
Open Access, Volume 11
Metastatic pancreatic adenocarcinoma: Long survival associated with ATM mutation
Raquel Gerson-Cwilich1; Lorena Lopez-Zepeda2; José Juan Sanchez-Hidalgo3; Jesús Javier Baquera-Heredia4; Pamela Renee Mendoza-Trillo5; Jesús Enrique Navarrete-Viveros5; Sergio Augusto Gutiérrez-Rueda6; Daniel Romellón-Portela6; Daniela Shveid Gerson7
1Medical Oncology, Residency Program Director and Head of Cancer Center, The American British Cowdray Medical Center, Mexico City, Mexico.
2Medical Oncology, Cancer Center, The American British Cowdray Medical Center, Mexico City, Mexico.
3Department of Resident at Oncology, Universidad Nacional Autónoma de México, Mexico.
4Department of Head of Pathology, Residency Program Director on Clinical-Anatomic Pathology, The American British Cowdray Medical Center, Mexico City, Mexico.
5Department of Pathology, Attendant Physician, Mexico.
6Resident in Clinical-Anatomic Pathology, Universidad Nacional Autónoma de México, Mexico.
7Medical Oncology, Cancer Center, Mexico.
Raquel Gerson-Cwilich
Medical Oncology, Residency Program Director and Head of Cancer Center, The American British Cowdray Medical Center, Mexico City, Mexico.
Email: rgerson1@yahoo.com
Received : May 30, 2025,
Accepted : June 19, 2025
Published : June 30, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Pancreatic cancer is a major cause of cancer-associated mortality. In México the incidence rises to 14.2% compared to 8.0% reported worldwide, and the mortality rate approaches 13.8% compared to global reports. Some risk factors are associated with family history (3 or more direct line family members) and genetic predisposition syndromes, such as hereditary pancreatitis, these in turn may be linked to different germline mutations, one of them being the ATM (Ataxia-telangiectasia) pathogenic variant. Overall, the relative risk of pancreatic cancer is 6.5 (95% CI, 4.5-9.5) in ATM variant carriers compared with noncarriers.
Case presentation: We present a case of a 70-year-old male who was diagnosed with pancreatic cancer, after a weight loss evaluation and an MRI which showed an intraductal papillary mucinous neoplasm in early 2022, which was not treated at the time due to patient refusal. In november 2022 a PET/CT (18F-FDG) scan showed metastatic disease to the liver, confirmed through a core needle biopsy. He tested negative for BCRA mutation, but positive for ATM R35 loss. The patient started systemic treatment with FOLFIRINOX which was later adjusted for toxicity due to grade 3 neuropathy, continuing treatment with FOLFIRI. He underwent a total of 30 chemotherapy until disease progression was documented in November 2024, thus, initiating third line treatment with gemcitabine/nab-paclitaxel. The last evaluation with a PET/CT scan showed stable disease with the new chemotherapy regimen. At the moment the patient has had an overall survival of 28 months, he still is undergoing treatment.
Conclusion: This case highlights the importance of evaluating mutations such as ATM, which have been described, but not yet completely evaluated in the context of pancreatic adenocarcinoma. The association between the use of chemotherapy directed to DNA repair systems, as well as to breakage of DNA, and the function pathway of ATM has demonstrated a prolonged PFS, compared to those patients with non-mutated ATM. The ATM mutation could serve as a prognostic marker for patients with metastatic pancreatic adenocarcinoma.
Keywords: ATM mutation; Irinotecan; Survival; Pancreatic; Genomic; Adenocarcinoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Gerson-Cwilich R (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Gerson-Cwilich R, Lopez-Zepeda L, Sanchez-Hidalgo JJ, Baquera-Heredia JJ, Mendoza-Trillo PR, Navarrete-Viveros JE, Gutiérrez-Rueda SA, et al. Metastatic pancreatic adenocarcinoma: Long survival associated with ATM mutation. Open J Clin Med Case Rep. 2025; 2362.
Introduction
Pancreatic cancer is a major cause of cancer-associated mortality. It is a highly aggressive neoplasm which conveys poor overall survival. According to the Global Cancer Observatory, its incidence is ranked twelfth worldwide with a total of 510,992 cases, being the sixth cancer ranked in mortality with a total of 467,409 cases [1]. In México its incidence rises to 14.2% compared to 8.0% reported worldwide, and its mortality rate approaches 13.8%, compared to 8.2% worldwide [2].
The risk factors for pancreatic cancer can be divided into environmental and hereditary risk factors. According to literature, family history including 3 or more direct family members and genetic predisposition syndromes such as hereditary pancreatitis, can be associated with different germline mutations, one of them being the ATM (Ataxia-telangiectasia) pathogenic variant [3]. ATM is a Ser/Thr protein kinase and is a member of the Phosphoinositide 3-Kinase (PI3K)-related Protein Kinase (PIKK) family, which also includes ATM and Rad3-Related Protein (ATR), the catalytic subunit of DNA-dependent Potein Kinase (DNA-PKcs) and SMG1, a protein kinase that is involved in the DNA-damage response [5,6]. ATM recognizes and responds to DNA Double-Strand Breaks (DSBs) to maintain the integrity of the genome and to minimize the risk of cancer and neurodegeneration. Studies have demonstrated that pathogenic variants in the ATM, BRCA1, BRCA2, CDKN2A, PALB2, PRSS1 STK11, TP53, and Lynch syndrome collectively occur in 4% to 10% of patients with metastatic pancreatic cancer [7].
The cumulative risk of pancreatic cancer among individuals with a germline pathogenic ATM variant was estimated to be 1.1% (95% CI, 0.8%-1.3%) by age 50 years; 6.3% (95% CI, 3.9%-8.7%) by age 70 years; and 9.5% (95% CI, 5.0%-14.0%) by age 80 years. Overall, the relative risk of pancreatic cancer was 6.5 (95% CI, 4.5-9.5) in ATM variant carriers compared with noncarriers. Although the risk of developing pancreatic cancer associated with the pathogenic variant in ATM rises with age, the landscape has been described in different cohorts in patients without KRAS, TP53, CDKN2A and SMAD4 mutations [5]. According to the GENIE (Genomic Evidence Neoplasia Information Exchange) American Association for Cancer Research, among 42 patients, 2.8% presented with ATM alterations. The highest prevalence was described in China (the pancreatic cancer sub-cohort of pan-cancer Chinese Origene) with a 12% prevalence of alterations [8].
The first line therapy for metastatic pancreatic cancer is based on the presence or absence of specific germline pathogenic variants and/or actionable molecular alterations in the tumor. For patients with or without BRCA1/2 or PALB2 pathogenic variants, and with Non-core HRD pathogenic variants, a platinum-based therapy is suggested, such as modified FOLFIRINOX, as it has demonstrated an OS of 11.1 months vs 6.8 months compared to gemcitabine-containing regimens and a PFS of 6.4 months vs 3.3 months [9]. However, in the phase 3 POLO trial, patients who harbor germline BRCA mutations have improved Progression-Free Survival (PFS) with the poly-ADP (adenosine diphosphate)-ribose polymerase inhibitor (PARPi) olaparib in the maintenance setting as compared to placebo (7.4 vs. 3.8 months) [10].
Genotoxic chemotherapies such as irinotecan can cause single-ended double-stranded breaks. DNA repair of such damage mostly involves Homologous Recombination (HR) repair or Non-Homologous End-Joining (NHEJ). In normal cells, the more precise HR repair pathway is the predominant means of double-stranded break repair in the synthesis phase (S Phase). In cells deficient in ATM/Chk2, the error prone NHEJ pathway takes over, leading to genotoxic DNA repair [4]. For patients with metastatic disease at diagnosis, who had an ATM alteration, the median OS was 24.7 vs 6.0 months (HR=0.16, 95% CI=0.04 to 0.71, P=0.02) [11].
Case Report
Diagnosis: In February 2022, a 70-year-old male presented with weight loss of 15 kg for approximately 3 months and consumptive symptoms. He had no past history of any chronic disease nor personal risk factors besides sporadic cigar smoking with a smoking index / pack years calculation which was non-significative. From February through July 2022, he did not seek nor receive medical attention. He continued symptomatic, prompting the need for extensive imaging studies. On July 2022, a Magnetic Resonance Imaging (MRI) was performed showing an Intraductal Papillary Mucinous Neoplasm (IPMNs) of the pancreas (Figure 1). During his evaluation, the patient refused further examination and treatment.
In november 2022 he underwent a new clinical evaluation, with a PET/CT with fluorodeoxyglucose as an imaging agent labeled by a radioactive isotope of fluorine-18 (18F-FDG total of 13.42 mCi) scan, which showed a solid heterogeneous lesion on the tail of the pancreas measuring 41 × 38 × 33 mm with a SUVmax of 7.19. The lesion encased the splenic artery over 180°, with thrombosis over the splanchnic vein. It was associated with para-aortic adenopathies and multiple hepatic intraparenchymal and hypovascular lesions, the largest measuring 17 mm in the segment III with an SUVmax of 19.13 (Figure 2a/b). On November 7th, 2022, he underwent a core needle biopsy of one of the metastatic lesions localized on the left hepatic lobule which revealed a pancreatic adenocarcinoma. On December 7th, 2022 the genomic profiling test Foundation One CDx was used to evaluate for BCRA1/2 mutations; the patient tested negative for BCRA1/2 but positive to ATM R35 loss, as well as KRAS G12V mutation, preserved MSI, and a TMB of 4 mut/Mb. Physical examination at the moment revealed no clinical signs, with a Karnofsky evaluation of 90% and an ECOG of 0.
Chemotherapy: The patient started systemic treatment on November 2022 with FOLFIRINOX (Irinotecan 150 mg/m2, Oxaliplatin 85 mg/m2, 5-Fluorouracil 400 mg bolus and infusion 2400 mg/m2 during 46 hours, adjusted 85% of total dosage) for 4 cycles, however the treatment was discontinued for 2 months due to a traumatic femoral fracture which was surgically resolved. Before the patient resumed treatment, he was evaluated with a new PET/CT scan with fluorodeoxyglucose (18F-FDG) on February 27, 2023 which exhibited a partial response according to Response Evaluation Criteria in Solid Tumor (RECIST) with a decrease of 58% in size of the main lesion in the tail of the pancreas, with a metabolic decrease of 29.5%. The liver was reported to show a decrease in the number of lesions (from 14 to 11) with a reduction of 50.9% of the aforementioned metabolism (Figure 2c).
The patient resumed treatment with the FOLFIRINOX chemotherapy regimen and completed 5 cycles from March 09, 2023 to May 18, 2023 for a total of 9 cycles. A PET/CT 18F-FDG scan conducted on May 2023, demonstrated stable disease according to RECIST compared to the previous study; however, the patient presented grade 3 neuropathy due to oxaliplatin on the 9th cycle of FOLFIRINOX, according to Common Terminology Criteria for Adverse Events (CTCAE) v4.0; whereby chemotherapy was adjusted, and oxaliplatin was discontinued. On June 20, 2023 the patient started treatment with FOLFIRI (Irinotecan 180 mg/m2, 5-Fluorouracil 400 mg bolus and infusion 2400 mg/m2 during 46 hours, adjusted 80% of total dosage) and was again evaluated for response with a PET/CT 18F-FDG scan after the 8th cycle of FOLFIRI which was administered on October 12, 2023.
On November 11, 2023 stable disease according to RECIST criteria was observed in the PET/CT 18F-FDG scan which allowed the patient to continue treatment (Figure 2d). There were no toxicities reported from the patient at each consult, and no clinical signs or symptoms of progressive disease recorded during each clinical examination. No other toxicities were associated with chemotherapy infusion and the patient underwent a total of 30 chemotherapy cycles with FOLFIRI until October 24, 2024. On November 12, 2024 a follow up PET/CT 18F-FDG scan showed progressive disease with increase in number, size and metabolism of the hepatic lesions, notably a metabolic increase of 263% in relation to hypodense lesion in liver segment IV measuring 12 mm, a preexisting lesion in liver segment II with a 133% increase in metabolism and an increase of 50% in size, and a third lesion on segment V, with a metabolic increase of 145% (Figure 2e).
With these new findings, the patient was programed for a new core needle liver biopsy over the right hepatic lobule, which pathology revealed a poorly differentiated pancreatic adenocarcinoma CK7 positive, CK20 positive, SMAD4 negative (loss of expression), Glipican negative (Figure 3). On December 5th, 2024, the patient started a third line of treatment with gemcitabine (1000 mg/m2) and nab-paclitaxel (125 mg/m2) every three weeks completing 3 cycles. The patient was evaluated in January 2025. On follow up his PET/CT 18F-FDG scan showed partial metabolic response of the pancreatic lesion with decrease of 30% in size, and a decrease of more than 30% of the metabolism previously reported in the hepatic lesions, although the size and number remained similar to the previous scan. (Figure 2f). Currently the patient has had an overall survival of 28 months, ongoing continuous treatment, is asymptomatic, dedicated to a full day regular work with a good overall quality of life.
Adverse events: During treatment, the main adverse event was grade 3 neuropathy according to CTCAE v4.0.
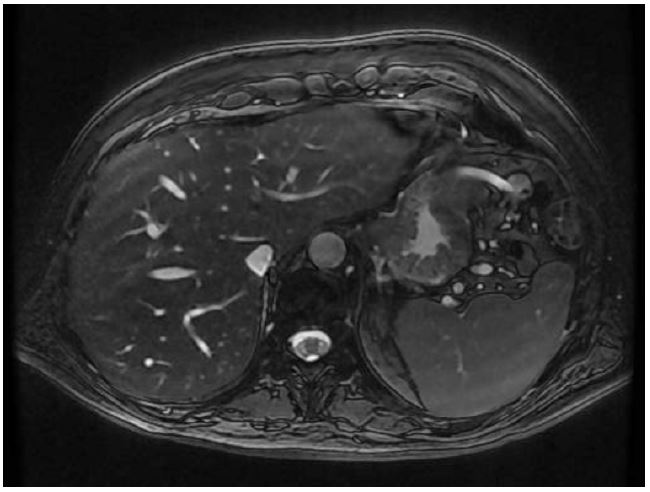
Figure 1: Imaging picture of the first Magnetic Resonance scan (MRI-T2 weighted) at the initial diagnosis showing at least two images: The first described at the tail of the pancreas, heterogeneous and hyperintense due to a small nodule, which measures 9 mm on its longest axis. The second at the distal edge of the pancreatic tail, with a thin wall, multilobulated with homogeneous hyperintense content on T2-weigthed, measuring 20×9 mm, which is dependent on the main pancreatic duct and causes dilation of the adjacent segment up to 4 mm associated with parenchymal atrophy.
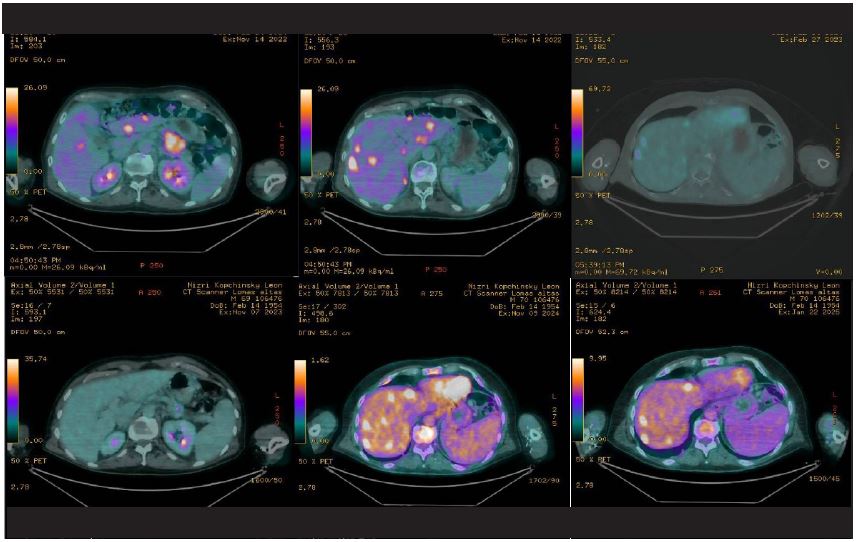
Figure 2: Imaging pictures of patients before, during, and after treatment. (A & B) depicts the primary lesion with a PET/CT with fluorodeoxyglucose as an imaging agent labeled by a radioactive isotope of fluorine-18 (18F-FDG total of 13.42 mCi) scan shown a solid heterogeneous lession on the tail of the pancreas measuring 41×38×33 mm with a SUVmax of 7.19. The lession encases the splenic artery over 180°, with thrombosis over the splacnic vein. It is associated to a para-aortic adenopathy and multiple hepatic intraparenchomatous and hypovascular lessions (at least 14, the biggest measuring 17 mm at the segment III and SUVmax 19.13) associated with metastasic disease. (C & D) shows the response to initial treatment, and during maintenance with stable disease. (E) depicts progressive disease after treatment with increase in number, size and metabolism of the hepatic lesions, which reported: On segment 4, an increase in metabolism out of 263% over a new hypodense lesion measuring 12 mm; on segment 2, a preexisting lesion with an increase in metabolism of 133% and increase of 50% in size. × shows the follow up scan after second line treatment with change in chemotherapy, with response over metabolism measured in SUV max.
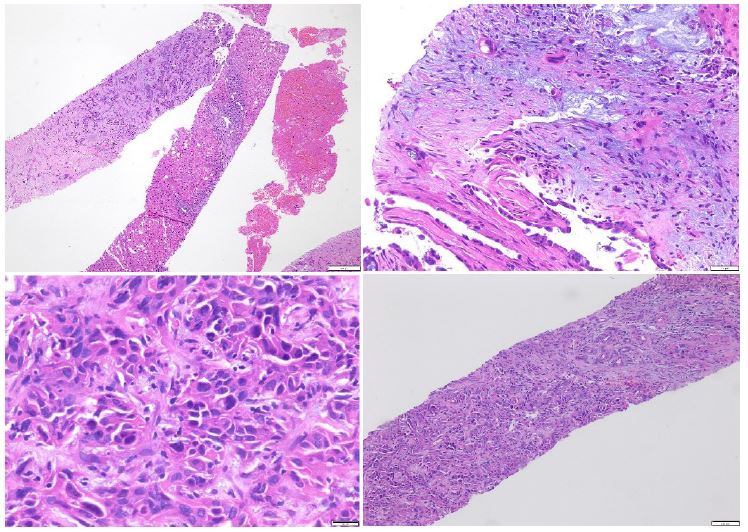
Figure 3: Pathology description of hepatic biopsy: (A) Residual hepatic parenchyma which is infiltrated by a poorly differentiated neoplasm with solid growth pattern and marked desmoplastic reaction. (B) Referred as hepatic parenchyma showing prominent desmoplastic stroma with myxoid sites. At the bottom is shows glandular tissue with pleomorphic cells. (C) Description of the main neoplastic tissue: composed of large cells with abundant and eosinophilic cytoplasm, it is shown with loss of the nuclear-cytoplasm relation as well as marked pleomorphism and nuclear hyperchromasia. (D) Substitution of hepatic parenchyma with neoplasia, with desmoplastic stroma, ductular reaction within the surrounding fibrous stroma and scarce chronic inflammatory infiltrates.
Discussion
The cornerstone treatment for patients with metastatic adenocarcinoma is systemic chemotherapy with FOLFIRINOX or mFOLFIRINOX. This takes into account divergent pathways that the clinician must evaluate in order to confer the best management to the patient. This usually includes performance status, comorbidities, actionable germline and somatic molecular alterations, and goals of care.
Within this context, according to NCCN (National comprehensive Cancer Network) guidelines and ESMO (European Society of Clinical Oncology) guidelines [12,13] the first line treatment in advanced pancreatic adenocarcinoma regardless of actionable mutations (BRCA1/2, non-core HDR), the efficacy of FOLFIRINOX over gemcitabine alone in patients with ECOG PS 0-1 and bilirubin level <1.5 times the Upper Limit of Normal (ULN) has demonstrated Overall Survival (OS) of 11.1 months vs 6.8 months, with a Progression Free Survival (PFS) of 6.4 months vs 3.3 months [14]. Recently the use of NALIRIFOX significantly improved the PFS and OS in the NALIRIFOX arm [mOS: 11.1 months versus 9.2 months in the GN arm (HR 0.83, 95% CI 0.70-0.99, P=0.04) [15].
In patients who have a BRCA1/2 mutation or core HDR mutation, the use of Olaparib maintenance therapy has reached a median OS 18.9 versus 18.1 months, HR 0.91, 95% CI 0.56-1.46 and a median PFS 7.4 versus 3.8 months, as compared to placebo. With rucaparib, as an option for maintenance therapy the median PFS and OS were 13 and 23 months, respectively [16].
For other actionable mutations, the use of directed therapy is suggested over chemotherapy. For example, patients with mismatch repair deficient (dMMR)/Microsatellite-Instability High (MSI-H), the use of pembrolizumab or nivolumab/ipilimumab are considerable options. In patients with Neurotrophic Tyrosine Receptor Kinase (NTRK) gene fusion, the use of an inhibitor such as larotrectinib, entrectinib or repotrectinib is described. Reasonable options for those who test positive for Rearranged During Transfection (RET) gene fusions are selpercatinib and for patients with BRAF V600E mutation, the use of a BRAF plus MEK inhibitor combination, as has been evaluated in phase II trials.
However, these guidelines do not have a straightforward recommendation for patients with an ATM alteration. The literature describes patients with an ATM alteration in pancreatic cancer [17] with a median of 2-year survival of 33%, with a mortality HR of 1.2 (0.8, 1.7 with 95% CI). However, there is limited clinical experience in this scenario. In a case series, 80% of patients with ATM, ATR, or CHEK2 mutations were treated with an oxaliplatin-based chemo-therapy and 62.5% demonstrated partial response or stable disease on first follow-up scans [17]. There was also a significantly longer progression-free survival compared with those patients whose tumors were DDR-non mutated (20.8 months vs. 1.7 months, respectively P=0.049). Specifically, 4 of 30 patients had known pathogenic ATM mutations, with at least one patient experiencing a prolonged partial response of nearly 40 months on 5-FU, irinotecan, and oxaliplatin [18].
Here, we described a patient who has reached an overall survival of 28 months with pancreatic adenocarcinoma. There have been associations of irinotecan-based chemotherapy which have shown better outcomes in patients with ATM alterations, which suggest that it can play a role in the overall survival of these patients. Notwithstanding, our patient is still ongoing treatment with a third line of chemotherapy, which has been above the median OS compared with that described in first line treatments maintenance therapy with Olaparib and BRCA1/2 mutations, and in patients with no alterations whatsoever.
Irinotecan containing chemotherapy examined in patients with ATM alteration show a median PFS for best irinotecan-based line (no platinum/PARP-inhibitor) of 12 months; for best platinum- or PARP-inhibitor-based line (No-irinotecan) of 2.8 months; and for best treatment containing no irinotecan, platinum or PARP-inhibitor, of 4.2 months (P=0.018) [19].
Conclusion
Our findings might suggest that patients with an ATM mutation who are treated with irinotecan-based chemotherapy could manifest better outcomes in terms of progression free survival and overall survival, as well as in quality of life. Our patient reached 28 months of OS which could make a change in the decision directly to evaluate for the ATM mutation that could serve as a prognostic marker for patients with metastatic pancreatic adenocarcinoma.
Declarations
Statement of ethics: This retrospective review of patient data did not require ethical approval in accordance with institutional guidelines.
Conflict of interest statement: The authors have no conflicts of interest to declare.
Funding sources: study was not supported by any sponsor or funder.
Author contributions: Clinical diagnosis, treatment, follow up: Gerson-Cwilich, Shveid-Gerson, López-Zepeda, Sánchez-Hidalgo. Pathologic diagnosis and evaluation: Baquera-Heredia, Mendoza-Trillo, Navarrete-Viveros. Acquisition of patient data: Sánchez-Hidalgo, Gutierrez-Rueda, Romellón-Portela. Manuscript writing: Sánchez-Hidalgo. Manuscript supervision: All authors read and approved the final manuscript.
Data availability statement: All data generated or analyzed during this study is included within this article. Further inquiries can be directed to the corresponding author.
References
- Sethi S, Debiec H, Madden B, Charlesworth MC, Morelle J, Gross L, et al. Neural epidermal growth factor-like 1 protein (NELL-1) associated membranous nephropathy. Kidney Int. 2020; 97: 163-174.
- Alsharhan L, Beck LH Jr. Membranous Nephropathy: Core Curriculum 2021. Am J Kidney Dis. 2021; 77: 440-453.
- Sharma Y, Jain A, Gupta P, Tiwari V, Gupta A, Bhargava V, et al. NELL-1 Associated Membranous Nephropathy - A Case Series from India. Indian J Nephrol. 2024; 34: 654-656.
- Ronco P, Plaisier E, Debiec H. Advances in Membranous Nephropathy. J Clin Med. 2021; 10: 607.
- Mohamed Jiffry MZ, Pitts K, Munir M, Khan A, Josephs M. A Rare Case of Neural Epidermal Growth Factor-Like 1 Protein (NELL-1) Antigen-Associated Membranous Nephropathy. Cureus. 2023; 15: e34713.
- Nassar R, Kadhem SA, Shakir M. Lipoic Acid as a Trigger for NELL-1 Positive Membranous Nephropathy. Kans J Med. 2023; 16: 297-298.
- Alsharhan L, Beck LH Jr. Membranous Nephropathy: Core Curriculum 2021. Am J Kidney Dis. 2021; 77: 440-453.
- Sultan A, Mamankar D, Thakare S, Rojekar A, Jamale T. Mercury-associated Neural Epidermal growth factor-Like 1 protein (NELL-1) positive membranous nephropathy after use of skin lightening creams. Clin Toxicol (Phila). 2023; 61: 387-391.
