. Complementing this, Roth et al. modeled a 6-month-old infant head and demonstrated that vigorous shaking alone could generate bridging vein strains approaching rupture thresholds, comparable to those seen in impact trauma [13]. Peak intracranial pressure during shaking was localized in the frontal region near the orbits, raising the possibility that such stresses may transmit to the vitreous and contribute to vitreoretinal injury. Taken together, these findings reinforce that shaking is not a benign mechanism: it can plausibly generate both intracranial and intraocular injury without direct impact, and underscores the importance of FEM in elucidating forces unique to abusive head trauma.
Other modeling efforts and experimental analyses further highlight differences in injury patterns between angular shaking forces and linear impact forces. For example, a computational study by Lam et al. (2022) examined soccer ball impact trauma to the eye and compared it conceptually to abusive shaking [14]. That study found that a blunt projectile impact (like a fast soccer ball) creates a transient pressure wave in the eye that travels front-to-back, causing a brief spike of very high pressure followed by a rebound to negative pressure. The highest stresses in the soccer-ball scenario tended to occur at the point of contact (anterior eye) and along the immediate impact axis, often damaging structures near where the force was applied [14]. The retina in such cases experienced its greatest stress at the vascular attachment points (where blood vessels anchor to the retina), with stress values around 15 kPa at those distal vessel branches [14]. However, the overall retinal injury pattern from a single blunt impact was more localized – often confined to the posterior pole or one quadrant of the retina [14]. This aligns with clinical experience: a focused blunt ocular trauma (like a sports ball injury) might cause retinal hemorrhages, but typically in a limited area (for instance, only in the superior retina of the impacted eye) rather than everywhere. The primarily linear force and single-impact nature of such trauma likely accounts for the more localized injury profile and the much lower incidence of extensive retinal hemorrhages compared to shaking [14]. By contrast, repetitive angular forces in shaking distribute the insults across a larger portion of the eye and allow for cumulative damage over time, which is why shaking causes far more widespread and multi-layer hemorrhages. In fact, epidemiologically, retinal hemorrhages are far more common in abuse than in accidental head injuries of any kind; for example, systematic reviews have found that the majority of shaken infants have retinal hemorrhages, whereas only a small minority of serious accidental trauma cases do. The FEM studies support this difference: they show that the mechanics of shaking are uniquely suited to injure the retina in diffuse and severe ways that one-time impacts (or isolated increases in pressure) cannot.
It is also worth noting the role of duration and repetition. A single acceleration-deceleration event (whether a shake or an impact) delivers a finite impulse to the eye. Shaking is essentially a series of impulses, giving the eye tissues no time to recover. One modeling analysis quantified this by integrating stress over time and found that a single shake cycle imparted nearly three times the “stress-time dose” to the retina as a single head impact event of comparable peak acceleration [15]. In practical terms, shaking “soaks” the retina in high stress for longer, and repeatedly, whereas an impact is a brief spike of stress followed by relief. This helps explain why, for example, in neonatal birth trauma, where the head might experience repetitive compressive forces (with each uterine contraction during delivery) but at relatively low magnitudes, the retinal hemorrhages tend to be mild and resolve quickly. FEM simulations of intrapartum head compression (mimicking the squeeze of the birth canal on a baby’s skull) showed some elevated stress in the infant’s retina, but it was confined to the posterior pole and did not accumulate significantly over successive compressions [16]. This correlates with the clinical observation that newborn RHs are generally few, small, and confined near the optic disc, clearing within a few weeks. The absence of high-frequency, high-magnitude oscillatory motion in normal labor (as compared to violent shaking) means that tissue fatigue and shear do not build up to pathological levels in the eye. Thus, FEM helps distinguish truly pathological trauma (shaking) from benign repetitive forces (birth) in terms of retinal outcomes.
Makoto Yoshida and colleagues advanced FEM of ocular trauma by explicitly comparing stress transmission in abusive shaking versus impact trauma [17]. Using a simplified spherical eye model validated against an agar gel physical analogue, they showed that shaking produces broad, sustained tensile stresses across the posterior retina, whereas impact generates sharper but transient stresses. Importantly, they proposed the “time integration of stress” (Pa·s) as a predictor of retinal hemorrhage, demonstrating that a single abusive shake delivered nearly three times the cumulative stress of a fall impact (101 vs. 36 Pa·s). This insight helps explain the paradox that RH is common in shaking but rare in short falls, emphasizing cumulative load over peak force. The study thus reinforced that FEM can mechanistically clarify why SBS/AHT produces diffuse, multilayer retinal hemorrhages while accidental impacts do not.
Multi-system injury considerations in AHT
While FEM studies focused on the eye have shed light on retinal hemorrhages, it is important to place these findings in the context of the broader injury pattern seen in abusive head trauma. AHT often involves a triad of injuries: subdural hemorrhages in the brain, retinal hemorrhages in the eyes, and diffuse axonal or cervical spine injuries – all without external impact in many cases. Biomechanical modeling has been extended to these other organ systems, strengthening the case that shaking alone can produce the full spectrum of SBS injuries. In a review of infant head dynamics, Nadarasa et al. (2014) compiled several finite element studies and concluded that violent shaking can indeed generate the classic triad of subdural hematomas, retinal hemorrhages, and neck injuries in silico without any blunt impact [18]. For example, when an infant head FEM includes bridging veins (the fragile veins spanning the subdural space in the brain), simulations show that inertial shaking forces are sufficient to stretch these veins to near their breaking point. One cited model found that purely shaking a dummy’s head caused bridging vein strains comparable to those seen when shaking was combined with a minor head impact. In other words, the rapid angular deceleration of the head during shaking can tear subdural veins, explaining how thin, widespread subdural hemorrhages (especially along the top of the brain or between the hemispheres) occur in abuse cases. This directly challenges the hypothesis that a forceful impact is needed to cause subdural bleeding – the models indicate it is not. Similarly, the whiplash motion of shaking can injure the cervical spine and neck soft tissues in infants. Autopsy studies have found neck muscle hemorrhages and ligament damage in many shaken infants, injuries that historically were ex-“ occult ex-” examination [5,10]. FEM researchers note that to fully capture this, future models should include the infant’s neck along with the head [18]. A realistic head-neck FEM could simulate how an infant’s neck flexes and extends during shaking and possibly predict the stresses on the cervical spinal cord and ligaments. While such a complex model is still under development, the trend is toward integrating multiple regions (skull, brain, eyes, neck) to see if a given event (like pure shaking vs. a short fall) can produce the combined injury pattern observed clinically. This systems-level approach is essentially what clinicians do in practice – they look at the constellation of injuries to judge likelihood of abuse – and FEM is moving in the same direction by unifying the simulations.
Furthermore, contemporary clinical guidelines have begun incorporating biomechanical insights. The European Society of Paediatric Radiology, for instance, recently published recommendations on differentiating abusive head injury from accidents based on imaging patterns [19]. They note, for example, that multifocal subdural hematomas along the falx or tentorium (midline and rear brain coverings) are much more common in abuse than in short falls, because shaking’s rotational forces tend to tear the veins at those particular locations. They also highlight that certain skeletal injuries (like posterior rib fractures and classic metaphyseal lesions of long bones) are highly specific to abuse and often co-occur with the intracranial and ocular findings [19]. All of this reinforces that no single injury (including retinal hemorrhage) is diagnostic in isolation – context is key. FEM research is responding to this by trying to create models that are as anatomically and physiologically faithful as possible to a real infant, incorporating age-dependent properties such as the flexibility of open cranial sutures, the higher brain water content in infants, and so on. Infant skulls, for example, are not just “small adult” skulls – they have open fontanelles and more compliant bone, which can redistribute forces differently than an adult skull would. If a model incorrectly treats an infant head like a mini adult head (rigid skull, fused sutures), it might misestimate stresses and fail to predict injuries accurately. Fortunately, newer models are addressing this: some researchers have even developed methods to morph a generic infant head FEM to match a specific baby’s head shape and size based on that infant’s CT/MRI, creating subject-specific models [20]. This recognizes that even among infants, individual anatomy can affect injury outcome – for instance, a slightly larger subarachnoid space or thicker skull might change how forces transmit. All these efforts contribute to making FEM a robust investigative tool that parallels clinical forensic analysis. By demonstrating that shaking can plausibly cause the multi-system injury complex of SBS, these simulations provide a scientific counterpoint to claims that the findings in suspected abuse must have come from other causes [19]. In summary, the multi-system FEM evidence aligns tightly with clinical data: shaking is uniquely capable of causing simultaneous ocular, brain, and neck injuries, whereas common household accidents are not.
Implications for prevention and future directions
Finite element modeling is not only useful for forensic analysis of injury mechanisms – it is also being applied proactively to improve child safety. A good example is the work by Suh et al. (2023), who used a pediatric eye FEM to test the effectiveness of protective eyewear in blunt impact scenarios [21]. They simulated a fast-moving soccer ball striking an 8-year-old child’s eye, comparing the outcomes with and without protective glasses (and even comparing different lens materials). The model revealed that a polycarbonate shatterproof lens dramatically reduced the force transmitted to the eye: peak retinal stress dropped by about 61%, and the overall strain energy within the globe was nearly 70% lower when the child wore the polycarbonate sports goggles. In practical terms, with the protective eyewear in place, the simulated retinal stress stayed below ~5 kPa – a level associated with a low risk of vitreoretinal damage in experimental studies – whereas without protection that threshold was exceeded during the impact. Standard plastic (acrylic) lenses, on the other hand, provided only partial protection and tended to crack under the same impact, which in a real scenario could introduce secondary hazards from lens fragments. This virtual experiment vividly demonstrated that well-designed protective eyewear can markedly dampen the forces delivered to a child’s eye, quantitatively supporting the recommendations of wearing shatterproof sports goggles in youth athletics. Beyond this specific example, the study illustrates the broader power of FEM to evaluate injury prevention strategies ethically and efficiently – one can test “what if” scenarios (different protections, different impact angles, etc.) without ever putting a child in harm’s way.
Looking ahead, continued advancements in pediatric FEM promise to further bridge biomechanics with clinical practice. One ongoing effort is to gather more precise pediatric tissue data – for instance, measuring the true tensile strength of infant retinal attachments, or the viscoelastic properties of newborn sclera and vitreous. These data would allow models to be calibrated with much greater accuracy, reducing the reliance on adult data or estimations. Another thrust is developing integrated models that include the entire head and eyes (and even the upper spine) together. Such models would let us simulate the interaction of brain, eye, and neck injuries in one framework, as discussed above. As computational power grows, researchers can include more anatomical detail – e.g. modeling individual retinal blood vessels or the layered microstructure of the retina – without the simulations becoming intractable. However, increasing complexity also underscores the need for rigorous validation. Model predictions must be continually checked against real-world data: for example, comparing the pattern of retinal hemorrhages or fractures predicted by a model with those observed in actual clinical cases or physical experiments. Encouragingly, the field is moving in that direction, using available clinical case series and even animal experiments to validate that the models produce realistic injury patterns.
In the future, we can envision developing a high-fidelity "virtual child" that can be subjected to various trauma scenarios. Investigators could input the conditions of a specific case (e.g. a fall from X height onto Y surface, or a shaking of Z intensity) and see if the model’s output matches the injuries observed in that child. While we are not there yet, the incremental progress made by the FEM studies reviewed here is building toward that goal. This would be immensely useful both scientifically – to test injury hypotheses – and clinically/forensically, to evaluate whether a caregiver’s explanation of injury is mechanically plausible. It could also guide product safety design (as in the eyewear example) by pinpointing failure points or effective protective measures. Ultimately, the integration of detailed pediatric finite element models into research and forensic investigations holds the promise of shedding light on ambiguous cases and, importantly, preventing abusive injuries by informing education and safety measures.
Table 1: Below summarizes several core FEM studies in pediatric ocular trauma and their key findings, highlighting how each has contributed to our understanding of retinal injury mechanisms under different conditions.
| Study | Year | Model Type | Key Findings | Implications for RH/AHT |
|---|---|---|---|---|
| Uchio et al. | 1999 | Whole-eye FEM based on cadaver tissue properties | Developed a 3D FEM of the eyeball using measured stress–strain data from human cornea and sclera. Identified rupture thresholds (cornea ~18% strain, sclera ~6.8% strain) under missile impact; predicted corneal rupture at 1.95 mm missile (30 m/s) and scleral rupture at 0.95 mm missile (30 m/s). | Provided early validated FEM of the intact eye. Though focused on intraocular foreign body (IOFB) injuries, it established methodological foundations and rupture thresholds relevant to later pediatric FEM studies of RH/AHT. |
| Roth et al. | 2007 | FEM of 6-month-old infant head | Shaking produced bridging vein strain up to 90%, impact up to 100% (both near rupture). Peak intracranial pressures during shaking (2.2 kPa) localized near orbits. | Demonstrated that shaking alone can induce subdural bleeding equivalent to impact; orbital proximity suggests possible stress transmission to vitreous and retinal vessels. |
| Rangarajan et al. | 2009 | FEM of infant eye + orbit with vitreous attachments | Repetitive shaking caused cumulative stress (“stress stacking”) at vitreoretinal adhesion sites (macula, ora serrata). | Supported vitreoretinal traction as a primary mechanism for multilayer hemorrhages in AHT. |
| Hans et al. | 2009 | FEM of infant eye with orbital structures | Shaking produced higher, more sustained posterior retinal forces than impact; impulse ~13× greater. | Showed shaking stresses at the infant head exceeded adhesion thresholds, reinforcing shaking as sufficient for RH. |
| Margulies et al. | 2010 | Review of FEM limitations | Highlighted lack of pediatric tissue property data, early assumptions about scleral elasticity, and vitreous behavior. | Established the need for pediatric-specific FEM calibration to improve reliability. |
| Li et al. | 2013 | Biofidelic FEM of 6-month-old infant head | Validated against cadaver impact tests. Showed drop height and surface stiffness alter skull strain and compliant sutures redistribute force. | Improved fidelity of infant head FEM; underscored that infant skull anatomy must be modeled accurately when assessing trauma. |
| Nadarasa et al. | 2014 | FEM of infant head (eyes, skull, brain, 45k elements) | Shaking caused ~14× higher retinal stress than falls; posterior pole showed diffuse globe stress, falls localized stress. | Showed shaking alone can exceed injury thresholds, aligning with widespread RH in AHT. |
| Yoshida et al. | 2014 | Simplified ocular FEM validated with gel model | Introduced stress-integration (Pa·s) as predictor of RH. Shaking delivered nearly 3× cumulative retinal stress compared to a fall (101 vs 36 Pa·s). | Explained why RH is frequent in AHT but rare in short falls; cumulative load better predicts hemorrhage than peak stress. |
| Nadarasa et al. | 2014 | FEM of infant head (eyes, skull, brain, 45k elements) | Shaking caused ~14× higher retinal stress than falls; posterior pole and diffuse globe stress, falls localized stress. | Showed shaking alone can exceed injury thresholds, aligning with widespread RH in AHT. |
| Suh et al. | 2021 | High-resolution infant FEM with layered retina | Shaking generated 9–11 kPa stress across all retinal layers at vitreoretinal adhesion points; ICP increase caused only localized optic nerve stress. | Demonstrated that diffuse multilayer RH are rotational (shaking) rather than pressure-driven. |
| Lam et al. | 2022 | Pediatric eye FEM: focal vs blunt impact | Blunt impact caused transient pressure wave with stress peaks at vascular beds; shaking pressure injuries more localized. | Supported distinction between focal sports injuries and diffuse multilayer RH of AHT. |
| Lam et al. | 2023 | FEM of neonatal head compression (birth) | Cyclic head compression produced localized posterior stress without cumulative build-up. | Explained benign, self-limited RH in newborns versus progressive RH in AHT. |
| Suh et al. | 2023 | FEM of 8-year-old eye with protective eyewear | Polycarbonate lenses reduced retinal stress by ~60%, keeping peak <5 kPa. | Validated protective eyewear efficacy in preventing RH from blunt trauma. |
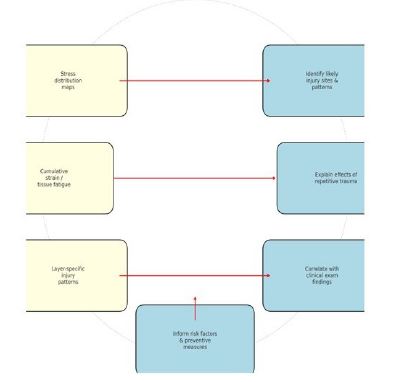
Figure 3: Thematic framework linking FEM simulation outputs to clinical and forensic insights. Finite element models provide quantitative data such as stress distribution maps (showing where and how much force is experienced by tissues), cumulative strain or tissue fatigue from repetitive loading, and layer-specific injury patterns. These outputs translate into insights by identifying likely sites and patterns of injury (e.g., retinal hemorrhages at the periphery vs. posterior pole), explaining the effects of repetitive trauma (why multiple shakes cause damage when one might not), correlating with clinical exam findings (such as multi-layered hemorrhages corresponding to high stresses in all retinal layers), and informing risk factors or preventive measures (for instance, how variations in anatomy or the use of protective eyewear influence injury outcome).
Conclusion
Finite element modeling has become an indispensable tool in the study of abusive head trauma, offering a scientific window into internal injury mechanics that were previously inferred only from clinical observations. Over the past decade-plus, FEM simulations have provided mechanistic clarity to what clinicians have long suspected: repetitive shaking can directly cause the classic findings of SBS/AHT – notably widespread, multilayer retinal hemorrhages as well as subdural bleeding – even in the absence of any impact. The models reviewed here consistently show that the patterns and magnitudes of stress produced by shaking align with the injuries seen in abused infants, whereas equivalent accidental scenarios (short falls, isolated impacts, or increased intracranial pressure alone) do not generate the same injury profile. This convergence of virtual evidence with real-world clinical data strongly rebuts the “junk science” claims made by some skeptics regarding shaken baby syndrome. On the contrary, the biomechanics of AHT are grounded in solid physics: the distinctive combination of rotational forces and repetitive loading in shaking is uniquely capable of causing diffuse ocular and neural trauma, whereas ordinary accidents lack these dynamics.
By rigorously testing various scenarios, FEM research has helped differentiate accidental trauma from abuse, not by speculation but by demonstrating which forces can – or cannot – produce the observed injuries. These simulations have essentially recreated abusive events in a computer model, lending credence to forensic diagnoses when a child’s injuries match the paral-“ fingerprint” parallel, computational modeling is informing injury prevention. The example of sports eyewear shows how we can use FEM to design and validate protective strategies before implementing them in the real world. More broadly, FEM studies are shedding light on age-related biomechanical vulnerabilities (for instance, how an infant’s compliant skull and firm vitreoretinal attachments contribute to injury) and thereby guiding pediatricians and investigators in what signs to look for.
Looking forward, continued refinement of these models will further strengthen their utility. A priority is improving pediatric-specific data for model inputs – measuring infant tissue properties and developing better anatomical models – so that simulations become ever more biofidelic. Another priority is validation and standardization: as multiple research groups develop infant head/eye models, comparing their outputs to actual clinical cases or experimental data will be crucial for building confidence in their predictions. Eventually, we may have a virtual injury assessment tool that can test caregivers’ explanations against biomechanical reality in a court of law or help emergency physicians rapidly evaluate if an injury pattern is consistent with a claimed accident.
In summary, the body of FEM literature to date has substantially advanced our understanding of how retinal hemorrhages occur in abusive head trauma. It provides a coherent mechanistic framework that ties together clinical observations, laboratory findings, and the laws of physics. With this foundation, the field is better equipped to move beyond old controversies and focus on constructive efforts: improving diagnostic accuracy, protecting children through better prevention (in sports and in identifying abuse early), and continually refining the models as new data emerge. Finite element modeling, once an experimental technique on the fringes of biomechanics, is now at the forefront of pediatric trauma research – and it will undoubtedly play an increasing role in both the scientific investigation of injury mechanisms and the practical mission of safeguarding children.
References
- Levin AV. Retinal hemorrhages: advances in understanding. Pediatr Clin North Am. 2009;56:333–344.
- Morad Y, Wygnanski-Jaffe T, Levin AV. Retinal hemorrhage in abusive head trauma. Clin Exp Ophthalmol. 2010;38:514–520.
- Maguire SA, Watts PO, Shaw AD, et al. Retinal haemorrhages and related findings in abusive and non-abusive head trauma: a systematic review. Eye. 2013;27:28–36.
- Greenwald MJ, Weiss A, Oesterle CS, Friendly DS. Traumatic retinoschisis in battered babies. Ophthalmology. 1986;93:618–625.
- Wygnanski-Jaffe T, Levin AV, Shafiq A, et al. Postmortem orbital findings in shaken baby syndrome. Am J Ophthalmol. 2006;142:233–240.
- Uchio E, Ohno S, Kudoh J, Aoki K, Kisielewicz LT. Simulation model of an eyeball based on finite element analysis on a supercomputer. Br J Ophthalmol. 1999;83:1106–1111.
- Liu X, Wang L, Wang C, Sun G, Liu S, Fan Y. Mechanism of traumatic retinal detachment in blunt impact: a finite element study. J Biomech. 2013;46:1321–1327.
- Margulies SS, Coats B, Christian CW, Forbes BJ, Duhaime AC. What can we learn from computational model studies of the eye? J AAPOS. 2009;13:332.
- Rangarajan N, Kamalakkannan SB, Hasija V, et al. Finite element model of ocular injury in abusive head trauma. J AAPOS. 2009;13:364–369.
- Suh DW, Song HH, Mozafari H, Thoreson WB. Determining the tractional forces on the vitreoretinal interface using a computer simulation model in abusive head trauma. Am J Ophthalmol. 2021;223:396–404.
- Nadarasa J, Deck C, Meyer F, Bourdet N, Raul JS, Willinger R. Development of a finite-element eye model to investigate retinal hemorrhages in shaken baby syndrome. Biomech Model Mechanobiol. 2018;17:517–530.
- Hans SA, Bawab SY, Woodhouse ML. A finite element infant eye model to investigate retinal forces in shaken baby syndrome. Graefes Arch Clin Exp Ophthalmol. 2009;247:561–571.
- Roth S, Raul JS, Ludes B, Willinger R. Finite element analysis of impact and shaking inflicted to a child. Int J Legal Med. 2007;121:223–228.
- Lam MR, Dong P, Shokrollahi Y, Gu L, Suh DW. Finite element analysis of soccer ball-related ocular and retinal trauma and comparison with abusive head trauma. Ophthalmol Sci. 2022;2:100129.
- Yoshida M, Yamazaki J, Mizunuma H. A finite element analysis of the retinal hemorrhages accompanied by shaken baby syndrome/abusive head trauma. J Biomech. 2014;47:3454–3458.
- Lam MR, Yang CD, Colmenarez JA, et al. The role of intrapartum fetal head compression in neonatal retinal hemorrhage. J AAPOS. 2023;27:267.e1–267.e7.
- Yoshida M, Nagatomi R, Yamada T, Taga Y, Oka H. Finite element analysis of shaken baby syndrome: predictive indicators for retinal hemorrhage. Pediatr Radiol. 2014;44:S587–S593.
- Nadarasa J, Deck C, Meyer F, Willinger R, Raul JS. Update on injury mechanisms in abusive head trauma—shaken baby syndrome. Pediatr Radiol. 2014;44:S565–S570.
- Colleran GC, Fossmark M, Rosendahl K, et al. Imaging of suspected child abuse: practice recommendations by the European Society of Paediatric Radiology (ESPR). Eur Radiol. 2025;35:1868–1880.
- Li Z, Han X, Ge H, Ma C. A semi-automatic method of generating subject-specific pediatric head finite element models for impact dynamic response. J Mech Behav Biomed Mater. 2016;60:557–567.
- Suh A, Lam M, Shokrollahi Y, et al. Quantifying the efficacy of protective eyewear in pediatric soccer-induced retinal injury. J AAPOS. 2023;27:131.e1–131.e6.
