
Open Access, Volume 11
Skeletal muscle metastases misdiagnosed as benign tumor by ultrasound: Report of two cases with literature review
Duan Yang Siyu1,2; Qu Wenhao1,2; Nie Fang2*
1The Second Clinical Medical School, Lanzhou University, China.
2Department of Ultrasound Medical Center, The Second Hospital of Lanzhou University, Gansu Province Medical Engineering Research Center for Intelligence Ultrasound, Gansu Province Clinical Research Center for Ultrasonography, China.
Nie Fang
Department of Ultrasound, Lanzhou University Second Hospital, Chengguan District, Lanzhou, Gansu, 730000, China.
Tel: 13993163088;
Email: ery_nief@lzu.edu.cn
Received : September 18, 2025,
Accepted : October 13, 2025
Published : October 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Background: Skeletal Muscle Metastases (SMM) are rare and pose diagnostic challenges due to overlapping sonographic features with benign tumors.
Purpose: To analyze pitfalls in ultrasonographic misdiagnosis of SMM and propose a multimodal solution.
Methods: Two cases (20M with AML, 60M with NSCLC) presenting lower limb masses underwent comprehensive ultrasound evaluation: grayscale, Doppler, Contrast-Enhanced Ultrasound (CEUS), and ultrasound-guided biopsy. A literature review of SMM characteristics was conducted.
Conclusion: Ultrasound alone carries high misdiagnosis risk for SMM due to atypical presentations. A standardized multimodal protocol (grayscale + Doppler + CEUS + biopsy) is essential for accurate diagnosis. Immediate biopsy is recommended for cancer patients with intramuscular masses showing discordant imaging/history.
Keywords: Ultrasound; Skeletal muscle metastases; Contrast-enhanced ultrasound.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Fang N (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Siyu DY, Wenhao Q, Fang N. Skeletal muscle metastases misdiagnosed as benign tumor by ultrasound: Report of two cases with literature review. Open J Clin Med Case Rep. 2025; 2386.
Case 1 Presentation
A 20-year-old male presented with unexplained left upper abdominal pain persisting for over one month. He had been diagnosed with Acute Myeloid Leukemia (AML) one month prior, experiencing two episodes of high-grade fever (Tmax >39°C) before achieving remission through induction chemotherapy.
Laboratory investigations revealed abnormal hematologic parameters
Lymphocyte ratio 14.3% (ref: 20-50%), monocyte ratio 2.1% (ref: 3-10%), and bone marrow aspirate cytology demonstrating hyperactive proliferation with 35.5% blast cells containing Auer rods, confirming AML.
Imaging studies (Figures 1-4):
Lower limb ultrasound: Revealed multiple hypoechoic masses within the medial compartment of the right thigh and medial left calf musculature, suggestive of schwannoma; CEUS recommended.
CEUS (performed next day): Demonstrated multiple hypoechoic foci in the left calf muscle layer. At 12 seconds post-contrast injection, lesions exhibited heterogeneous hyper-enhancement (> adjacent muscle tissue) with irregular non-enhancing areas.
CEUS conclusion: Enhancement pattern suggestive of benign lesions; core needle biopsy advisable.
The patient then underwent ultrasound-guided core needle biopsy.
Pathological result: Extramedullary leukemia infiltration (myeloid sarcoma).

Figure 1: Multiple echogenic areas were detected in the muscle layer of the left medial calf, all with regular morphology, clear borders, and heterogeneous internal echogenicity.
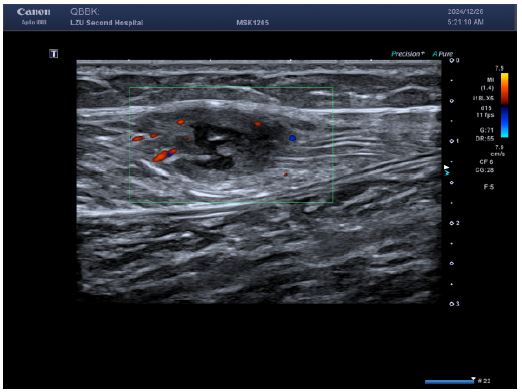
Figure 2: Color Doppler flow imaging showed a small amount of short rod-shaped blood flow around the lesion.
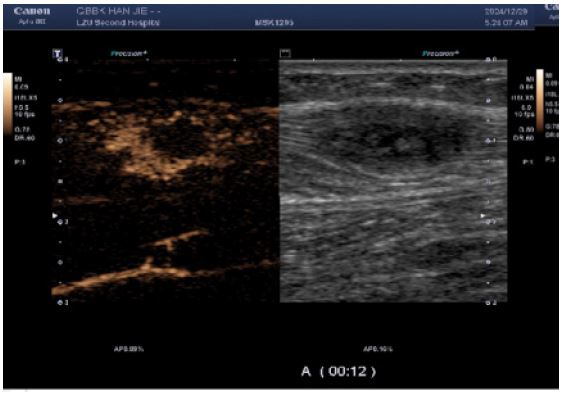
Figure 3: CEUS suggested heterogeneous hyper-enhancement at 12 s of contrast injection.
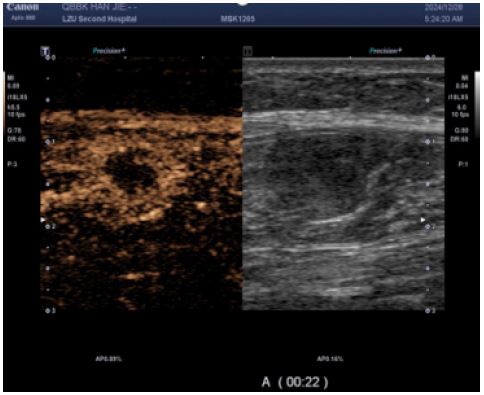
Figure 4: The enhancement borders were clear, and areas of non-enhancement were seen within them; Irregular non-enhancing areas are present throughout the enhancement pattern, consistent with a benign enhancement pattern.
Case 2 Presentation
A 60-year-old male presented with a mass in the medial-posterior aspect of the right calf persisting for >6 months, accompanied by pain for 3 months. He had been diagnosed with Non-Small Cell Lung Cancer (NSCLC) at our institution six months prior. Laboratory studies revealed no abnormalities.
Imaging studies
Lower limb ultrasound: Detected a hypoechoic lesion within the intermuscular space of the right calf. Initial impression: Schwannoma suspected; CEUS recommended.
CEUS (performed next day): Subsequent CEUS performed 24 hours post-initial scan demonstrated heterogeneous enhancement at 25 seconds post-contrast injection, characterized by peripheral hyper-enhancement and a large central non-enhancing area – an imaging pattern misinterpreted as indicative of a benign lesion.
The patient then underwent ultrasound-guided core needle biopsy.
Pathological result: Metastatic poorly differentiated pulmonary adenocarcinoma or adenosquamous carcinoma to the right calf.
Discussion
SMM is exceedingly rare [1]. Histopathologically, SMM may originate from diverse malignancies, with the most frequent primary tumors being lung cancer, renal cell carcinoma, gastrointestinal malignancies, and genital tract neoplasms [2]. The predominant sites involve skeletal muscles of the lower limbs, particularly the thigh and calf musculature [2].
Lung cancer represents a common primary source in such cases, where superficial metastases to the skin and subcutaneous tissues account for 0.75%-9% of tumor disseminations [3]. Notably, SMM may serve as the initial manifestation of occult malignancy, necessitating accurate and early diagnosis. Myeloid Sarcoma (MS) denotes an extramedullary proliferation of one or more types of immature myeloid cells, forming mass lesions that disrupt normal tissue architecture [4]. Historically termed «chloroma» due to its greenish hue derived from myeloperoxidase activity, this entity is now standardized as myeloid sarcoma in the WHO classification [4]. It demonstrates a predilection for children and young adults, with a distinct male predominance [5].
The sonographic presentation of SMM demonstrates considerable heterogeneity with limited documented evidence. Characteristic ultrasound features predominantly include hypoechoic lesions exhibiting round-to-oval or lobulated configurations accompanied by intralesional hypervascularity. Notably, many such metastases mimic abscess morphology through central hypoechogenicity with peripheral rim enhancement [6,7]. Critical discriminators from benign masses on grayscale and color Doppler imaging encompass: lobulated tumor margins, and peripheral pedicle-feeding vessels supplying architecturally disordered intratumoral vasculature [8]. Contrastingly, our two reported cases manifested atypical features diverging from conventional malignant patterns: well-demarcated boundaries with sharp tissue delineation, sparse intranodular vascular signals, and irregular avascular necrotic foci demonstrating both anechoic and non-enhancing properties—likely representing tumor pseudocapsule formation and extensive coagulative necrosis.
Currently, definitive diagnosis of SMM relies predominantly on histopathological examination, as ultrasonographic assessment exhibits inherent limitations. Ultrasonography alone—particularly without clinical history—carries significant misdiagnosis risks; nevertheless, it provides critical guidance for percutaneous biopsies and facilitates treatment response monitoring. In both presented cases, our institution performed a comprehensive ultrasonographic protocol encompassing two-dimensional grayscale imaging, color Doppler flow mapping, CEUS, and ultrasound-guided core needle biopsy, culminating in definitive diagnosis of metastatic malignancies.
The reasons for the misdiagnosis of this patient as a benign tumor were as follows: (1) The initial diagnostic context involved routine ultrasound without documented extramuscular malignancy, precluding sufficient justification for metastatic suspicion; (2) Sonomorphological mimicry manifested as well-circumscribed, spindle-shaped anechoic foci with smooth margins, distinct hyperechoic capsules, and posterior acoustic enhancement within the calf musculature—features pathognomonic for schwannoma yet discordant with the infiltrative borders characteristic of aggressive malignancies; (3) Vascular analysis (Figure B) revealed sparse punctate vascular signals rather than the abundant internal/peripheral flow or large perforating vessels typical of subcutaneous cancers; (4) CEUS kinetics further reinforced misdiagnosis through arterial-phase peripheral hyper-enhancement with central non-enhancing zones, maintained circumscribed margins, and early washout in adjacent tissues—collectively aligning with classical benign enhancement profiles and creating a compelling illusion of non-malignant pathology.
The sonographic features of SMM remain inadequately characterized in current literature, exhibiting limited specificity with considerable overlap across benign musculoskeletal conditions. Nevertheless, documenting these findings holds clinical significance, as patients with known malignancies may be referred for ultrasonographic evaluation of intramuscular masses. In such scenarios, preemptive familiarity with the sonographic hallmarks of SMM may critically inform biopsy triage decisions for indeterminate lesions.
Declarations
Competing interests: The authors have no relevant financial or non-financial interests to disclose.
Ethics statement: This study was approved (or granted exemption) by the ethics committee of LanZhou university second hospital (approval no. 2024A-279). We certify that the study was performed in accordance with the 1964 declaration of HELSINKI and later amendments.
Consent: Consent from the patient was taken to publish their data and images.
Data availability statement: All data generated or analysed during this study are included in this published article.
References
- Surov A, Hainz M, Holzhausen HJ, et al. Skeletal muscle metastases: primary tumours, prevalence, and radiological features. Eur Radiol. 2010; 20: 649-658.
- Lasagna A, Ghiara M, AAM, et al. Skeletal muscle metastases: pitfalls and challenges of a highly inhospitable environment. Future Oncol. 2022; 18: 897-901.
- Perisano C, Spinelli MS, Graci C, et al. Soft tissue metastases in lung cancer: a review of the literature. Eur Rev Med Pharmacol Sci. 2012; 16: 1908-1914.
- Loscocco GG, Vannucchi AM. Myeloid sarcoma: more and less than a distinct entity. Ann Hematol. 2023; 102: 1973-1984.
- Ramia de Cap M, Chen W. Myeloid sarcoma: an overview. Semin Diagn Pathol. 2023; 40: 129-139.
- Salman R, Sebaaly MG, Asmar K, et al. Rare skeletal muscle metastasis from renal cell carcinoma: case report and review of the literature. CEN Case Rep. 2018; 7: 316-319.
- Cha SM, Kim HS, Lee JH, et al. Skeletal muscle metastases of the trunk and pelvis: focus on ultrasound, CT findings, and clinical manifestations. Br J Radiol. 2022; 95: 20220513.
- Lee SJ, Kim OH, Choo HJ, et al. Ultrasonographic findings of the various diseases presenting as calf pain. Clin Imaging. 2016; 40: 1-12.
