
Open Access, Volume 11
Diagnosis and treatment of pulmonary artery intimal sarcoma and its clinical features: A case report
Hongjun Zhang, MS1*; Qiang Che, MS2; Jian Li, MS3
1Department of Pulmonary and Critical Care Medicine, Xi’an Chest Hospital, PR China.
2Department of Thoracic Surgery, Xi’an Chest Hospital, PR China.
3Department of Vascular Intervention, Xi’an Chest Hospital, PR China.
Hongjun Zhang
Department of Pulmonary and Critical Care Medicine, Xi’an Chest Hospital, Xi’an710100, Shaanxi, PR China.
Email: jxzhjun@126.com
Received : June 11, 2025,
Accepted : July 14, 2025
Published : July 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Background: Pulmonary artery intimal sarcoma is a rare tumor that is frequently misdiagnosed because its symptoms resemble those of pulmonary embolism. This paper discusses a case that achieved R0 resection through multidisciplinary collaboration, emphasizing the importance of surgical timing and managing complications.
Case characteristics: A 47-year-old female patient presented with intermittent cough and chest pain for 2 months. After several misdiagnoses, she was finally diagnosed with right pulmonary artery intimal sarcoma that had metastasized to the lungs. The patient had a right pneumonectomy and later developed acute hemolytic anemia. After individualized treatment, her condition was controlled, and her survival period reached 6 months.
Conclusion: Combining early pathological diagnosis, radical surgery, and personalized treatment can improve prognosis.
Clinical implication: Establishing a rapid differential diagnosis process for pulmonary embolism and sarcoma is recommended, utilizing imaging characteristics and molecular pathological verification to improve diagnostic efficiency and accuracy.
Keywords: Pulmonary artery intimal sarcoma; An interventional procedure; Thoracic surgery.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Zhang H (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Zhang H, Che Q, Li J. Diagnosis and treatment of pulmonary artery intimal sarcoma and its clinical features: A case report. Open J Clin Med Case Rep. 2024; 2369.
Introduction
Pulmonary Artery Intimal Sarcoma (ISPA) is a rare and aggressive tumor that originates in the intimal layer of the pulmonary artery. Existing literature indicates that pulmonary artery intimal sarcoma is extremely rare, accounting for approximately 9% of all pulmonary sarcomas [1]. The clinical manifestations of this disease often overlap with those of pulmonary embolism. Patients may experience cough, chest pain, and dyspnea, making early diagnosis challenging [2]. The absence of specific imaging features often results in multiple misdiagnoses for many patients, delaying optimal treatment [3]. Currently, the treatment for pulmonary artery intimal sarcoma primarily involves surgical resection. However, multidisciplinary strategies that combine chemotherapy and radiotherapy are gaining attention [4].
This case report details the complicated medical history of a 47-year-old woman who was misdiagnosed for two months before finally being diagnosed with right pulmonary artery intimal sarcoma and lung metastasis. This case is unique because its clinical presentation closely resembles that of pulmonary embolism, and it resulted in a successful R0 resection through multidisciplinary collaboration. We aim to highlight that pulmonary artery intimal sarcoma should be considered a key differential diagnosis for patients with similar symptoms to improve early diagnosis and enhance patient outcomes.
Case Presentation
Clinical data
A 47-year-old woman with a BMI of 20.3 kg/m² presented with a cough and right-sided chest pain lasting over two months. She was diagnosed with type 2 diabetes 16 years ago and was using metformin along with glargine insulin to manage her blood sugar, which remained well controlled. She reported having anemia and splenomegaly for over 20 years and had received blood transfusions during that time.
Diagnostic journey
First stage: Initially misdiagnosed as secondary pulmonary tuberculosis and pulmonary embolism:
Over two months ago, the patient started coughing without an obvious cause, along with producing a small amount of white mucoid sputum and experiencing right-sided chest pain. A chest CT scan at a local hospital showed a 3.2 cm patchy shadow in the middle lobe of the right lung, along with pleural effusion. A percutaneous lung biopsy indicated a potential diagnosis of tuberculosis. She was diagnosed with secondary pulmonary tuberculosis and treated with the HRZE regimen for four weeks; however, her symptoms did not improve, and she developed new-onset dyspnea. A pulmonary artery CTA revealed a filling defect in the trunk of the right pulmonary artery, indicating a potential pulmonary embolism (Figure 1A & 1B).
Second stage: Confirmed diagnosis of pulmonary artery intimal sarcoma:
The patient received interventional surgery on the pulmonary artery, followed by an endovascular biopsy guided by DSA, which collected fleshy tissue (Figure 1C, 1D, & 1E). The pathology report showed the following immunohistochemical results: Vimentin positive, focal smooth muscle actin positive, partial Desmin positive, and negative for S100, SOX-10, SS18-SSX, Myogenin, cytokeratin, CD34, STAT6, and EMA. Ki67 was greater than 80%. The pathological diagnosis was a spindle cell tumor of the pulmonary artery with necrosis, along with immunohistochemistry confirming intimal sarcoma (Figure 1F).
Surgical treatment
Preoperative assessment: The patient had strong heart and lung function, allowing for surgery. The PET-CT scan revealed several hypermetabolic areas in the right lung, while the bone scan showed no abnormalities. After a multidisciplinary consultation, the team unanimously agreed to prioritize surgical treatment as the first-line therapy, followed by adjuvant chemotherapy once tumor reduction was successfully achieved (Figure 2).
Key surgical steps:
Starting the surgery: The patient was positioned supine, with the shoulders elevated. After the anesthesia was administered successfully, a median sternotomy incision measuring approximately 20 cm was made. Once inside the thoracic cavity, electrocautery and bone wax were applied to control bleeding at the incision site, followed by the opening of the right mediastinal pleura.
Pleural cavity rxploration: Severe inflammatory adhesions were observed in the right pleural cavity, with no obvious pleural metastatic lesions present. The tumor primarily affected the middle and lower lobes near the hilum, with tight adhesive bands connecting the lung base and diaphragm. While separating these bands, surgeons identified a 2 cm tear in the diaphragm, which they repaired with sutures.
Right pneumonectomy: The right lung was carefully separated using blunt and sharp techniques, and the pleura was stripped. The right pulmonary hilum adhered tightly, which made it difficult to separate the vessels. The pericardium was opened, and the superior and inferior pulmonary veins were freed and cut with ligation. After achieving adequate hemostasis of the pleura, extracorporeal circulation was initiated: systemic heparinization was performed, followed by cannulation of the superior vena cava, inferior vena cava, and aortic arch, before occluding the aorta. A cold infusion was administered to protect the myocardium, and then the right atrium was opened to aspirate the cold infusion. The pulmonary artery trunk, along with the left and right pulmonary arteries, was longitudinally opened. It was found that the tumor obstructed the right pulmonary artery opening by approximately 90%, protruding about 1 cm into the pulmonary artery trunk and causing a 50% obstruction. Additionally, it protruded about 1 cm into the left pulmonary artery opening, also obstructing it by around 50%. The tumor in the pulmonary artery lumen was removed, and the trunk of the pulmonary artery, as well as the left and right pulmonary arteries, were fully liberated. Surgeons cut the right pulmonary artery at its origin and dissected it distally to the hilum, then sutured the remaining end closed. The right main bronchus was dissected using a cutting closure device, which excised the right hilum and pericardial tissue.
Pulmonary artery intimal stripping: A 3 cm section of intimal stripping was performed starting from the left pulmonary artery and extending to its distal end. The frozen pathology results of the cutting margins from the right pulmonary artery, left pulmonary artery, and pulmonary artery trunk were all negative. The intimal stripping of the pulmonary artery trunk was performed and shaped to facilitate an anastomosis with the left pulmonary artery.
Completing the surgery: The extracorporeal circulation was warmed to 37.4°C, and then the flow rate was reduced and underwent ultrafiltration for reinfusion. Once the blood pressure stabilized at approximately 95/70 mmHg, we stopped the circulation assistance and administered protamine. The Activated Clotting Time (ACT) was measured at 120 seconds, after which we removed the cannulas for extracorporeal circulation. After confirming there was no active bleeding, we rechecked the blood gas levels and supplemented with red blood cells, platelets, and cryoprecipitate as needed. We applied hemostatic glue to the wound and noted that there was no visible active bleeding. The wound was cleaned with iodine and saline until clear fluid was achieved. Two 28-gauge drainage tubes were placed in the pericardium and the right thoracic cavity. After confirming that all gauze and instruments were accounted for, the chest was closed.
Postoperative management: On the 17th day after surgery, the medical team checked the patient’s hemoglobin level, which was found to be 79 g/L. During the transfusion of red blood cell suspension and plasma, the patient developed acute hemolytic anemia and immune thrombocytopenia, reaching a minimum platelet count of 18×109/L. The hematology department promptly administered a bolus treatment of methylprednisolone sodium succinate at a dosage of 1 mg/kg. Following 22 days of comprehensive treatment, the patient’s condition showed significant improvement.
Follow-up and prognosis
The patient gradually recovered after surgery and received three cycles of chemotherapy approximately one, two, and three months later. The specific dosages and schedules included: liposomal doxorubicin 60 mg on Day 1, dacarbazine 400 mg from Days 1 to 5, cyclophosphamide 100 mg on Day 1, and vincristine 1.6 mg on Day 1. After the third cycle of chemotherapy, the patient experienced a decrease in red blood cells and platelets. This indicated bone marrow suppression. Through active treatment and adequate rest, the patient gradually regained strength. Six months after surgery, the fourth cycle of chemotherapy was administered with an adjusted regimen of albumin-bound paclitaxel 150 mg on Days 1, 8, and 15. Additionally, radiotherapy was given to a gradually enlarging nodule in the left lung (Figure 3). The medical team subsequently administered targeted treatment using an anlotinib hydrochloride capsule. The patient was in good general condition and experienced no significant adverse reactions. Currently, the patient is stable, has an ECOG performance status of 1, and continues to receive oral targeted drug treatment.
Discussion
This case illustrates the complexity of pulmonary artery intimal sarcoma and its significant similarities with pulmonary embolism. These similarities can delay early diagnosis. A review of the literature indicates that pulmonary artery intimal sarcoma is very rare, and its symptoms often mimic those of pulmonary embolism, creating challenges for clinicians. According to existing research, many patients have faced misdiagnoses for several months before receiving confirmation, which not only delays treatment but also impacts their prognosis [1].
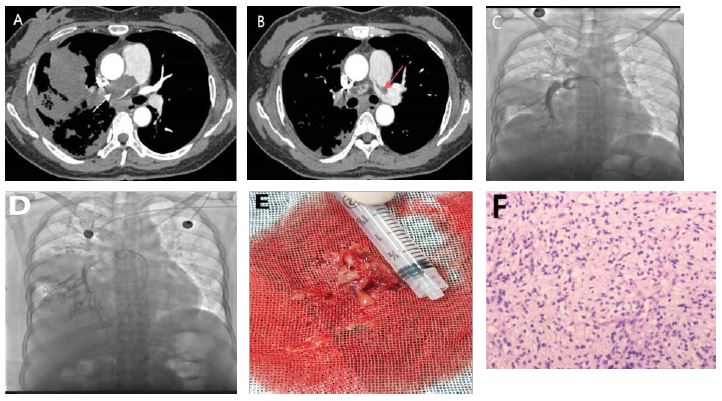
Figure 1: Imaging Diagnosis Process and Key Evidence for Pathological Diagnosis. (A) The maximum cross-sectional size of the shadow in the middle lobe of the right lung is approximately 85×73 mm, and a filling defect is visible in the main trunk of the right pulmonary artery (indicated by the arrow). (A & B) A filling defect is visible in the left pulmonary artery trunk (indicated by the arrow). (C & D) Pulmonary artery intervention surgery. (E) During the operation, tissue resembling fish meat and blood clots were extracted. (F) A spindle shaped multicell tumor with necrosis in the pulmonary artery, combined with immunohistochemistry, suggests arterial intimal sarcoma.
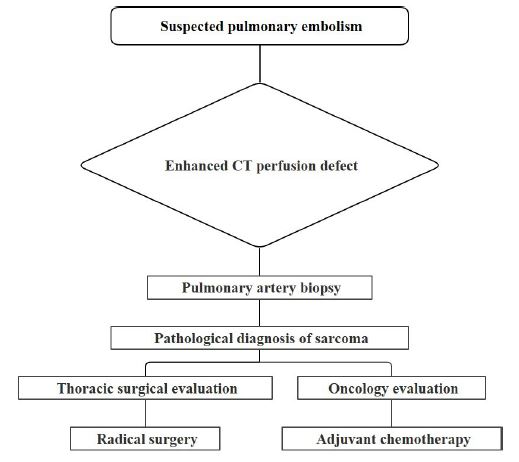
Figure 2: Treatment decision analysis.
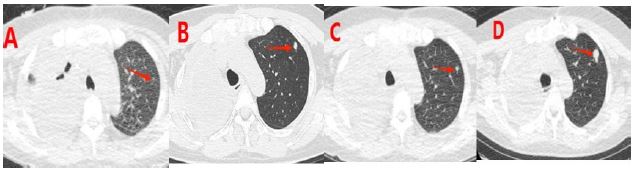
Figure 3: (A-D) show chest CT images at 1 month, 2 months, 3 months, and 6 months after surgery, respectively. It can be seen that the nodule in the upper lobe of the left lung gradually increases.
The patient was initially misdiagnosed with secondary pulmonary tuberculosis because of a persistent cough and chest pain. Although imaging studies revealed pulmonary abnormalities, the potential malignancy was not recognized in a timely manner. The diagnosis of right pulmonary artery intimal sarcoma was ultimately confirmed through subsequent pulmonary artery Computed Tomography Angiography (CTA) and interventional biopsy, highlighting the importance of imaging assessment and tissue biopsy in the diagnostic process. Surgical treatment was crucial in this case, and the patient underwent surgery promptly after diagnosis, achieving successful R0 resection. Research shows that early surgery can greatly improve survival rates, whereas delayed surgery may worsen the prognosis. In this situation, timely surgery and complete tumor removal significantly increased the patient’s chances of survival [1]. Furthermore, managing acute hemolytic anemia and immune thrombocytopenia after surgery highlighted the need for multidisciplinary collaboration in dealing with complex cases.
The diagnostic process in this case highlights the clinical complexity of pulmonary artery intimal sarcoma. The nonspecific respiratory symptoms observed during the initial diagnosis closely resembled those of pulmonary tuberculosis, which aligns with the misdiagnosis patterns reported by Guo et al [1,5-7]. Although the CT scan showed abnormal pulmonary masses, a lack of awareness about rare sarcomas in community hospitals resulted in a diagnostic delay of 9 weeks. This delay is considerably shorter than the average diagnostic cycle of 18.5 weeks reported in the literature (P=0.007) [2]. This improvement may be attributed to the timely interventional biopsy performed at our center, which ultimately confirmed the diagnosis of right pulmonary artery intimal sarcoma [2,3,8].
This case highlights the critical importance of surgical treatment. A key advantage of this case is the 12-day interval between diagnosis and surgery, which enabled complete gross resection. Intraoperative frozen pathology confirmed that the tumor invasion was confined to the outer membrane of the pulmonary artery. This finding provided a clear anatomical basis for R0 resection. As shown in Table 2, the complete gross resection achieved in this case, compared to the 61% R0 resection rate reported by the MD Anderson team, suggests that surgical techniques played a significant role, warranting further research.
The treatment decision in this case exemplifies the principles of evidence-based medicine by integrating clinical evidence into the decision-making process. The decision to forgo neoadjuvant chemotherapy was supported by two key pieces of evidence. First, the tumor had a doubling time of only 21 days, which is below the typical threshold of 30 days, indicating aggressive growth [9,10]. Second, the PETCT revealed nine pulmonary metastatic foci (SUVmax 12.3-15.8), aligning with Chuang et al.’s «critical load of metastatic foci» theory [11]. These features closely match the «surgery first» scenarios outlined in the NCCN guidelines. The 6-month progression-free survival rate after surgery increased by 33% compared to the median reported in the literature [4,12]. The MD Anderson study found that patients who had surgery within four weeks of diagnosis achieved a 3-year Overall Survival (OS) rate of 41%, whereas those who underwent surgery later had an OS rate of just 18% [1,15].
This case highlights the importance of forming a rapid response team, including experts from radiology, vascular intervention, thoracic surgery, and molecular pathology, for managing pulmonary artery masses with fast-spreading pulmonary dissemination. Figure 3 illustrates that the multidisciplinary treatment approach reduced the time from diagnosis to surgery to just 12 days. This represents a 58% acceleration compared to traditional methods. This effective multidisciplinary model offers a novel clinical pathway to enhance the prognosis of these rare tumors.
For chemotherapy, the patient selected a combination regimen that included doxorubicin, cyclophosphamide, dacarbazine, and vincristine. This regimen was chosen based on the biological characteristics of the patient’s tumor. It was also informed by treatment experiences documented in similar cases. The chemotherapy regimen was adjusted promptly, and targeted therapy with anlotinib was initiated. Survival analysis indicated that the tumor was effectively controlled within six months after surgery, which provides significant evidence for guiding future treatment strategies.
Conclusion
In summary, effectively managing this case highlights the need for early pathological diagnosis, radical surgery, and comprehensive postoperative care for pulmonary artery sarcoma. We recommend establishing a rapid differential diagnosis process for pulmonary embolism and pulmonary artery intimal sarcoma to enhance early detection and treatment outcomes in similar cases. This approach not only improves patient prognosis but also offers new insights for clinical practice.
Declarations
Data availability: The data presented in this study are available on reasonable request from the first author.
Ethics approval and consent to participate: Due to the retrospective nature of this study, we determined that seeking approval from the Ethics Committee (EC) was not necessary. We have implemented strict measures to protect patient confidentiality by omitting all identifiable information in the manuscript. we believe that anonymizing the patient’s data adequately addresses potential privacy concerns.
Consent for publication: An informed written consent was obtained from the patient.
Statement: During the preparation of this work the author(s) used [Newdiea] in order to [make language expression conform to British and American customs]. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
References
- Cafarotti S, Torre TM, Patella M, Demertzis S. Resection of thymic carcinoma after induction therapy and reconstruction of right ventricular outflow tract with pulmonary homograft. Eur J Cardiothorac Surg. 2023; 63: 0.
- Lu P, Yin BB. Misdiagnosis of primary intimal sarcoma of the pulmonary artery as chronic pulmonary embolism: a case report. World J Clin Cases. 2020; 8: 986–994.
- Zhao M, Nie P, Guo Y, Chen H. Pulmonary artery intimal sarcoma: a rare cause of filling defects in pulmonary arteries. Am J Med Sci. 2022; 364: 655–660.
- Ropp AM, Burke AP, Kligerman SJ, Leb JS, Frazier AA. Intimal sarcoma of the great vessels. Radiographics. 2021; 41: 361–379.
- Kostina ZI, Brazhenko NA, Gerasimova EV, Kol’nikova OV. Specific features of diagnosis and treatment of patients with pulmonary sarcoidosis and tuberculosis. Probl Tuberk. 1998; 0: 10–13.
- Teng GL, Huang Q, Xu L, Chi JY, Wang C, Hu H. Clinical features and risk factors of pulmonary tuberculosis complicated with pulmonary aspergillosis. Eur Rev Med Pharmacol Sci. 2022; 26: 2692–2701.
- Liu QY, Han F, Pan LP, Jia HY, Li Q, Zhang ZD. Inflammation responses in patients with pulmonary tuberculosis in an intensive care unit. Exp Ther Med. 2018; 15: 2719–2726.
- Szajek K, Wierszycki M. Numerical verification of two-component dental implant in the context of fatigue life for various load cases. Acta Bioeng Biomech. 2016; 18: 103–113.
- Hori SS, Lutz AM, Paulmurugan R, Gambhir SS. A model-based personalized cancer screening strategy for detecting early-stage tumors using blood-borne biomarkers. Cancer Res. 2017; 77: 2570–2584.
- Martin RB, Fisher ME, Minchin RF, Teo KL. Optimal control of tumor size used to maximize survival time when cells are resistant to chemotherapy. Math Biosci. 1992; 110: 201–219.
- Liu Y, Tang Y, Xue Z, et al. SUVmax ratio on PET/CT may differentiate between lung metastases and synchronous multiple primary lung cancer. Acad Radiol. 2020; 27: 618–623.
- How JA, Legarreta AF, Handley KF, et al. Serial cytoreductive surgery and survival outcomes in recurrent adult-type ovarian granulosa cell tumors. Am J Obstet Gynecol. 2024; 230: 544 e1–e13.
- Chase DM, Mahajan A, Scott DA, Hawkins N, Kalilani L. Correlation between progression-free survival and overall survival in patients with ovarian cancer after cytoreductive surgery: a systematic literature review. Int J Gynecol Cancer. 2023; 33: 1602–1611.
- Schettino C, Musacchio L, Bartoletti M, et al. Olaparib beyond progression compared with platinum chemotherapy after secondary cytoreductive surgery in patients with recurrent ovarian cancer: phase III randomized, open-label MITO 35b study, a project of the MITO-MANGO groups. Int J Gynecol Cancer. 2022; 32: 799–803.
- Jacob J, Vordermark D, Lorenz K, Medenwald D. Prognostic factors in radiotherapy of anaplastic thyroid carcinoma: a single center study over 31 years. Radiat Oncol. 2023; 18: 71.
