
Open Access, Volume 11
Peritoneal dialysis associated infection caused by a novel Mycolicibacterium (Mycobacterium) species
Bojana Simsic1,2*; Genevieve E Martin1,3,4; Alyssa Fitzpatrick1,5; Max Cummins2; Dimitrios Menouhos2; Maria Globan6; Ella M Meumann1,2,3; Robert W Baird1,2; Sze Yen Tay1,7
1Infectious Diseases Department, Royal Darwin Hospital, Northern Territory, Australia.
2Territory Pathology, Royal Darwin Hospital, Northern Territory, Australia.
3Global and Tropical Health Division, Menzies School of Health Research, Charles Darwin University, Darwin, Northern Territory, Australia.
4Department of Infectious Diseases, University of Melbourne, Melbourne, Australia.
5Department of Infectious Diseases, Women’s and Children’s Hospital, Adelaide, South Australia, Australia.
6Mycobacterium Reference Laboratory, Victorian Infectious Diseases Reference Laboratory, Melbourne, VIC, Australia.
7Department of Infectious Diseases, The Canberra Hospital, ACT, Australia.
Bojana Simsic
The Canberra Hospital, Infectious Diseases Department, Royal Darwin Hospital, Yamba Drive, Garran,
Australian Capital Territory 2605, Australia.
Tel: +61-8-89228888, +61-2-51240000;
Email: bo.simsic@gmail.com
Received : July 20, 2025,
Accepted : August 13, 2025
Published : August 29, 2025,
Archived : www.jclinmedcasereports.com
Abstract
We report a case of a 64-year-old man with end-stage renal failure who was diagnosed with peritoneal dialysis-associated peritonitis caused by a novel species in the genus of Mycolicibacterium (Mycobacterium). This rapidly growing non-tuberculous mycobacterial species was repeatedly isolated from peritoneal fluid. The patient’s symptoms failed to improve despite empirical intraperitoneal antibiotics of cefazolin and ceftazidime, until the removal of the Tenckhoff catheter and commencement of a four-month course of antimycobacterial treatment. Initially identified as M. litorale using Sanger sequencing and analysis of the 16S rRNA, Whole Genome Sequencing (WGS) and genomic analysis revealed instead a novel isolate most closely related to M. litorale that is yet to be taxonomically defined. More than six months after the cessation of antimicrobials, the patient remains well and has been referred for consideration of renal transplantation. This novel Mycolicibacterium species is likely of low virulence but has potential to cause prosthesis-associated infections.
Keywords: Mycolicibacterium litorale; Novel mycolicibacterium; Non-tuberculous mycobacteria; Rapid growing mycobacteria; Prosthesis-associated infection; Catheter-associated peritonitis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Simsic B (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Simsic B, Martin GE, Fitzpatrick A, Cummins M, Menouhos D, et al. Peritoneal dialysis associated infection caused by a novel Mycolicibacterium (Mycobacterium) species. Open J Clin Med Case Rep. 2025; 2374.
Introduction
Rapidly Growing Mycobacteria (RGM) are a large heterogeneous group of environmental organisms which can cause opportunistic pulmonary, skin and soft tissue, and less commonly prosthetic device-related infections [1,2]. There are over 75 species of RGM recognised which are grouped into six major taxonomic groups according to pigmentation and genetic relatedness. Both the number of species and their roles in human diseases continue to grow [3]. Here, we report a case of peritoneal dialysis-associated peritonitis due to a novel Mycolicibacterium (Mycobacterium) species related to Mycolicibacterium litorale.
Case Presentation
A 64 year-old livestock systems manager, living in Darwin with end-stage renal failure, presented with two days of fevers and lateral abdominal pain two months after starting peritoneal dialysis. Peritoneal fluid had a leucocyte count of 3400×106 cells/mL (mixed neutrophil 48% / mononuclear 51% infiltrate). After 4 days of incubation at 35oC in 5% CO2, bacterial colonies were noted on horse blood and chocolate agar plates. Gram stain demonstrated a beaded and poorly staining Gram-positive bacillus. Although non-pigmented on blood agar, the isolate produced a yellow-orange pigment on a Lowenstein-Jensen slope (Figure 1A), and Ziehl-Neelsen stain was positive, indicating the growth of a RGM.
Repeat peritoneal fluid cultures taken on the first four days of admission were persistently positive with the same isolate, and the patient’s symptoms and peritoneal fluid leucocyte count failed to improve despite empirical intraperitoneal cefazolin and ceftazidime. Following identification of a RGM on day six, the patient’s Tenckhoff catheter was removed, and he was commenced on empirical antimycobacterial treatment active against common RGMs such as M. fortuitum and M. chelonae [5]. The patient was treated empirically with a 4-drug regimen of cefoxitin, trimethoprim/sulfamethoxazole, linezolid and ciprofloxacin.
Sanger sequencing and analysis of the 16S rRNA and Internal Transcribed Spacer (ITS) genes of the isolate showed 100% Basic Local Alignment Search Tool (BLAST) nucleotide sequence identity with M. litorale. M. litorale is a recently identified RGM and phylogenetic analyses have placed it closely to other RGMs including M. fortuitum, M. monacense and M. doricum (98.2%, 98.0% and 97.9% 16S rRNA gene sequence similarity, respectively) [4]. Cefoxitin was ceased after six days, when this result became available, based on the susceptibility profile of a similar species in a case report [5,6]. The minimum inhibitory concentrations (MICs, ug/mL) as determined by broth microdilution were Clarithromycin, 2; Trimethoprim/Sulfamethoxazole, 8/152; Linezolid, 2; Doxycycline, 0.5; Imipenem,16; Amikacin, 1; Tigecycline, 0.5; and no inducible macrolide resistance was detected after 14-day incubation. Based on the MICs, trimethoprim/sulfamethoxazole was replaced by doxycycline.
Due to adverse drug reactions including visual changes, anaemia and diarrhea, linezolid was ceased after six weeks. Dual therapy with ciprofloxacin and doxycycline was continued to complete four months of treatment following Tenckhoff catheter removal. More than six months after the cessation of antimicrobials, the patient remains well with no evidence of relapse.
Subsequently, Whole Genome Sequencing (WGS) and genomic analysis revealed the isolate as a novel Mycolicibacterium species related to M. litorale. The genome, hereby referred as TPG_MSP_01, was found to share 99.57% nucleotide identity with a Mycolicibacterium sp (NIID-NTM18, accession AP023287) isolated from an infected cardiac device in 2020 which was also initially thought to be M. litorale [5,6]. It shares 88.11% nucleotide identity with the reference genome of the M. litorale type strain JCM 17423 (accession GCF_010731695.1) (Figure 1B) [4,6,7]. The TPG_MSP_01 genome has been uploaded to the National Centre for Biotechnology Information (NCBI) Sequence Read Archive under BioProject ID PRJNA1248661. Detailed methods are described in the Supplementary Appendix.
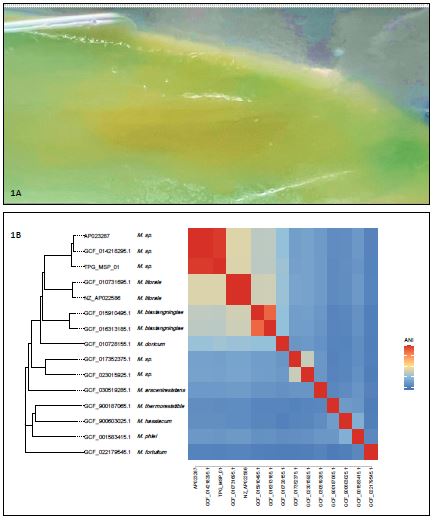
Figure 1: (A) M. litorale clinical isolate Mycololicibacterium spp. clinical isolate growing on a Lowenstein-Jensen slope. Noting the isolate produced a yellow-orange pigment. (B) Distance-based tree including TPG_MSP_01 in the context of related Mycolicibacterium spp. Heatmap shows pairwise average nucleotide identity comparisons.
Discussion
Mycobacteria rarely cause peritonitis but should be considered if standard bacterial cultures are negative or mycobacterial infection is suspected [8]. NTM peritonitis represents less than 1% of reported PD-related peritonitis, however delays in diagnosis, drug toxicities and intrinsic antimicrobial resistance contribute to poor outcomes [9]. M. fortuitum, M. chelonae and M. abscessus abscessus are the most commonly isolated mycobacteria causing catheter-related peritonitis [8,10].
Previous episodes of peritonitis with NTM, recent use of intraperitoneal antimicrobials and exit site infections have been identified as risk factors of PD-related NTM peritonitis [9]. Although routine blood agar cultures are capable of isolating RGM, acid-fast bacilli staining, selective media and extending incubation period can increase the detection of mycobacterial species [10].
Taxonomic characterisation of mycobacteria is evolving as whole genome sequencing has become increasingly accessible and thereby enabling greater resolution of mycobacterial species in comparison to sequencing of single genes [11,12]. This has led to taxonomic reclassification and change of taxonomic relationships of many mycobacterial species [11]. Our genomic analysis indicated that our isolate (TPG_MSP_01) belongs to a distinct, and to our knowledge as-yet taxonomically undefined, species of Mycolicibacterium. Notably, the initial analyses using 16S RNA sequencing in our case, and the use of heat shock protein 65 and RNA polymerase beta subunit gene sequencing performed in a previously published report of a pacemaker infection, had originally identified M. litorale as the causative pathogen instead [5,6]. This highlights the limitations of single gene sequencing which can have difficulty distinguishing closely-related bacterial species [13]. Extensive PubMed search has not found any published clinical cases attributed to M. litorale infection.
Clinical breakpoints for antimicrobial susceptibility for RGM as a group are available from Clinical and Laboratory Standards Institute (CLSI), but individual species breakpoints are yet to be defined for all active antimicrobials. Reproducibility of MICs results can be difficult and clinical correlations to in-vitro susceptibilities may be poor, hence clinical management is based largely on expert opinions [12,14]. Previous case series on NTM catheter-associated peritonitis have reported a wide-ranging treatment durations with most recommending early catheter removal. The 2022 International Society for Peritoneal Dialysis guidelines recommends treatment duration of a minimum of 6 weeks with two active drugs in addition to catheter removal to avoid relapse, recurrence and long term peritoneal membrane damage [8]. Our patient’s infection responded to a combination of device removal and targeted drug regimen over 4 months (a duration chosen on shared decision making with the patient). The first reported case recovered after cardiac device removal and 4 months of treatment involving 1 month of empirical imipenem, amikacin, clarithromycin and sitafloxacin, followed by 3 months of targeted treatment with clarithromycin, sitafloxacin and doxycycline. Both cases presented with minimal clinical symptoms despite significant bacterial burden suggesting opportunistic infections caused by a low-virulence pathogen.
Conclusion
We report a second case of infection caused by a novel Mycolicibacterium sp. most closely related to M. litorale. This species is yet to be taxonomically defined and has been submitted to NCBI. Although there are no clinical breakpoints, the patient made good recovery on a combination of device removal, and treatment with linezolid, ciprofloxacin and doxycycline.
Declarations
Author contributions: Writing of initial manuscript was performed by BS, GEM, MC, DM, SYT, RB and EM. BS, GEM, AF and SYT were responsible for the clinical care of the patient. RWB, EM, MC, MG and DM were responsible for pathogen identification, antimicrobial susceptibility testing, whole genome sequencing and analysis and interpretation of these results. All authors have reviewed and approved the final version.
Acknowledgments: We would also like to acknowledge the contribution of Mr. Rolf Nilsson who has provided permission to share his story in this report and who played an important role in the shared decision-making process. We also acknowledge the contributions of all colleagues who were involved in the clinical management of this case.
Conflict of interest: The authors have no competing interests to declare.
Funding source: The authors received no funding for this project.
Ethical approval: Exemption from full Human Research Ethics Committee (HREC) review was granted for this project by NT Health in line with policy for publication of case reports of the the Human Research Ethics Committee of the Northern Territory Department of Health and Menzies School of Health Research. The application for exemption specifically included a request to include the name of the patient.
References
- Tortoli E. Clinical manifestations of nontuberculous mycobacteria infections. Clin Microbiol Infect. 2009; 15: 906–10.
- Hussein AA, Baghdy Y, Wazni OM, Brunner MP, Kabbach G, Shao M, et al. Microbiology of cardiac implantable electronic device infections. JACC Clin Electrophysiol. 2016; 2: 498–505.
- Brown-Elliott BA, Philley JV. Rapidly growing mycobacteria. [Reference incomplete – journal/book details missing].
- Zhang Y, Zhang J, Fang C, Pang H, Fan J. Mycobacterium litorale sp. nov., a rapidly growing mycobacterium from soil. Int J Syst Evol Microbiol. 2012; 62: 1204–7.
- Miyama H, Takatsuki S, Fukano H, Uwamino Y, Hasegawa N. Infection of a cardiac implantable electronic device caused by Mycolicibacterium litorale. JACC Case Rep. 2020; 2: 277–8.
- Fukano H, Miyama H, Takatsuki S, Hirabayashi A, Suzuki M, Yoshida M, et al. Complete genome sequence of Mycolicibacterium sp. strain NIID-NTM18, isolated from cardiac implantable electronic device infection and most similar to Mycolicibacterium litorale. Microbiol Resour Announc. 2020; 9: e00830-20.
- Matsumoto Y, Kinjo T, Motooka D, Nabeya D, Jung N, Uechi K, et al. Comprehensive subspecies identification of 175 nontuberculous mycobacteria species based on 7547 genomic profiles. Emerg Microbes Infect. 2019; 8: 1043–53.
- Li PKT, Chow KM, Cho Y, Fan S, Figueiredo AE, Harris T, et al. ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment. Perit Dial Int. 2022; 42: 110–53.
- Fung WWS, Chow KM, Li PKT, Szeto CC. Clinical course of peritoneal dialysis-related peritonitis due to non-tuberculous mycobacterium – a single centre experience spanning 20 years. Perit Dial Int. 2022; 42: 204–11.
- Gokani K, Davda P, Dedicoat MJ, Kamesh L, David MD. Peritoneal dialysis associated non-tuberculous mycobacterial peritonitis at a tertiary care hospital in the UK. Clin Infect Pract. 2023; 17: 100213.
- Armstrong DT, Parrish N. Current updates on mycobacterial taxonomy, 2018 to 2019. J Clin Microbiol. 2021; 59: e0152820.
- Lange C, Böttger EC, Cambau E, Griffith DE, Guglielmetti L, van Ingen J, et al. Consensus management recommendations for less common non-tuberculous mycobacterial pulmonary diseases. Lancet Infect Dis. 2022; 22: e178–90.
- Johnson JS, Spakowicz DJ, Hong BY, Petersen LM, Demkowicz P, Chen L, et al. Evaluation of 16S rRNA gene sequencing for species and strain-level microbiome analysis. Nat Commun. 2019; 10: 5029.
- Daley CL, Iaccarino JM, Lange C, Cambau E, Wallace RJ, Andrejak C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: An official ATS/ERS/ESCMID/IDSA clinical practice guideline – executive summary. [Journal details missing – likely Clin Infect Dis].
- Bnaya A, Wiener-Well Y, Soetendorp H, Einbinder Y, Paitan Y, Kunin M, et al. Nontuberculous mycobacteria infections of peritoneal dialysis patients: a multicenter study. Perit Dial Int. 2021; 41: 284–91.
