
Open Access, Volume 11
Sunitinib induced thrombocytopenic purpura
Dong Hyun Lim*; Mi Hwa Heo; Jin Young Kim
Department of Hematology-Oncology, Keimyung University School of Medicine, South Korea.
Dong Hyun Lim
Department of Hematology-Oncology, Keimyung University School of Medicine, South Korea.
Email: hyunly12@naver.com
Received : August 08, 2025,
Accepted : September 15, 2025
Published : September 30, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Sunitinib is an oral, multi-targeted tyrosine kinase inhibitor which has anti-tumor and anti-angiogenic activities due to selective inhibition of several growth factor receptors. Sunitinib is approved for the first line treatment for Metastatic Renal Cell Carcinoma(mRCC), which used widely until now. However, it can cause several adverse reactions, including diarrhea, fatigue, nausea, stomatitis, vomiting, hypertension, hand-foot syndrome, neutropenia, anemia, increased creatinine, and thrombocytopenia, and it is important to aware these side effects for early detection and management of side effects. In this case, we present a case of thrombocytopenic purpura while treating with sunitinib therapy for metastatic clear renal cell carcinoma, with systematic review.
Keywords: Sunitinib; Thrombocytopenic purpura; Renal cell carcinoma; Hemolytic uremic syndrome; Tyrosine kinase inhibitor.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Lim DH (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Lim DH, Heo MH, Kim JY. Sunitinib induced thrombocytopenic purpura. Open J Clin Med Case Rep. 2025; 2380.
Introduction
Sunitinib is an oral, multi-targeted Tyrosine Kinase Inhibitor (TKI) which has anti-tumor and anti-angiogenic activities due to selective inhibition of several growth factor receptors. It potentially inhibits activation of receptors like Vascular Endothelial Growth Factor Receptors (VEGFR-1,-2,-3), platelet Derived Growth Factor Receptors (PDGFR –α and –β), stem cell factor receptor (KIT), Fms-Like Tyrosine kinase-3 (FLT3), Colony Stimulating Factor receptor type 1 (CSF-1R), and glial cell-line-derived neurotrophic factor receptor (RET), which are required for tumor cell proliferation against hypoxia [1,2]. It is clinically used in the treatment of several cancers, like metastatic Renal Cell Carcinoma (mRCC) [2], pancreatic neuroendocrine tumor [1], and imatinib resistant metastatic gastrointestinal stromal tumor [3].
Recently, several combination treatments are regarded as first line treatment for mRCC: the combination of two Immune Checkpoint Inhibitors (ICI) or an ICI with TKI combination or single agent TKI [13]. Although the combination of two ICI is preferred as the first choice for treat mRCC in Korea, TKI like sunitinib has been used for a long time for managing mRCC, and it is important to understand the characteristic of this agent.
Sunitinib has several side effects, including diarrhea, fatigue, nausea, stomatitis, vomiting, hypertension, hand-foot syndrome, neutropenia, anemia, increased creatinine, and thrombocytopenia. Sunitinib interferes with multiple intracellular tumorogenic pathways, and hypotheses for side effects include anti-angiogenesis effect leads to the potential for side effects by preventing adequate blood flow to normal tissues at a time of injury, increasing vascular resistance and endothelial dysfunction, and decreasing vascular compliance [4]. Thrombotic Thrombocytopenic Purpura-Hemolytic Uremic Syndrome (TTP-HUS) is rarely occurred during treated with sunitinib, but it can be severe and fatal. Here we describe the case of a patient with mRCC who developed TTP-HUS during treated with sunitinib.
Case Report
A 77-year-old man had diagnosed for 9 cm sized renal cell carcinoma, poorly differentiated with sarcomatoid differentiation and necrosis at left kidney, which involved renal pelvis and ureter in march, 2021. Additional image work up showed metastasis to liver, so he had been treated for 4 weeks with 50mg of sunitinib daily orally on a 4-week-on and 2-week-off schedule since April, 2021. At the time when he visited emergency room, sunitinib was not taken for few weeks. He also diagnosed for Pulmonary Thromboembolism (PTE), so he was treated with New Oral Anticoagulant (NOAC) for a month. He had no other major previous illness.
He visited to emergency room due to dyspnea for 5 days at may, 2021. On clinical examination, he had pale conjunctiva with severe lower limb pitting edema, skin necrosis at both foot and both hands, but no remarkable neurologic symptoms. His blood pressure was 137/72 mmHg; pulse rate, 94 beats per minute; and respiratory rate, 20 breaths per minute, and temperature was 36.2℃.
He was found to have severe thrombocytopenia, and anemia. The hemoglobin concentration was 5.0 g/dL, platelet count was 12,000/μL, reticulocyte count was 5.72 %, and the peripheral blood smear showed schistocytes (>2%) (Figure 1). Lactate Dehydrogenase (LDH) was 1890 U/L, and the coombs direct and indirect tests were negative. He also had electrolyte imbalance and azotemia, hypoproteinemia: sodium was 138 mmol/L, potassium was 5.6 mmol/dL, calcium was 7.0 mg/dL, phosphorus was 4.9 mg/dL, BUN was 74 mg/dL, Creatinine was 4.25 mg/dL, total protein 4.7 g/dL, albumin 1.8 g/dL. He also had coagulopathy: PT INR 1.51, APTT 37.0 seconds, fibrinogen 109.9 mg/dL. Moreover, his lab showed elevated C-Reactive Protein (CRP) (8.5 mg/dL) and cardiac markers: CK-MB 6.51 ng/mL, Troponin I 0.47 ng/mL, NT ProBNP 7407 pg/mL. A urinalysis showed albuminuria (1+), Pyuria (2+).
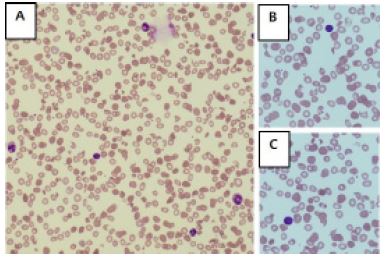
Figure 1: PB smear of patient. (A) x400; (B,C) x1000.
After administration, his symptoms (general weakness, mental drowsiness, skin necrosis) got worse, and laboratory test results showed microangiopathic hemolytic anemia (MAHA) and thrombocytopenia. Red Blood Cell (RBC), platlet transfusion was done. Meanwhile, additional laboratory test was done: ADAMTS13 (a disintegrin and metalloprotease with thrombospondin type 1 repeats member 13) was 20.9, haptoglobin was <10 mg/dL. These findings were suspected to be due to sunitinib induced TTP. Renal Replacement Therapy (RRT) was initiated, because of aggravation of azotemia with poor urine output. Followed lab showed improvement for anemia, but thrombocytopenia got worse. He showed confused mentality, skin and soft tissue necrosis with no improvement despite continuing RRT, drug withdrawal, antibiotics covering and conservative manage. Plasmapheresis was done for managing TTP. Followed lab showed improvement of thrombocytopenia and coaguloapthy, but it discontinued because of cost issue (Figure 2).
After discontinuing plasmapheresis and RRT, Thrombocytopenia, fever, dyspnea with increased O2 demand, were observed. Poor prognosis was implicated, and Physicians Opinion for Life Sustaining Treatment (POLST) was completed since patient didn’t want life suspending treatment. After few days, he expired.
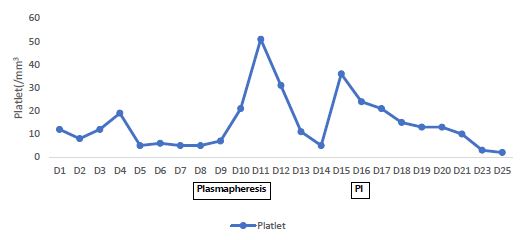
Figure 2: Response to plasmapheresis.
Discussion
Multiple TKI, targeting either the Vascular Endothelial Growth Factor (VEGF) and VEGR-receptors, or the Mammalian Target of Rapamycin (mTOR) pathways has improved the outcome of treatment of mRCC dramatically [13]. Generally, Adverse events reported in patients with mRCC who received TKI like sunitinib are diarrhea, fatigue, nausea, stomatitis, vomiting, hypertension, hand-foot syndrome, neutropenia, anemia, increased creatinine, and thrombocytopenia [4]. These were well tolerated, since its severity is mild to moderate [5]. However, adverse reactions like TTP-HUS are not well announced, but it can be critical to patients.
Basically, TTP-HUS is a kind of thrombotic microangiopathy (TMA) that has features of thrombocytopenia with Microangiopathic Hemolytic Anemia (MAHA) with or without multiple organ damage [5,6]. Several conditions like malignant hypertension, sepsis, disseminated cancer, pregnancy with or without preeclampsia or the HELPP (hemolysis, elevated liver enzyme levels and a low platelet count) syndrome can induce Thrombotic Microangiopathy (TMA) [6]. Chemo-therapeutic agents like mitomycin C, cisplatin, bleomycin, doxorubicin, 5-fluorouracil, interferon-alfa, carboplatin, daunorubicin, dacarbazine, oxaliplatin, vinblastine, cytarabine, and gemcitabine can also cause TMA [5]. It is thought to be due to excess fragmentation of erythrocytes passing through the narrowed vascular lumen with fibrinoid necrosis and perivascular edema, and an excess consumption of platelets activated by the injured endothelium [6].
The pathophysiology of TTP-HUS due to sunitinib is not very well known. It is thought that Sunitinib damages the capillary endothelium, especially to renal endothelial cell injury from VEGF starvation of the podocytes, which then results in endothelial cell death and disruption of the endothelial barrier that causes platelet activation and aggregation along with thrombin deposition, thus leading to thrombocytopenia and hypofibrinogenemia [8]. It has been demonstrated that damaged renal endothelium caused a pronounced platelet influx into the glomeruli and peritubular capillaries, and it was followed by large fibrin thrombus accumulation consistent with the histology of severe thrombotic microangiography [12].
About 6 cases has been previously reported which described TTP-HUS associated with sunitinib [5-7]. Clinical features of the previous reports about anti-VEGF agents associated TTP-HUS are showed in (Table 1) [5-7,9,10,12]. It shows that all patients in these cases presented renal complications, and do not seem to be dose-dependent [11].
According to previously reported cases, The prognosis of TTP-HUS associated with sunitinib was very good, except one case: Talebi et al. Described case of microangiopathic hemolytic anemia associated with sunitinib, which was the first case with fatal outcome despite treatment with plasmapheresis, dialysis, and withdrawal of sunitinib.
Difference between cases with improved course and worsened course are follows: First, cases eventually got worsen in spite of withdrawal of sunitinib with following dialysis and plasmapheresis were with infection. The case which was reported by Talebi et al. [12], had ascending colon colitis. In this case, patient had soft tissue necrosis at both feet and hands. All of these cases had antibiotic therapy initially, but there was no improvement despite treatment. In contrast, other cases which didn’t present signs of infection, or had viral infection with appropriate anti-viral agent treatment had good prognosis with or without plasmapheresis [5-7,9,10] (Table 1). Secondly, plasmapheresis was not initially done due to insurance guideline made by Health Insurance Review and Service (HIRS) in Korea. In guideline, plasmapheresis should be started after checking diagnostic test for TTP/HUS like ADAMTS13, which takes several days. It delays treatment for TTP/HUS, and it may induce poor outcomes. Moreover, HIRS previously cut off cost for continued plasmapheresis when treating TTP/HUS. In this case, plasmapheresis was done after 8 days of admission, continued for about 4 days, with meaningful improvement. If it were continued, the outcome could be better, since thrombocytopenia got better while it was done.
Table 1: Summary of literature reporting thrombotic thrombocytopenic purpura-hemolytic uremic syndrome associated with sunitinib.
| Authors (Yr) | Age / Gender | Malignancy | Sx, signs, laboratory findings | Time interval after start of treatment | ADAMTS13 activity | Management | Outcome |
|---|---|---|---|---|---|---|---|
| Kapiteijn et al. (2007) | 54 / F | GIST | Loss of vision, epileptic insults, hypertension, azotemia, RPLS | 7 mos | 40% | Withdrawal, plasma infusion | Recovered |
| Frangie et al. (2008) | 70 / M | RCC | Asthenia, hypertension, nausea, edema, renal insufficiency | 3 wks | 27% | Withdrawal, plasma exchange | Recovered |
| Choi et al. (2008) | 62 / F | RCC | Hematuria, edema, anorexia, nausea, dyspepsia, petechia | 3 wks | Not described | Withdrawal, plasma exchange | Recovered |
| Talebi et al. (2012) | 68 / M | RCC | Nausea, malaise, weakness, fever, renal failure, azotemia | 31 mos | 22% | Withdrawal, plasma exchange, dialysis | Expired |
| Kim et al. (2013) | 53 / F | RCC | Weakness, fever, cough, sputum | 33 mos | 56% | Withdrawal, plasma exchange | Recovered |
| Imane et al. (2014) | 73 / F | RCC | Epistaxis, fatigue | 4 wks | Not described | Withdrawal, plasma exchange | Recovered |
| This case | 77 / M | RCC | Dyspnea, general weakness, fever | 4 wks | 21% | Withdrawal, plasma exchange, dialysis | Expired |
To sum up, oncologists should be aware that TKI targeting anti-VEGF like sunitinib can cause potentially fatal TMA like TTP-HUS, especially when infection is combined. Also, institutional support should be made for maintaining appropriate manage like plasmapheresis to achieve better outcomes for treating sunitinib induced TTP-HUS.
Conclusion
This is the second case report on occurrence of TTP-HUS, which had worsened outcomes despite early intervention. With comparing of other cases, Oncologists should be aware that sunitinib may cause potentially fatal TTP-HUS, especially when it comes with infection.
References
- Raymond E, Dahan L, Raoul JL, et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med. 2011; 334: 501-513.
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007; 356: 115-124.
- Demetri GD, van Oosterom AT, Garrett CR, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumor after failure of imatinib: a randomized controlled trial. Lancet. 2006; 368: 1329-1338.
- Schwandt A, Wood LS, Rini B, Dreicer R, et al. Management of side effects associated with sunitinib therapy for patients with renal cell carcinoma. Onco Targets Ther. 2009; 2: 51-61.
- Choi MK, Hong JY, Jang JH, Lim HY. TTP-HUS associated with sunitinib. Cancer Res Treat. 2008; 40: 211-213.
- Kapiteijn E, Brand A, Kroep J, Gelderblom H. Sunitinib induced hypertension, thrombotic microangiopathy and reversible posterior leukencephalopathy syndrome. Ann Oncol. 2007; 18: 1745-1747.
- Frangie C, Lefaucheur C, Medioni J, Jacquot C, Hill GS, Nochy D. Renal thrombotic microangiopathy caused by anti-VEGF-antibody treatment for metastatic renal-cell carcinoma. Lancet Oncol. 2007; 8: 177-178.
- Eremina V, Jefferson JA, Kowalewska J, Hochster H, Haas M, Weisstuch J, et al. VEGF inhibition and renal thrombotic microangiopathy. N Engl J Med. 2008; 358: 1129-1136.
- Kim EJ, Choi YM, Lee SW, Ha YJ, Lee JL. A case of sunitinib-associated thrombotic thrombocytopenic purpura. Korean J Med. 2013; 84: 2.
- El Dika I, Mukherji D, Temraz S, Assi R, Shamseddine A. Sunitinib induced thrombotic thrombocytopenic purpura in addition to severe hypothyroidism: a case report and review of the literature. Case Rep Med. 2014; 958414: 1-4.
- Dlott JS, Danielson CFM, Blue-Hnidy DE, McCarthy LJ. Drug-induced thrombotic thrombocytopenic purpura/hemolytic uremic syndrome: a concise review. Ther Apher Dial. 2004; 8: 102-111.
- Talebi TN, Stefanovic A, Merchan J, Lian E, Silva O. Sunitinib-induced microangiopathic hemolytic anemia with fatal outcome. Am J Ther. 2012; 19: e143-e145.
- Tran J, Ornstein MC, et al. Clinical review on the management of metastatic renal cell carcinoma. JCO Oncol Pract. 2022; 18: 3.
