
Open Access, Volume 11
Bile duct injury after blunt abdominal trauma – An infrequent consequence of a common problem
Raquel Gomes*; João Mendes; José P Couto; Maria João Koch; Licínio Rego
General Surgery Service, Local Health Unit of Alto Minho, Portugal.
Raquel Gomes
General Surgery Service, Local Health Unit of Alto Minho, Portugal.
Email: fraquel.18@gmail.com
Received : August 07, 2025,
Accepted : September 21, 2025
Published : September 30, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Bile duct injuries resulting from trauma are uncommon and typically occur alongside other injuries. We present a case of polytrauma following a motor vehicle accident. Upon evaluation, the patient exhibited signs of traumatic brain injury, severe pulmonary contusion, lacerations of the liver, and a retroperitoneal hematoma without active hemorrhage. During intensive care follow-up, the patient developed septic shock due to an intra-abdominal abscess. A laparotomy was performed to debride and drain the extensive retroperitoneal hematoma. On the first postoperative day, a high output of biliary fluid was observed in the abdominal drain. The diagnosis of a bile leak was confirmed through Endoscopic Retrograde Cholangiopancreatography (ERCP) with sphincterotomy and bile duct stenting, which facilitated the gradual resolution of the leak.
This case highlights the importance of maintaining a high index of suspicion for bile duct injuries in early diagnosis, as the signs may be subtle, but timely detection can prevent serious complications.
Keywords: Polytrauma; Bile duct injury; Endoscopic retrograde cholangiopancreatography; Hepaticojejunostomy.
Abbreviations: ERCP: Endoscopic Retrograde Cholangiopancreatography; CT: Computed Tomography; ICU: Intensive Care Unit; ARDS: Acute Respiratory Distress Syndrome; ECMO: Extracorporeal Membrane Oxygenation.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Gomes R (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Gomes R, Mendes J, Couto JP, Koch MJ, Rego L. Bile duct injury after blunt abdominal trauma – An infrequent consequence of a common problem. Open J Clin Med Case Rep. 2025; 2382.
Introduction
Bile duct injuries, including bile leaks and stenosis, are uncommon in trauma victims, with an incidence of 3-5%. These injuries are typically associated with penetrating abdominal trauma, while only about 15% occur in cases of blunt trauma.
Most traumatic biliary lesions affect the gallbladder (85%), whereas injuries to the main bile duct are infrequent. These injuries usually occur in polytrauma patients with multiple injuries and can be particularly dangerous as they may go unnoticed. Such injuries are most commonly associated with hepatic lesions but may also be linked to duodenal, pancreatic, or other injuries. They are often identified belatedly, even in patients who undergo surgical exploration, which can increase the risk of complications and morbidity [1].
In this case report, we present a patient who experienced blunt abdominal trauma with splenic and hepatic lacerations that developed a bile duct leak, which became clinically apparent only one month after the trauma.
Case Presentation
A male in his early 50s was involved in a high-velocity car crash, resulting in cranial, thoracoabdominal, and extremity trauma.
He was admitted to the emergency room of a central hospital in a hemodynamically stable condition, with a Glasgow Coma Scale score of 15. A whole-body CT scan revealed a small subarachnoid hemorrhage, multiple bilateral rib fractures coupled with severe pulmonary contusion, and a small left pneumothorax. Abdominal CT findings indicated a grade II hepatic laceration involving segments IV, V, and VI, a grade I splenic laceration, and a retroperitoneal hematoma without active hemorrhage, as well as a left acetabular fracture.
The patient underwent conservative management for his abdominal injuries and received ventilatory support, being admitted to the Intensive Care Unit (ICU). Within the first few hours of admission, he developed Acute Respiratory Distress Syndrome (ARDS) and was transferred to another Trauma I Center for Extracorporeal Membrane Oxygenation (ECMO) support.
One month after admission, and while still intubated, the patient was readmitted to his original hospital. Upon readmission, he presented with fever and significantly elevated inflammatory markers. A thoraco-abdominal CT scan revealed a multiloculated hematoma in the right quadrants of the abdomen, with no signs of active bleeding. Percutaneous drainage of the collection yielded abundant purulent content.
Three days later, the patient was extubated and transferred to a hospital closer to his residence. Upon arrival, clinical deterioration occurred, characterized by cardiovascular and neurological dysfunction, necessitating reintubation. The previously purulent abdominal drainage had changed to enteric characteristics, prompting a new CT scan, which indicated a multiloculated retroperitoneal collection extending from the right flank to the pelvis, suggestive of bowel perforation (Figure 1). The patient was taken for laparotomy, during which a large infected retroperitoneal hematoma was identified and extensively debrided and bowel perforation was ruled out. Two drains were placed in the right flank and peri-hepatic space. The surgery proceeded without complications. However, on the first postoperative day, a high output of biliary content was noted in the abdominal drains. Bilirubin analysis of the drain’s contents confirmed the presence of biliary drainage.
The biliary drainage indicated a high-output bile leak (maximum drainage of 1500 mL per day).
Several days after surgery and once the patient was stabilized, an Endoscopic Retrograde Ccholangiopancreatography (ERCP) was performed. This revealed a high-output bile leak in the distal portion of the main bile duct. The procedure included a sphincterotomy and the placement of a metal bile duct stent (Figure 2).
Following the ERCP, the drainage output decreased, allowing for the removal of the abdominal drains one week later. The patient was discharged four months after admission. At the time of discharge, the patient’s condition had significantly improved, but they still required ongoing rehabilitation.
During follow-up, the patient presented with multiple episodes of cholangitis with repeated ERCPs and biliary stenting due to a short biliary stenosis in the distal portion of the bile duct.
Due to the persistence of bile duct stenosis and recurrent episodes of cholangitis, definitive surgical treatment with a Roux-en-Y hepaticojejunostomy was performed. There were no significant complications in the postoperative period, and the patient is now under clinical follow-up.
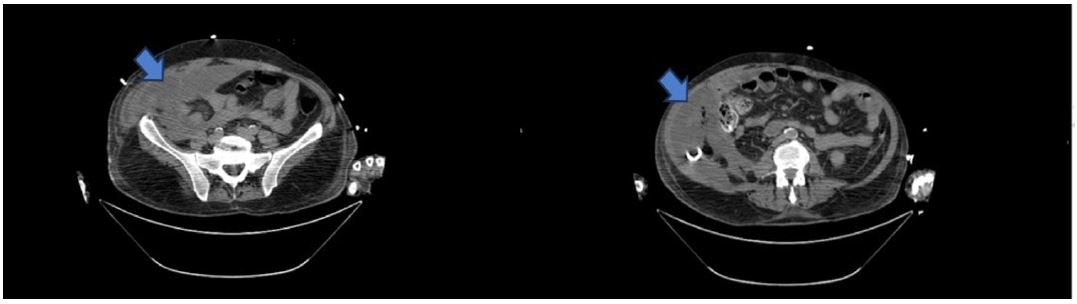
Figure 1: Abdominopelvic CT scan previous to the exploratory laparotomy: Evidence of a multiloculated retroperitoneal collection (arrow) extending from the right flank till the pelvis with a heterogeneous aspect.
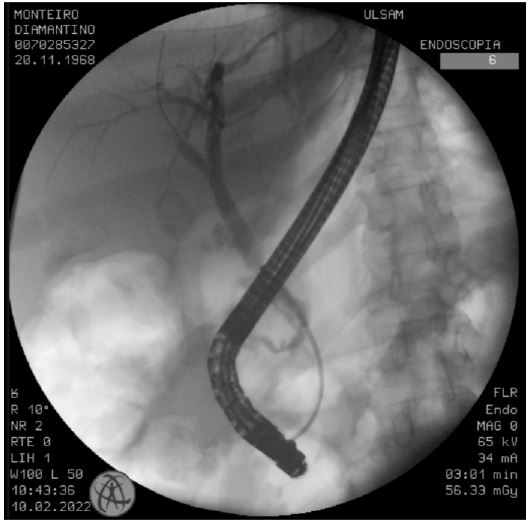
Figure 2: Image of the ECRP done for treatment of the bile duct leak.
Discussion
Bile duct injuries can occur in the intrahepatic portion of the biliary tree, which is typically associated with concurrent hepatic lesions, or in the extrahepatic portion of the bile duct. The latter is rare in trauma cases and usually occurs in the fixed sections of the bile duct. Various mechanisms can lead to the rupture of the main bile duct, including compression against the vertebral column, rupture due to a sudden increase in gallbladder pressure associated with a short cystic duct, and laceration at the junction of the bile duct and the pancreas [1,2].
The diagnosis of biliary lesions can occur early in patients undergoing exploratory laparotomy for concomitant injuries if there is evidence of bile extravasation during the procedure [3]. However, most cases often go unnoticed as imaging findings can be subtle, particularly in incomplete lesions. These injuries can also manifest later, even months after the initial trauma. In the case presented, the biliary lesion was detected only one month after the accident, and there was no suspicion of a bile duct injury during the surgery. Such injuries can arise not only from direct trauma to the biliary tree but also from ischemic lesions due to the devascularization of the bile ducts [2].
Consequently, diagnosing bile duct injury in a trauma context requires a high index of suspicion. It should be considered when there is worsening abdominal pain or distension in patients who develop jaundice or exhibit elevated cholestasis parameters, or when there is a change in the content of an abdominal drain [1].
Regarding treatment, unlike iatrogenic bile duct injuries, which have established management guidelines, there is no consensus on the best approach for biliary lesions occurring in a trauma context. This variability is due to the rarity of these injuries, their late detection, and the potential complications arising from concurrent lesions [4,5]. Thus, the initial management of bile duct injuries depends on the patient’s hemodynamic stability. In hemodynamically unstable patients, surgical exploration is essential to prevent late complications. In stable patients, there is time for a comprehensive evaluation to find all concomitant injuries [2].
Despite the low frequency of these injuries, it is well established that minor bile leaks can often be managed conservatively, allowing for spontaneous resolution. However, managing major injuries can be more complex. In such cases, early bile flow diversion is crucial to prevent complications like infected biloma or biliary peritonitis. The mainstays of treatment for bile duct injuries associated with blunt abdominal trauma are percutaneous drainage and endoscopic treatment with Endoscopic Retrograde Cholangiopancreatography (ERCP). When conservative management fails, surgical intervention is necessary, with Roux-en-Y hepaticojejunostomy being the standard procedure [5-8].
Conclusion
In trauma context it is important to maintain a high index of suspicion for bile duct injuries to allow an early diagnosis, as the clinical signs may be subtle, but timely detection can prevent serious complications. Conservative management allows the resolution of the majority of cases but when it fails surgical intervention with Roux-en-Y hepaticojejunostomy is the standard treatment.
References
- Balzarotti R, Cimbanassi S, Chiara O, Zabbialini G, Smadja C. Isolated extrahepatic bile duct rupture: a rare consequence of blunt abdominal trauma. Case report and review of the literature. World Journal of Emergency Surgery. 2012; 7:16.
- Yun Chul Park, Young Goun Jo, Wu Seong Kang, Eun Kyu Park, Hee Jun Kim, Jung Chul Kim. Isolated Common Hepatic Duct Injury after Blunt Abdominal Trauma. J Trauma Inj. 2017; 30(4):231-234.
- Sanford Z, Abdolmaali K, Robinson D, Denning D. Blunt trauma: An uncommon cause of common bile duct injury. Trauma Case Rep. 2015; 1: 44–48.
- Angelis N, Catena F, Memeo R, Coccolini F, Pérez A, Romeo A, et al. 2020 WSES guidelines for the detection and management of bile duct injury during cholecystectomy. World Journal of Emergency Surgery. 2021; 16: 30.
- Zakaria H, Oteem A, Gaballa N, Hegazy O, Nada A, Zakareya T, et al. Risk factors and management of different types of biliary injuries in blunt abdominal trauma: Single-center retrospective cohort study. Annals of Medicine and Surgery. 2020: 36–4.
- Hommes M, Kazemier G, Schep N, Kuipers E, Schipper I. Management of biliary complications following damage control surgery for liver trauma. Eur J Trauma Emerg Surg. 2013; 39: 511-6.
- Maestre M, Bengoechea A, Lizandro A, Ramos C, Serrano JL. Complicaciones en el manejo conservador del traumatismo hepático cerrado: fístula biliar, hemobilia y biloma. Cir Esp. 2013; 91: 537–539.
- Ghosh S, Kazi F, Sharma J. Extrahepatic Bile Duct Injury caused by Blunt Abdomen Trauma: A case report. Cureus. 2022; 14: e25662.
