
Open Access, Volume 11
The stethoscope’s secret: How auscultation helps identify the subtle signs of bronchial carcinoid tumors
Kartik Sood, MD1*; Manal Sayed Rezzek El Sayed2
1Pulmonologist, Hatta Hospital, Dubai Health, UAE.
2Head of Specialized Internal Medicine Department, Hatta Hospital, Dubai Health, UAE.
Kartik Sood
Pulmonologist, Hatta Hospital, Dubai Health, UAE.
Email: drkartiksood@gmail.com
Received : June 05, 2025,
Accepted : July 07, 2025
Published : July 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Bronchial carcinoid tumors, although rare, can present subtly and often masquerade as more common pulmonary conditions. This case highlights how vigilant clinical auscultation played a pivotal role in diagnosing a bronchial carcinoid tumor in a 50-year-old male presenting with persistent cough and intermittent wheezing. Initial investigations were inconclusive, but meticulous physical examination led to targeted imaging and subsequent diagnosis via bronchoscopy and biopsy.
Keywords: Bronchial carcinoid; Auscultation; Wheeze; Pulmonary nodule; CT scan; Bronchoscopy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Sood K (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Sood K, EI Sayed MSR. The stethoscope’s secret: How auscultation helps identify the subtle signs of bronchial carcinoid tumors. Open J Clin Med Case Rep. 2025; 2367.
Introduction
Bronchial carcinoid tumors represent a subset of neuroendocrine tumors that originate in the lungs. They account for less than 5% of all pulmonary neoplasms and often present in younger adults. These tumors can be challenging to diagnose, particularly when their presentation mimics benign conditions such as asthma or bronchitis. This case report underlines the significance of careful clinical auscultation in guiding early diagnostic work-up.
Case Presentation
A 42-year-old male presented to our outpatient clinic with a 2-month history of persistent dry cough, mild exertional dyspnea, and occasional wheezing. He was a non-smoker with past history of Bronchial Asthma which was diagnosed 3 years back and patient was on Inhaled salbutamol on as needed basis. Clinical auscultation revealed a localized wheeze over the right lower lobe. Chest X-ray showed a suspicious opacity. CT chest revealed a well-defined lesion at the origin of the right lower lobe bronchus. Bronchoscopy visualized an endobronchial mass, and biopsy confirmed a typical carcinoid tumor.
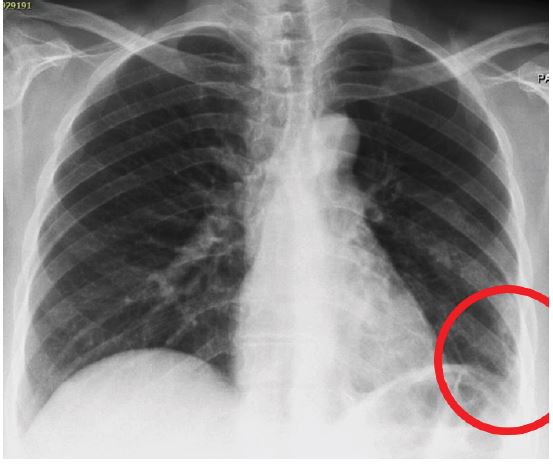
Figure 1: Chest X-ray showing an opacity in the right lower lobe.
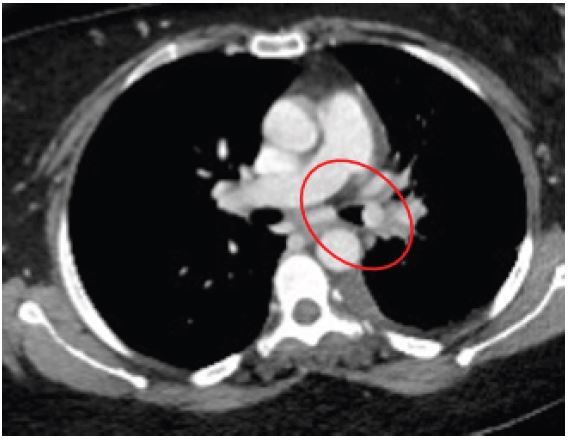
Figure 2: CT axial image showing endobronchial lesion.
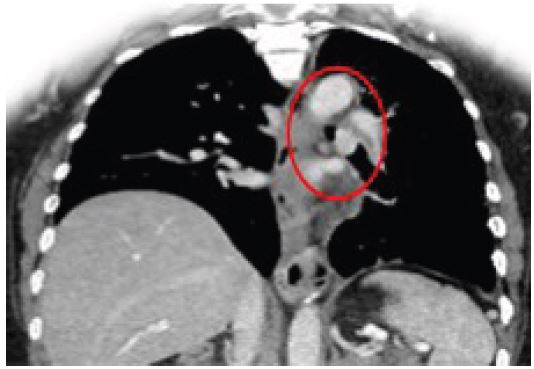
Figure 3: CT coronal image showing tumor obstructing the right lower lobe bronchus.

Figure 4: Left main bronchus was 90% occluded by endobronchial mass -see by bronchoscopy.
Discussion
Bronchial carcinoids are rare but important differential diagnoses in patients with unexplained cough and localized wheezing. Physical examination can provide critical clues, particularly when imaging findings are subtle. In this case, early auscultation findings guided further workup. Bronchoscopy remains essential for visual confirmation and biopsy. Typical carcinoids have an excellent prognosis if diagnosed early and resected completely.
In the diagnosis of bronchial carcinoid tumors, immunohistochemical markers play a crucial role. Markers such as chromogranin A, synaptophysin, and Ki-67 are commonly used in biopsy samples to confirm the neuroendocrine nature of the tumor. Chromogranin A and synaptophysin are markers of neuroendocrine differentiation, while Ki-67 is a proliferation marker that helps in assessing the tumor’s growth rate. A low Ki-67 index is typically associated with typical carcinoids, whereas a higher Ki-67 index may indicate atypical carcinoids or other high-grade neuroendocrine tumors [1-5].
Conclusion
This case underscores the importance of thorough clinical examination. A vigilant auscultation detected localized wheeze, which prompted targeted imaging and bronchoscopy. Early diagnosis led to timely surgical intervention and improved prognosis.
Declarations
Patient consent: Written informed consent was obtained from the patient for the publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Conflict of interest: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethical approval: This case report was conducted in accordance with ethical standards and institutional guidelines. Approval from the ethics committee was not required as the report describes a single anonymized patient case with informed consent.
References
- Caplin ME, Baudin E, Ferolla P, et al. Pulmonary neuroendocrine (carcinoid) tumors: European Neuroendocrine Tumor Society expert consensus and recommendations for best practice. Ann Oncol. 2015.
- Gustafsson BI, Kidd M, Chan A, Malfertheiner MV, Modlin IM. Bronchopulmonary neuroendocrine tumors. Cancer. 2008.
- Caplin ME, Baudin E, Ferolla P, et al. Pulmonary neuroendocrine (carcinoid) tumors: European Neuroendocrine Tumor Society (ENETS) guidelines for diagnosis and treatment. Neuroendocrinology. 2015; 103: 108–118.
- Skuladottir H, Hirsch FR, Hansen HH. Pulmonary neuroendocrine tumors: incidence and prognosis of histological subtypes. A population-based study in Denmark. Lung Cancer. 2002;37(2):127–135.
- Beasley MB, Thunnissen FB, Brambilla E, et al. Pulmonary atypical carcinoid: predictors of survival in 106 cases. Hum Pathol. 2000; 31: 1255–1265.
