
Open Access, Volume 11
Twelve years of unexpected bleeds: Hemoperitoneum as a rare twist in rare bleeding disorders
Somdipa Pal*; Dhruti Manish Pandya; Jyothi Munireddy; Siddharth Totadri; Vandana Bharadwaj; Anand Prakash
Department of Pediatric Hematology Oncology, St. John’s Medical College and Hospital, India.
Somdipa Pal
Department of Pediatric Hematology Oncology, Johns Medical College and Hospital, Bangalore-560034, Karnataka, India.
Tel: +918373970796; Email: drsomdipa@gmail.com
Received : May 21, 2025,
Accepted : June 27, 2025
Published : June 30, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Massive hemoperitoneum is rare and associated with underlying systemic or local pathology. We report 8 episodes of hemoperitoneum in 7 children with rare bleeding disorders who presented with acute abdominal pain. The diagnosis was by imaging, and all responded with conservative treatment. Hemorrhagic corpus luteal cyst was the most common etiology in adolescent girls. Oral Contraceptive Pill (OCP) prophylaxis was used to prevent recurrence. Optimal management can be attained by a high index of suspicion, careful clinical assessment, multidisciplinary treatment, close follow-up, and prophylaxis when feasible, to prevent recurrences.
Keywords: Hemoperitoneum; Rare bleeding disorder; Adolescent; Oral contraceptive pill.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Pal S (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Pal S, Pandya DM, Munireddy J, Totadri S, Bharadwaj V, Prakash A. Twelve years of unexpected bleeds: Hemoperitoneum as a rare twist in rare bleeding disorders. Open J Clin Med Case Rep. 2025; 2366.
Introduction
Rare Bleeding Disorders (RBDs) are defined as the congenital deficiency of fibrinogen (Factor I), Factor II, Factor V, Factor VII, Factor X, Factor XI, and Factor XIII. These are autosomal recessive inheritance, with a 3-5% prevalence of all coagulation factor deficiency [1]. The incidence is higher in areas with high consanguinity rates, like southern India [2]. Hemoperitoneum or intraperitoneal bleeding is an uncommon presentation in children with bleeding disorders and extremely rare in RBDs. Only a few case reports of hemoperitoneum in RBDs [3-12]. We share our experience of children with RBDs who presented with hemoperitoneum.
The Institutional Ethics Committee (IEC number: IEC/357/2024) approved the protocol with a waiver of informed consent.
Clinical cases
We retrospectively reviewed data for all children less than 18 years of age with bleeding disorders diagnosed at our institute from January 2012 to July 2024. The salient features of the children with hemoperitoneum along with RBDs are detailed below.
Table 1 describes the clinical characteristics, management approach, and outcomes.
Case 1
A 9-year-old boy with afibrinogenemia (diagnosed previously due to intracranial bleeding following minor trauma) was brought to the emergency room with complaints of an acute onset of pain in the abdomen. There was no history of fever, changes in stool color or consistency, burning micturition, vomiting, or any trauma. An urgent ultrasound of the abdomen confirmed the diagnosis of hemoperitoneum. CT abdomen also confirmed the same diagnosis with no evidence of bleeding vessels. He was treated with packed red blood cells and cryoprecipitate transfusion. He was discharged and continues on prophylaxis with cryoprecipitate because of recurrent major bleeding episodes.
Cases 2,3,4,5,7
All these children were adolescent girls between 14 to 17 years of age who presented with complaints of acute onset of pain over the abdomen (Table 1). They all had ongoing menorrhagia. These children were already diagnosed with different RBDs (2 children had F XIII deficiency, one child each F I, F VII, and F X deficiency), given previous bleeding episodes. Diagnosis of hemoperitoneum was confirmed by Ultrasound (USG) or CT abdomen. All children had hemorrhagic corpus luteal cysts detected by USG. Acute episodes were managed with packed red blood cells and cryoprecipitate or FFP transfusion. One child had a 2nd episode of severe hemoperitoneum requiring injectable Factor VII replacement. Children with afibrinogenemia were recommended cryoprecipitate prophylaxis, and the rest of the children were kept on Oral Contraceptive Pill (OCP) prophylaxis to control menorrhagia.
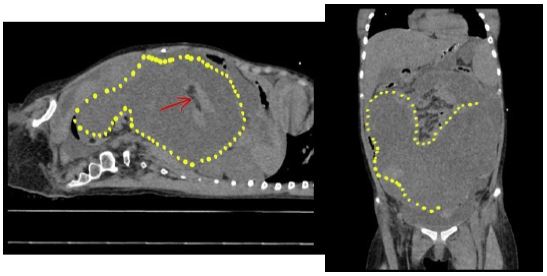
Figure 1: CT scan of the abdomen, demarcated lines showing hemoperitoneum.
Table 1: Details of cases.
| Patient details | Case 1 | Case 2 | Case 3 (2 episodes) | Case 4 | Case 5 | Case 6 | Case 7 |
|---|---|---|---|---|---|---|---|
| Age & Sex | 9 years/M | 16 years/F | 14years/ F | 13years/ F | 13years/ F | 17 years/M | 17years/ F |
| Diagnosis | Afibrinogenemia | Afibrinogenemia | Factor VII deficiency | Factor X deficiency | Factor XIII deficiency | Afibrinogenemia | Factor XIII deficiency |
| Another life-threatening bleed | Intracranial bleed | No | Intracranial bleed | No | No | No | No |
| Etiology | Spontaneous | Haemorrhagic luteal cyst | Haemorrhagic lutealcyst | Haemorrhagic luteal cyst | Haemorrhagic luteal cyst | Trivial trauma, Spleniclaceration | Haemorrhagic luteal cyst |
| Treatment | Cryoprecipitate & PRBCtransfusion | Cryoprecipitate and PRBCtransfusion | FFP, PRBCtransfusion, Factor VII replacement | FFP, PRBCtransfusion | Cryoprecipitate and PRBCtransfusion | Cryoprecipitate and PRBCtransfusion | Cryoprecipitate andPRBC transfusion |
| Prophylaxis | Monthly Cryoprecipitate | Monthly Cryoprecipitate | OCP and FFP | OCP | OCP | Regularfollow- up | OCP |
Case 6
A 17-year-old boy, previously diagnosed with afibrinogenemia, was brought in with complaints of acute pain in the left upper abdomen after a trivial trauma while playing. He was hypotensive and required intensive care. USG was done on suspicion of hematoma and showed splenic laceration injury, which was managed conservatively with packed red cells, cryoprecipitate transfusion, and tranexamic acid in consultation with pediatric surgery.
Discussion
The Prevalence of rare inherited bleeding disorders in the general population is 1-2 per million [12]. According to the RBD database, FXI (37%) and FVII (23%) deficiencies are the most prevalent RBDs worldwide, followed by FI (10%), FV (10%), FX (9%), FXIII (6%) deficiencies [13]. According to a study of North India, FX (1.8%) was found to be the most common RBD [14]. There is very little data on RBDs from South India. We had 91 children with RBDs diagnosed at our institute over 12 years. Factor XIII (33%) and Factor I deficiency (32%) were the predominant etiologies of RBD in our series. Other RBDs that we encountered were F VII-8, F X-7, F V-5, F XI-3, F II-1, and F XII-1.
Most RBDs do not have well-established treatment strategies. While superficial skin and muscle bleeds may be easily detected and controlled with compression, diagnosis of hemoperitoneum requires a high index of suspicion and prompt intervention for optimal outcomes. The prevalence of hemoperitoneum with an underlying bleeding disorder is very rare [15], as well as life-threatening.
In our cohort, the most common bleeding disorder leading to hemoperitoneum was afibrinogenemia, followed by FXIII deficiency. There is no data to compare the spectrum of bleeding manifestations in RBDs. All our patients showed improvement with conservative management. While no definitive treatment guidelines exist for these rare scenarios, surgery can often be avoided with close monitoring and early initiation of supportive care.
In our cohort of hemoperitoneum, the majority (71%) were adolescent girls with menorrhagia. All teenage girls had proven ruptured corpus luteal cysts as per imaging. Studies have demonstrated that female patients of reproductive age, with inherited bleeding disorders, have twice the incidence of hemorrhagic ovarian cysts in comparison to the general population [2,3,8,9], but prompt diagnosis and treatment can give a good outcome.
These cysts rupture during ovulation due to excessive bleeding, leading to hemoperitoneum. Each menstrual cycle increases the possibility of hemoperitoneum in adolescent girls with bleeding disorders. Similarly, one child in our cohort had recurrent episodes of menorrhagia and hemoperitoneum. Prophylaxis is important to prevent recurrent episodes. Hormonal Oral Contraceptives (OCPs) decrease menorrhagia by inhibiting ovulation and ovulation-triggered bleeding [5,6,10]. We started OCP prophylaxis in 4 out of 5 adolescent girls, and they responded with decreased episodes of menorrhagia and no recurrence of hemoperitoneum. This approach allowed avoidance of the use of blood products with their inherent risks (allergic reactions and risk of transmitting infectious agents). Combined OCPs are also known to increase the risk of thrombosis as well in 3-4% of cases [11]. None of our children developed any complications, although longer follow-up is required. Fibrinogen concentrate and factor XIII concentrate could not be used for prophylaxis due to high cost and poor availability.
Our case series is limited by retrospective data collection and a small sample size. We also could not do long-term follow-ups to look for recurrences and to prove that OCPs are practical, safe, and cost-effective prophylaxis for hemoperitoneum.
Conclusion
This study presents one of the largest case series of hemoperitoneum in children with rare bleeding disorders. Among adolescent girls, an exaggerated Mittelschmerz sign emerged as the most common cause, though spontaneous and post-traumatic hemoperitoneum should also be considered. A high index of suspicion is essential when evaluating children with bleeding disorders who present with an acute abdomen. The mainstay of treatment includes factor replacement therapy, transfusion support, and tranexamic acid, while oral contraceptive pills are highly effective in preventing recurrence.
Acknowledgement: I would like to express my sincere gratitude to all those who have supported me in the completion of this paper. I am deeply thankful to all the authors for their invaluable guidance, constant encouragement, and insightful feedback throughout this work.
My appreciation extends to the institute for providing the resources and support necessary for carrying out this research.
Finally, I am grateful to my family and friends for their unwavering support and understanding throughout the process.
References
- James P, Salomon O, Mikovic D, Peyvandi F. Rare bleeding disorders - bleeding assessment tools, laboratory aspects, and phenotype and therapy of FXI deficiency. Haemophilia. 2014; 20: 71–5.
- Mannucci PM, Duga S, Peyvandi F. Recessively inherited coagulation disorders. Blood. 2004; 104: 1243–52.
- Ramadan M, Kharroubi M, Khaza’al J. Successful conservative treatment of ovulation-related hemoperitoneum in a patient with congenital hypofibrinogenemia: a case report and review of literature. J Clin Gynecol Obstet (North Am). 2020; 9.
- Cetinkaya SE, Pabuccu EG, Ozmen B, Dokmeci F. Recurrent massive hemoperitoneum due to ovulation as a clinical sign in congenital afibrinogenemia. Acta Obstet Gynecol Scand. 2011; 90: 192–4.
- Schneider D, Bukovsky I, Kaufman S, Sadovsky G, Caspi E. Severe ovarian hemorrhage in congenital afibrinogenemia. Acta Obstet Gynecol Scand. 1981; 60: 431.
- Bottini E, Pareti FI, Mari D, Mannucci PM, Muggiasca ML, Conti M. Prevention of hemoperitoneum during ovulation by oral contraceptives in women with type III von Willebrand disease and afibrinogenemia: case reports. Haematologica. 1991; 76: 431–3.
- Castaman G, Ruggeri M, Rodeghiero F. Congenital afibrinogenemia: successful prevention of recurrent hemoperitoneum during ovulation by oral contraceptive. Am J Hematol. 1995; 49: 363–4.
- Henselmans JM, Meijer K, Haaxma R, Hew J, van der Meer J. Recurrent spontaneous intracerebral hemorrhage in a congenitally afibrinogenemic patient: diagnostic pitfalls and therapeutic options. Stroke. 1999; 30: 2479–82.
- Koussi A, Economou M, Athanasiou-Metaxa M. Intra-abdominal hemorrhage due to a ruptured corpus luteum cyst in a girl with congenital afibrinogenemia. Eur J Pediatr. 2001; 160: 196.
- Ozdemir O, Sari ME, Kurt A, Sen E, Atalay CR. Recurrent massive haemoperitoneum associated with ruptured corpus luteum in women with congenital afibrinogenemia: case report. Turk J Obstet Gynecol. 2014; 11: 242–5.
- Kim JH, Jeong SY, Cho DH. Massive hemoperitoneum due to a ruptured corpus luteum cyst in a patient with congenital hypofibrinogenemia. Obstet Gynecol Sci. 2015; 58: 427–30.
- Tshering S, Dorji N, Pradhan B. Ovulation triggered hemoperitoneum in inherited Factor VII deficiency. Open J Clin Med Case Rep. 2021; 7: 1721.
- Peyvandi F, Spreafico M. National and international registries of rare bleeding disorders. Blood Transfus. 2008; 6: s45–8.
- Gupta M, Bhattacharyya M, Choudhry VP, Saxena R. Spectrum of inherited bleeding disorders in Indians. Clin Appl Thromb Hemost. 2005; 11: 325–30.
- Acharya SS, et al. Rare Bleeding Disorder Registry: deficiencies of factors II, V, VII, X, XIII, fibrinogen and dysfibrinogenemias. J Thromb Haemost. 2004; 2: 248–56.
