
Open Access, Volume 11
A spinal tubular lateral approach for a lumbar osteophyte: An illustrative case
Venanzi Maria Sole, MD1,2*; Bruzzo Mattia, MD2
1Neurosurgery Unit, Istituto Giannina Gaslini, Genoa, Italy.
2Spinal Unit, Ospedali Galliera, Genoa, Italy.
Venanzi Maria Sole
Neurosurgery Unit, Istituto Giannina Gaslini, Genoa, Italy.
Email: mariasolevenanzi@gaslini.org
Received : June 10, 2025,
Accepted : July 10, 2025
Published : July 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Background: Osteophytes are common in degenerative joints and are often associated with osteoarthritis. Obesity-induced mechanical stress contributes significantly to vertebral osteophyte formation. While conservative management with non-steroidal anti-inflammatory drugs is the initial standard treatment, surgical intervention is considered based on persistence of symptoms, osteophyte location and orientation.
Observations: In this case-report, the authors present a 72-year-old man with a history right crural neuralgia due the compression of the iliopsoas muscle by a lumbar osteophyte, originating from the zygapophyseal joint (third- fourth lumbar vertebra). A mini-invasive spinal tubular lateral approach (usually used in lateral lumbar interbody fusion, LLIF, to expose the spinal disc) was employed to drill the osteophyte away. There were no complications during and after the operation. After surgery, the patient experienced an immediate pain relief, and subsequent follow-up at 6 weeks indicated sustained pain-free status, with a post-operative lumbar Computed Tomography (CT) after 6 weeks revealing the absence of the osteophyte.
Lessons: This case report demonstrates the effective application of lumbar tubular lateral approach to address a specific pathology outside the spinal disc, such as lumbar osteophytes. The successful outcome was achieved through the patient’s referral to a specialized spinal surgery center and the involvement of a neurosurgeon experienced in LLIF procedures.
Keywords: Osteophytes; Spinal tubular lateral approach; Case report.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Venanzi MS (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Venanzi MS, Mattia B. A spinal tubular lateral approach for a lumbar osteophyte: An illustrative case. Open J Clin Med Case Rep. 2025; 2368.
Introduction
Osteophytes are bone projections that develop along joints, due to abnormal growth of bone or bony spurts. They can impact various degenerative joints, including interphalangeal joints (manifesting as Heberden’s nodes), hips, and knees, and they are usually identified radiologically in the presence of osteoarthritis [1].
While precise data on the frequency of spinal osteophyte formation and age-related changes remain scarce, it is reasonable to infer a similar presentation to osteoarthritis, with an increasing prevalence with age [1]. The main factor contributing to vertebral osteophyte formation is obesity since the increased weight on the vertebral column cause mechanical stress and the subsequent bone formation [1,2]. Notably, excessive mechanical stress during youth predisposes individuals to osteophyte development later in life [3]. Other factors associated with osteophytosis include non-insulin-dependent diabetes mellitus [4], hypervitaminosis A [5,6], and the secretion of bone morphogenetic factor [7].
Clinical manifestations of vertebral osteophytes often arise from the compression of adjacent structures, including nerves, muscles, or vessels.
A conservative approach with non-steroidal anti-inflammatory drug is the standard treatment. If drug therapy proves ineffective, surgical intervention may be considered, with the proposed approach contingent on the orientation of the osteophyte [1]. While anterior surgical approaches have been employed in various studies, particularly at the cervical level [8-10], in this case, a lateral approach was chosen to address the offending osteophyte at the zygapophyseal joint between the third and fourth lumbar vertebra.
Case Presentation
A 72-year-old male patient presented to our institution with a history of right crural neuralgia that had begun a few months prior. At the neurological examination there was no evidence of sensory or motor deficits in the lower limbs, but she experienced significant walking impairment due to intense pain. A spinal lumbar Magnetic Resonance Imaging, MRI, (Figure 1A) revealed the presence of a right lumbar osteophyte at the zygapophyseal joint between the third and fourth lumbar vertebra, resulting in impingement of the ipsilateral psoas muscle. A lumbar CT scan was not performed before the surgery.
Needle electromyography did not indicate any nerve involvement.
Despite a two-month course of non-steroidal anti-inflammatory drugs, the patient experienced only modest clinical improvement, with persistent nighttime pain and continued functional impairment. Therefore, a surgical intervention to smooth the osteophyte was proposed and a spinal tubular lateral approach was performed.
Under general anesthesia, during the surgical procedure, the patient was placed lateral position, perpendicular to the floor, with patient’s iliac crest at the break in the bed and the X-ray kept at 0-90 degrees.
Both hips were flexed to relax psoas muscle and knees bent to prevent leg falling. Three grips were utilized to immobilize the patient: two posteriorly (one at the mid-shoulder level and the other at buttock level) and one anteriorly to secure the thorax (Figure 2A & B).
Once the optimal position was achieved, the patient was securely taped to the bed. Then, the bed was broken 50% of the maximum allowed and checked lateral x-ray, adjusting Trendelenburg position to ensure the lumbar disc perpendicular to the floor and the lateral x-ray parallel to the disc space (Figure 1).
Using X-ray guidance, the point on the skin directly overlying the osteophyte was identified. An incision was made through the skin, fat, and subcutaneous tissue. Retractors were placed, and the fascia of the external oblique muscle was opened with a scalpel, followed by atraumatic splitting of the muscle using fingers.
The transversalis fascia and its muscle were then encountered and opened. In the depth of the muscle, the lumbar osteophyte exposed and identified with the assistance of X-ray. The expansion channel was placed, after confirming that there were no blood vessels or nerve structures in the lateral side of the intervertebral space.
The bony spur was carefully drilled away, and an X-ray was performed to confirm the complete removal of the osteophyte (Figure 3B & C).
The patient was discharged at home on the second day after the operation. He reported complete relief of pain immediately after the procedure, and at the 6-week follow-up, he was still pain-free. A lumbar computed tomography revealing the absence of the osteophyte was performed 6 weeks after the operation (Figure 4A).
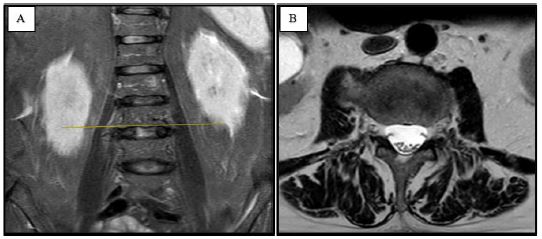
Figure 1: Lumbar MRI displaying the right osteophyte the third and fourth lumbar vertebra: coronal (A) and axial planes (B).
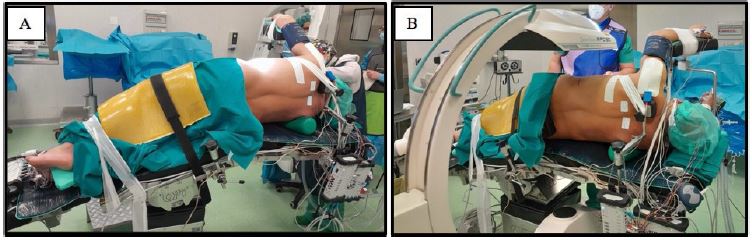
Figure 2: Patient’s and X-ray positioning in the operative room.
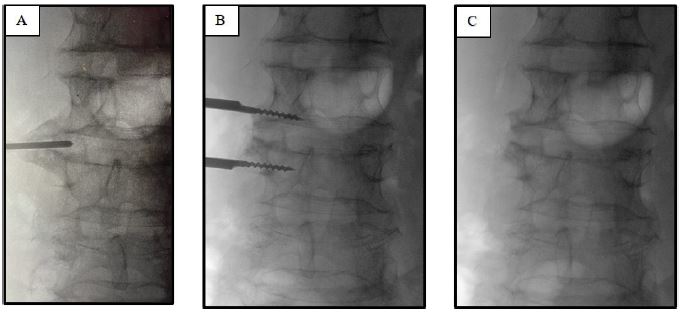
Figure 3: Lumbar X-ray imaging displaying lumbar tract before (A) and after the osteophyte’s drilling (B,C).
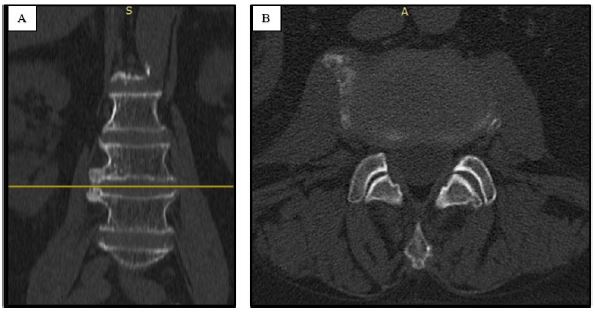
Figure 4: The follow-up lumbar computed tomography, 6 weeks after the operation revealing the absence of the osteophyte: coronal (A) and axial planes (B).
Discussion
Osteophyte formation on spinal vertebral bodies is one of the degenerative changes typical of osteoarthritis. The onset of osteophyte pathogenesis begins with the degeneration of the nucleus pulposus, characterized by water loss and a reduction in height. This process leads to diminished resilience of the intervertebral disc under load, accompanied by a loss of elasticity in the annulus fibrosus. Consequently, to optimize weight-bearing surface area, bony projections emerge from the borders of the zygapophyseal joints [11]. Pye et al, indeed, observed a correlation between the increasing severity of osteophyte formation and the concurrent narrowing of vertebral disc spaces. This observation implies a potential association between the worsening changes seen in osteoarthritis and the degree of osteophyte severity [12].
The formation of vertebral osteophytes is attributed to established etiological factors such as obesity and non-insulin dependent diabetes mellitus. Mitigating these factors may confer a preventive effect against osteophyte formation [1].
In the context of lumbar osteophytes, Cvijetic et al. reported a prevalence of 21.3% in men and 23.9% in women over 45 years old [13]. Lumbar osteophytes are predominantly found in the order of L4, L5, L1, L2, and L3, with a majority located on the superior (39.7%) and inferior surfaces (38.4%) of the body and 22% at the level of the articular facet (as in our case). They typically originate from the anterior side of the superior surface of the body (30.4%) and the lateral side of the inferior surface (26.2%) [14].
Lumbar osteophytes may impact in local structures, leading to scenarios such as lumbar algia and nerve root compression. As Matsumoto et al. described, in the majority of cases of L5 nerve’s compression in the lumbosacral tunnel (composed by the fifth lumbar vertebral body, the lumbosacral ligament and the sacral ala), osteophytes are detected [15]. Chaabane et al. previously reported a case of a 58-year-old man with an osteophyte in the right sacroiliac joint causing conflict with the crural nerve, resulting in back pain and slight motor deficiency of the right leg [16].
Radiologic imaging and electrophysiological studies, such as electromyography, can detect nerve involvement. Lumbar MRI and CT scans may also aid in distinguishing osteophytes from other pathologies causing similar symptoms, such as lumbar disc herniation. These bony spurs, due to their proximity to major abdominal vessels, can potentially lead to cardiovascular complications, including vena cava [17,18].
While Di Lorenzo et al. previously detailed a case of psoas impingement syndrome in severe hip osteoarthritis [19], and LaBan et al. reported compression of the iliopsoas muscle by a lumbar osteophyte in one patient [20], this is the first time that the spinal tubular lateral approach has been proposed to remove a lumbar osteophyte.
Traditionally, the initial treatment entails a conservative approach utilizing non-steroidal anti-inflammatory drugs to minimize the inflammatory reaction associated with osteophyte formation. In cases where this approach proves ineffective, surgical intervention may be pursued to address the osteophyte. The resolution of symptoms following osteophyte removal was evident in our case, aligning with existing literature [1].
The anterior surgical approach is the most proposed and primarily used for the cervical tract, noteworthy cases, such as that reported by Calisaneller et al, have highlighted the efficacy of this strategy. They presented a patient with diffuse idiopathic skeletal hyperostosis with osteophytic spurs spanning from C2 to C6, resulting in worsening dysphagia: the vertebrae were smoothed by using a high-speed drill [21].
For cases involving the C1-C2 region, a peri-oral transpharyngeal approach may be considered [22].
Additionally, interbody fusion emerges as a viable option, particularly when load-bearing vertebrae, such as C5-C6 or L1-L2, are affected, preventing post-surgical osteophyte’s recurrence. We refrained from immediate interbody fusion, keeping it as a potential future strategy in case of recurrence.
In order to mitigate vascular and visceral risks associated with the anterior approach and minimize blood loss inherent to an open posterior approach, we embraced a less-invasive alternative employing a lateral approach. This approach draws inspiration from the extreme Lateral Interbody Fusion (XLIF) technique but differs in execution, since last operative steps of discectomy and arthrodesis by positioning a cage were not performed. A minimal invasive muscle-splitting approach enables rapid postoperative mobilization. However, this approach carries the risk of lumbar plexus, psoas muscle, and bowel injury, particularly at the L4/5 level. Additionally, the management of vascular injury, if encountered, can be challenging [23].
The clinical and radiological success of this minimally invasive technique was made possible by the patient’s consultation at a specialized spine center, coupled with the extensive experience of the spine surgeon in performing XLIF procedures.
Conclusion
This case-report display how a surgical approach, usually used in spinal surgery, such as a lumbar tubular lateral approach (used particularly in XLIF to expose the lumbar disc), may be used for other spinal pathology, such as osteophytes, not necessarily involving spinal disc.
The excellent clinical and radiological result was possible since the patient was referred to a spinal surgery center with an XLIF- experienced neurosurgeon. Indeed, the choice of this type of operation, instead of other much less invasive and with greater complications, was weighted after meticulous intraoperative observations and the ability of the spinal surgeon to reinvent the surgical gesture.
References
- Klaassen Z, Tubbs RS, Apaydin N, Hage R, Jordan R, Loukas M. Vertebral spinal osteophytes. Anat Sci Int. 2011; 86: 1–9.
- Lindsey T, Dydyk AM. Spinal osteoarthritis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024.
- Venne G, Tse MY, Pang SC, Ellis RE. Mechanically-induced osteophyte in the rat knee. Osteoarthritis Cartilage. 2020; 28: 853–864.
- Littlejohn GO. Insulin and new bone formation in diffuse idiopathic skeletal hyperostosis. Clin Rheumatol. 1985; 4: 294–300.
- Seawright AA, English PB, Gartner RJ. Hypervitaminosis A and hyperostosis of the cat. Nature. 1965; 206: 1171–2.
- Yee C, Wong HY, Fewer HD, Rogers AG. Two cases of dysphagia due to cervical spine osteophytes successfully treated surgically. Can Med Assoc J. 1985; 132: 810–2.
- Hanamura H, Higuchi Y, Nakagawa M, Iwata H, Nogami H, Urist MR. Solubilized bone morphogenetic protein (BMP) from mouse osteosarcoma and rat demineralized bone matrix. Clin Orthop Relat Res. 1980; 148: 281–90.
- Brandenberg G, Leibrock LG. Dysphagia and dysphonia secondary to anterior cervical osteophytes. Neurosurgery. 1986; 18: 90–3.
- Calisaneller T, Ozdemir O, Tosun E, Altinors N. Dysphagia due to diffuse idiopathic skeletal hyperostosis. Acta Neurochir (Wien). 2005; 147: 1203–6.
- Hasegawa H, Bitoh S, Ohtsuki H, Obashi J, Furukawa H, Yamamoto T. A case of Forestier’s disease causing dysphagia. No Shinkei Geka. 1984; 12: 1379–83. Japanese.
- Oichi T, Taniguchi Y, Oshima Y, Tanaka S, Saito T. Pathomechanism of intervertebral disc degeneration. JOR Spine. 2020; 3: e1076.
- Pye SR, Reid DM, Lunt M, Adams JE, Silman AJ, O’Neill TW. Lumbar disc degeneration: association between osteophytes, end-plate sclerosis and disc space narrowing. Ann Rheum Dis. 2007; 66: 330–3.
- Cvijetić S, McCloskey E, Korsić M. Vertebral osteophytosis and vertebral deformities in an elderly population sample. Wien Klin Wochenschr. 2000; 112: 407–12.
- Chanapa P, Yoshiyuki T, Mahakkanukrauh P. Distribution and length of osteophytes in the lumbar vertebrae and risk of rupture of abdominal aortic aneurysms: a study of dry bones from Chiang Mai, Thailand. Anat Cell Biol. 2014; 47: 157–61.
- Matsumoto M, Chiba K, Nojiri K, Ishikawa M, Toyama Y, Nishikawa Y. Extraforaminal entrapment of the fifth lumbar spinal nerve by osteophytes of the lumbosacral spine: anatomic study and a report of four cases. Spine (Phila Pa 1976). 2002; 27: E169–73.
- Chaabane M, Abid R, Hamza K, Aloulou R, Robbana A, Chaabouni L, Hamza R. Etiologie inhabituelle de cruralgie. J Radiol. 1994; 75: 283–5. French.
- León JA, Calamia KT, Leventhal JP. Chronic obstructive pneumonia caused by a vertebral body osteophyte. Mayo Clin Proc. 2000; 75: 185–8.
- Scapinelli R. Compression of the inferior vena cava due to diffuse idiopathic skeletal hyperostosis. Rev Rhum Engl Ed. 1997; 64: 198–201.
- Di Lorenzo L, Jennifer Y, Pappagallo M. Psoas impingement syndrome in hip osteoarthritis. Joint Bone Spine. 2009; 76: 98–100.
- LaBan MM, Jones M, Lenger A. Mechanical compression of the iliopsoas muscle by a large vertebral osteophyte, presenting with abdominal and lumbar pain. Am J Phys Med Rehabil. 2015; 94: e75.
- Calisaneller T, Ozdemir O, Tosun E, Altinors N. Dysphagia due to diffuse idiopathic skeletal hyperostosis. Acta Neurochir (Wien). 2005; 147: 1203–6.
- Snodgrass JJ. Sex differences and aging of the vertebral column. J Forensic Sci. 2004; 49: 458–63.
- Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg. 2015; 1: 2–18.
