
Open Access, Volume 11
Pulmonary edema after appendicectomy: A postoperative complication
Chiara Cafora; Rossella Esposito; Ivana Maruzzella; Concetta Pellegrini; Fabiana Maurelli; Giovanni Liguori; Fabrizio Gritti; Emilia Capasso; Paolo Francesco Marsilia; Francesco Imperatore*
ICU “A. Cardarelli” Hospital, Naples, Italy.
Francesco Imperatore
ICU “A. Cardarelli” Hospital, Naples, Italy.
Email: francesco.imperatore@aocardarelli.it
Received : May 29, 2025,
Accepted : June 19, 2025
Published : June 30, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Negative Pressure Pulmonary Edema (NPPE) is a rare but potentially life-threatening postoperative complication, with an estimated incidence of 0.05%–0.1% [1]. We report the case of a healthy 19-year-old male who developed acute respiratory distress and hemoptysis immediately following extubation after an uncomplicated laparoscopic appendicectomy. Computed tomography revealed bilateral pulmonary edema. He was successfully managed with oxygen therapy, bronchodilators, and diuretics, with complete resolution of symptoms within 72 hours. This case underscores the importance of early recognition of NPPE and the need to carefully balance diuretic use to avoid hypovolemia.
Keywords: Negative pressure pulmonary edema; General anesthesia; Laparoscopic appendicectomy; Postoperative complication; Respiratory failure.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Imperatore F (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Cafora C, Esposito R, Maruzzella I, Pellegrini C, Maurell F, Liguori G, Imperatore F, et al. Pulmonary edema after appendicectomy: A postoperative complication. Open J Clin Med Case Rep. 2025; 2363.
Introduction
Negative Pressure Pulmonary Edema (NPPE) is a non-cardiogenic pulmonary edema caused by a marked inspiratory effort against an obstructed upper airway, typically due to post-extubation laryngospasm [1,2]. Although uncommon, it is more frequently seen in healthy, young patients capable of generating significant negative intrathoracic pressure [3,4]. NPPE is a diagnosis of exclusion, based on clinical findings, imaging, and response to supportive therapy [5]. This report presents a postoperative case of NPPE and reviews the underlying pathophysiology, diagnostic approach, and management strategies.
Case Report
A 19-year-old male (BMI 22 kg/m², ASA I) presented for elective laparoscopic appendicectomy. The procedure was performed under general anesthesia using propofol, rocuronium, and sevoflurane. Intubation with a 7.0 mm endotracheal tube and intraoperative course were uneventful (Figure 1).

Figure 1: Chest CT with IV contrast before surgery.
Upon emergence and extubation, the patient reported a sensation of “a lump in the throat,” followed by persistent coughing, hemoptysis, and oxygen desaturation (SpO2 82% on room air). Physical examination revealed tachypnea, use of accessory muscles, and diffuse wheezing. Initial chest radiography showed bilateral alveolar infiltrates. A contrast-enhanced chest CT scan (Figure 2) confirmed diffuse pulmonary edema without pleural effusion or cardiomegaly.
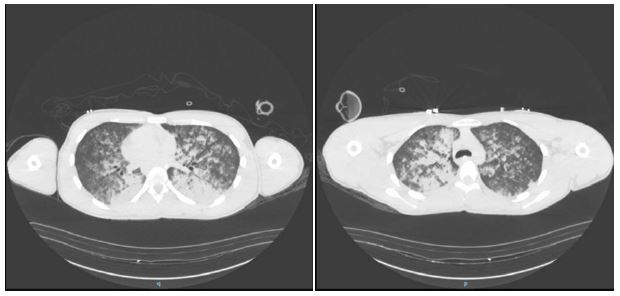
Figure 2: Chest CT with IV contrast immediate postoperation (day 1 of hospitalization) revealed extensive patchy airspace opacities throughout the lungs bilaterally, more prominent centrally with a slight basilar predominance.
Laboratory studies revealed leukocytosis (WBC 13,000/μL) with normal hemoglobin and natriuretic peptide levels. Cardiac and allergic causes of pulmonary edema were excluded. The clinical presentation was consistent with NPPE due to acute upper airway obstruction post-extubation, likely from transient laryngospasm.
Supportive treatment included oxygen via Venturi mask (FiO2 0.5), inhaled salbutamol, and a single dose of intravenous furosemide (20 mg). The patient’s respiratory status improved over the following 48 hours. Repeat imaging on day 3 showed near-complete resolution of pulmonary edema. The patient was discharged home in stable condition on postoperative day 3 (Figure 3A & 3B).
Figure 3: Radiographic images of the chest on day 2 (A) and day 3 (B) of hospitalization revealed improvement in pulmonary edema and nearly resolution of pulmonary edema, respectively.
Discussion
NPPE arises when vigorous inspiratory efforts against an occluded airway create a sudden drop in intrathoracic pressure (as low as −100 cm H2O), leading to increased venous return and pulmonary capillary transudation [3-6]. The resulting hydrostatic pressure gradient causes rapid fluid extravasation into the alveolar space.
Typical symptoms develop within hours of extubation and include dyspnea, hypoxemia, hemoptysis, and pink frothy sputum [5-7]. Radiographic findings include bilateral central infiltrates without cardiomegaly. Pulmonary CT imaging often reveals diffuse ground-glass opacities [8].
Differential diagnosis includes cardiogenic pulmonary edema, ARDS, neurogenic edema, and anaphylaxis [4]. Point-of-care lung ultrasound may show diffuse B-lines, particularly in anterior and central zones [6].
Treatment is mainly supportive, aimed at oxygenation and maintaining airway patency [1-3]. Noninvasive or mechanical ventilation may be necessary in severe cases [2]. The use of diuretics is debated, as patients are often euvolemic; excessive use can result in hypovolemia and hypotension, particularly in younger individuals [9,10].
The prognosis is generally favorable, with full resolution typically within 24 to 72 hours and no long-term sequelae [4].
Conclusion
NPPE should be considered in any postoperative patient developing acute respiratory distress immediately after extubation, especially in the absence of cardiac or allergic causes [1-4]. Prompt recognition and supportive care are crucial to prevent complications [3-5]. Judicious use of diuretics is advised, balancing fluid removal with the risk of volume depletion [9,10].
References
- Tsai PH, Wang JH, Huang SC, Lin YK, Lam CF. Characterizing post-extubation negative pressure pulmonary edema in the operating room-a retrospective matched case-control study. Perioper Med (Lond). 2018; 7: 28.
- Mankowski ´ W, Radkowski P, Onichimowski D. Dawidowska-Fidrych J. The practical considerations of managing negative pressure pulmonary edema for anesthesiologists – literature review. Polish Ann Med. 2022; 29: 288–91.
- Lemyze M, Mallat J. Understanding negative pressure pulmonary edema. Intensive Care Med. 2014; 40: 1140–3.
- Guru PK, Agarwal A, Pimentel M, McLaughlin DC, Bansal V. Postoperative pulmonary edema conundrum: a case of negative pressure pulmonary edema. Case Rep Crit Care. 2018; 2018: 1584134.
- Malepati S, Samant S, Sietsema KE, Van Natta TL. A 26-year-old man with postextubation dyspnea and hemoptysis. Chest. 2011; 139: 708–11.
- Silva A, Furtado I, Grenho B, Isidoro M. Point of care ultrasound-diagnostic approach of an Atypical negative pressure pulmonary oedema. Turk J Anaesthesiol Reanim. 2022; 50: 306–8.
- Chuang YC, Wang CH, Lin YS. Negative pressure pulmonary edema: report of three cases and review of the literature. Eur Arch Otorhinolaryngol. 2007; 264: 1113–16.
- Barile M. Pulmonary Edema: a pictorial review of imaging manifestations and current understanding of mechanisms of disease. Eur J Radiol Open. 2020; 7: 100274.
- Maxwell BG, Mihm FG. Questioning diuretic use in acute negative-pressure pulmonary edema. Anesthesiology. 2011; 114: 461.
- Krodel DJ, Eikermann M. Acute postoperative negative-pressure pulmonary edema. Anesthesiology. 2011; 114: 462.
