
Open Access, Volume 11
Use of cupping for spasticity management: A pilot case study
Bryn Hager, PT, DPT, PCS, CBIS; Faye Akin, DPT; Joshua Lopez, DPT; Camden Roth, DPT; Stefanie Bond, PT, DPT, GCS
School of Physical Therapy & Rehabilitation Sciences, University of South Florida, USA.
Hager Bryn
School of Physical Therapy & Rehabilitation Sciences, University of South Florida, USA.
Email: brynhager@usf.edu
Received : April 14, 2025,
Accepted : May 13, 2025
Published : May 15, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Background and purpose: Spasticity, a velocity-dependent increase in muscle tone, significantly impacts individuals with neurological conditions. Current treatments often involve pharmacological interventions with notable limitations, including adverse effects and inconsistent efficacy. This pilot case study explored the use of dry cupping therapy as a novel, cost-effective approach for spasticity management.
Case description: A 62-year-old male with left-sided spasticity secondary to a stroke participated in an 8-week cupping intervention targeting affected muscle groups.
Intervention: The therapy was administered 1-2 times weekly before physical therapy sessions. Outcome measures included the Modified Ashworth and Modified Tardieu Scales, the 6 Minute Walk Test, 10 Meter Walk Test, and Observational Gait Scale.
Outcomes: Improvements in muscle tone and spasticity were observed, with notable reductions in the Modified Ashworth and Modified Tardieu Scale scores across muscle groups. Functional outcomes included a 13.72-meter improvement in the 6 Minute Walk Test and a significant increase in Observational Gait Scale scores (from 5 to 15). Minimal adverse effects, such as mild bruising and transient nerve pain, were reported. The patient and his spouse noted sustained improvements in muscle tone at 4-week follow-up.
Discussion: Dry cupping therapy demonstrated potential as a non-invasive and accessible intervention for spasticity reduction and functional improvement. Cupping therapy possesses potential to influence clinical guidelines or practices for spasticity management in diverse neurologic populations. While findings are promising, further research with larger sample sizes and randomized controlled trials is necessary to establish efficacy, optimize parameters, and explore broader applications in neurological populations.
Keywords: Spasticity; Stroke; Cupping therapy; Novel treatment; Case study.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Hager B (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Hager B, Akin F, Lopez J, Roth C, Bond S. Use of cupping for spasticity management: A pilot case study. Open J Clin Med Case Rep. 2025; 2353
Introduction
Spasticity is defined as a velocity-dependent increase in muscle tone and frequently occurs after neurological injuries or due to neurological disorders [1]. It can significantly impact volitional control for individuals with this condition, often interfering with their ability to perform daily tasks, increasing time and effort to complete tasks, and prompting frustration [2-4]. Spasticity’s effects on movement are particularly pronounced in anti-gravity muscles, where it affects the ability to control specific muscle groups and prevents individuals from performing basic movements [3].
Assessment and treatment of spasticity is common for physical therapists due to its impact on quality of life, and management of spasticity is critical to improving functional outcomes [5]. Various interventions are used to manage spasticity across providers; however, limited evidence exists to determine the best choice amid current treatments [1,5]. This has presented a research gap and supports the need for alternative approaches to spasticity management. Additionally, access to interventions may vary be patient demographic, providers, and regions [1], further supporting the need for more accessible interventions.
The inception of this study was the principal investigator’s anecdotal experience and success with cupping therapy for spasticity management in clinical practice. This was an incidental finding, but after initial success, they developed further interest in understanding its clinical utility. It was explored with various neurological populations in a day rehabilitation setting. Due to success across ages, demographics, and diagnoses, interest grew in understanding how cupping therapy could be further utilized in clinical practice.
Cupping therapy involves the application of glass or plastic cups over a muscle [1]. Suction is created, which can impact blood flow, muscle relaxation, and pain [1]. Current research on cupping surrounds musculoskeletal populations, with limited data on use for neurological patients [1]. A scoping review was conducted in 2024 [1], identifying many key factors to cupping’s potential for success clinically. These include fewer identified negative side effects than current treatment options, decreased duration of adverse effects, reduced administration time, and reduced cost for implementation and administration [1]. Cupping therapy demonstrated potential as a novel treatment for spasticity management, with the capacity to modulate hyperactive stretch reflexes [6], increase inhibitory activity at the spinal cord level, and ultimately decrease spastic response [1,7]. Limitations of the scoping review highlighted the minimal amount of research that exists related to neurologic populations [1], which supports the need for initial data on implementation. There is no current guidance on best practice parameters for administration of cupping therapy for neurologic populations. For these reasons, a clinical case study was pursued.
The intention of the study was to quantify any changes following cupping administration, as well as describe effects of the intervention.
Case Description
Our scoping review was conducted beginning in March of 2024, which served as support for this study. The IRB process for the case study began in June 2024, with our patient identified as an appropriate candidate in July 2024. IRB approval was received in September 2024, and study protocol began shortly thereafter. The study ran for eight weeks and concluded in November 2024. At the time of the study, our patient was not on spasticity medications, nor was he receiving Botox injections. This remained consistent throughout the study.
Inclusion criteria for this study included any individual over the age of 18 with a neurological diagnosis presenting with changes in muscle tone and/or spasticity associated with the diagnosis. Exclusion criteria included individuals under the age of 18, contraindications to cupping therapy, and those that experienced changes in tone and/or spasticity that is not due to a neurological condition.
Our patient was a 62-year-old left-handed male. His stroke occurred on November 2, 2023 (age 61). He received six weeks of inpatient rehabilitation, including occupational, physical, and speech therapy. Following discharge, he had been seen by home health for four weeks, then outpatient therapy beginning in February 2024. During his initial physical therapy evaluation, he reported symptoms of left upper and lower extremity weakness and decreased coordination of his left hand. He also reported difficulty with walking, balance, fine motor skills, and performing household tasks due to the dysfunction of his left hand. At the time of his evaluation, the patient used a hemi-walker for ambulation.
Initial and final testing for this study included the 6 Minute Walk Test, 10 Meter Walk Test, Observational Gait Scale, Modified Ashworth Scale, and Modified Tardieu Scale. Every two weeks, the Modified Ashworth and Modified Tardieu Scales were readministered to track results (Table 1). These measures were selected due to their psychometric data and support for use in the stroke population [8,9], as well as ability to capture changes in tone and function. To maintain consistency, only the principal and co-investigator performed these measures. Regarding the 6 Minute Walk Test and 10 Meter Walk Test, therapist 1 guarded the patient, and therapist 2 kept track of time and conducted measurements. This was consistent at both initial and final testing. When performing the Observational Gait Scale, both investigators separately completed the measure after watching the patient ambulate for approximately two minutes. They compared results to ensure agreement of findings. For initial and final testing, scores were consistent between both parties. Regarding the Modified Ashworth Scale, each investigator performed the assessment at the joints independently, then compared results to ensure consistency. During the Modified Tardieu, therapist 1 positioned limbs at R1 and R2, and therapist 2 took goniometric measurements. The patient continued with outpatient physical therapy following the conclusion of the study.
Intervention
Dry cupping was administered to the patient’s left side by either the principal investigator or co-investigator. Training and review of technique between investigators was conducted prior to the first administration to ensure consistency. Cups were placed throughout the upper and lower extremities and involved the following muscle groups: deltoid, biceps brachii, brachioradialis, wrist flexors, hamstrings, and gastrocnemius. This was based upon scores from the Modified Ashworth and Modified Tardieu Scales, with modification to number and location of cups also based upon scores on these measures. If scores were noted to have decreased and remained consistent for 2-3 sessions, administration of cups was ceased. This was used as a benchmark to determine any possible carryover effects. Specifically, this was trialed with the hamstrings and gastrocnemius muscles. Because spasticity remained high in the upper extremity, cups continued to be placed on the limb throughout the study.
A variable number of cups were applied, which was dependent upon patient response to treatment. This number ranged from 4-12, with more cups being used during initial sessions and fewer cups as sessions progressed (Figure 1, Tables 2,3). Skin inspection was completed prior to and immediately following administration, as well as throughout the therapy session. Cups were also cleaned prior to and following administration. These procedures were implemented for safety and to maintain appropriate hygiene. The specific brand of cups used was “Professional Cupping Set” by K.S. Choi Corp [10] and was acquired from Amazon.
Outcomes
The patient’s condition was monitored immediately after cupping administration, throughout the session, and upon return to the clinic for the next visit. Immediately after administration, markings on the skin were typically noted, with six instances in which bruising was observed. If bruising was present, it lasted no longer than until the next session (from two to five days later). This correlates with findings of typical dry cupping adverse effects [1] (Tables 4 & 5).
Clinicians also noted a change in muscle tone and presentation following cupping administration. Most notably, the targeted muscles had a flaccid or more hypotonic presentation. Joint range of motion was also observed to increase following administration. Re-measurement was not performed after cupping due to time constraints. Other observed functional changes include achieving full weight bearing on the lower extremities and improved heel strike during gait training, as well as grasp and release and fine finger motor movements in the upper extremity.
As sessions progressed, it was noted that muscle definition of the targeted muscles improved. This was most significant in the biceps and may be attributed to improved volitional control and muscle activation with inhibited spasticity. Notably, during week three (session five), the patient reported he could feel the suction of the cups (deep pressure sensation). Prior to this, the patient had absent sensation in his affected extremities. In week five (session seven), the patient reported new onset of nerve pain, which was described as numbness, tingling, sharp/shooting pain, and an electric sensation from his trunk down to his knee. He indicated this nerve pain over the next week, after which the sensation subsided. This finding correlates with recent research that supports cupping has the ability to improve physiological responses and processing of sensory information [11,12]. These changes in sensation are integral to and closely linked with motor recovery following a stroke [13,14]. From this, we postulate the addition of cupping therapy contributed to sensory and motor nerve recovery in our patient.
Functional measures assessed for this study include the 10 Meter Walk Test, 6 Minute Walk Test, and Observational Gait Scale. These were chosen due to the patient’s greatest self-reported limitation being gait speed and efficiency. His primary therapist also agreed with this assessment. Between initial and final testing, the 10 Meter Walk Test speed stayed relatively the same. His 6 Minute Walk Test improved from 93.88 meters to 107.6 meters (13.72-meter improvement), which did not meet MCID for this patient population [15]. His Observational Gait Scale score increased from 5 to 15 out of a possible 22 points. This measure does not currently have MDC or MCID data to determine if this was a significant change.
Table 1:
| Week | 10 MeterWalk Test (meters/ second) | Comments | 6MinuteWalk Test(meters | Comments | Observational Gait Scale(22 points maximum) | Comments | Modified Tardieu Scale | Modified Ashworth Scale |
|---|---|---|---|---|---|---|---|---|
| 1 | 36.9 seconds(0.271 m/s) self-selected; 32.49seconds (0.308m/s) fast | NBQC | 93.88m (308feet) | NBQC | 5 | NBQC | Ankle: R1 -15, R2 -5 (10),Knee: R1 -10, R2 0 (10), Wristflexors: R13, R2 14 (11),Elbow flexors: R1 91,R2 145 (54) | Hamstring: 1, Gastroc: 1+ with 2 beats of clonus noted, Elbow flexors 3, Elbow extensors 0,Wrist extensors 0, Wrist flexors1+ |
| 2 | ||||||||
| 3 | Ankle: R1 -10, R2 -5(5), Knee: R 1-2, R2 0 (2),Wrist flexors: R1 40,R2 45 (5), Elbowflexors: R1 163,R2 171 (8) | Hamstring: 0, Gastroc: 1+, Elbowflexors 1+, Elbow extensors 0, Wrist extensors 0, Wrist flexors1 | ||||||
| 4 | ||||||||
| 5 | Ankle: R1 -3, R2 0(3), Knee: R 1 0,R2 0 (0), Wristflexors: R1 70,R282 (7),Elbow flexors: R1 132, R2172 (40) | Hamstring: 0, Gastroc: 1, Elbowflexors 1+, Elbow extensors 0, Wrist extensors 0, Wrist flexors1 | ||||||
| 6 | ||||||||
| 7 | Ankle: R1 -12, R2 -5 (7),Knee: R13 R2 0 (3),Wrist Flexors: R1 40 R260 (20),Elbow flexors: R1 99, R2170 (71) | Hamstring: 0, Gastroc L: 0,Elbow flexors: 1+, Elbow extensors 0, Wrist extensors 0,Wrist flexors: 1 | ||||||
| 8 | 39.11 seconds(0.255 m/s) self-selected; 34.4(0.29 m/s) fast | NBQC | 107.6m (353feet) | NBQC | 15 | NBQC | Ankle: R1 -20, R2 -8 (12),Knee R10 R2 0 (0),Wrist Flexors: R1 60 R264 (20),Elbow flexors: R1 110 R2177 (61) | Hamstring: 0, Gastroc L 0, Elbowflexors: 1+, Elbow exensors 0, Wrist extensors 0, Wrist flexors1+ |
Table 2:
| Date | Week | Location of cupping application | Number of unitsapplied |
|---|---|---|---|
| 9/17/24 | 1 | Left hamstring, bicep, wrist flexors | 5 |
| 9/19/24 | 1 | Left hamstring, bicep, wrist flexors,lateral deltoid | 8 |
| 9/24/24 | 2 | Left hamstring, gastrocnemius, bicep,wrist flexors, lateral deltoid | 12 |
| 9/26/24 | 2 | ||
| 10/1/24 | 3 | Left hamstring, gastrocnemius, bicep,and wristflexors | 11 |
| 10/3/24 | 3 | Left hamstring, gastrocnemius, bicep,wrist flexors | 12 |
| 10/8/24 | 4 | ||
| 10/10/24 | 4 | ||
| 10/15/24 | 5 | Left hamstring, gastrocnemius, bicep,wrist flexors | 11 |
| 10/17/24 | 5 | Left gastrocnemius, bicep,brachioradialis, wrist flexors | 8 |
| 10/22/24 | 6 | Left gastrocnemius, bicep,brachioradialis, wrist flexors | 8 |
| 10/24/24 | 6 | Left gastrocnemius, bicep,brachioradialis, wrist flexors | 9 |
| 10/29/24 | 7 | Left bicep,brachioradialis, wristflexors | 4 |
| 10/31/24 | 7 | Left bicep,brachioradialis, wristflexors | 5 |
| 11/5/24 | 8 | Left bicep,wrist flexors | 6 |
| 11/7/24 | 8 | Left bicep,brachioradialis, wristflexors | 7 |
Table 3:
| Muscle (group) | Number of cupping therapyapplications |
|---|---|
| Hamstring | 6 |
| Gastrocnemius | 7 |
| Biceps brachii | 13 |
| Wrist flexors | 13 |
| Lateral Deltoid | 2 |
| Brachioradialis | 6 |
Table 4:
| Effect | Occurrences noted |
|---|---|
| Mild ecchymosis/marking | 6 |
| Difficulty maintaining suction | 2 |
| Bruising | 4 |
| New onsetnerve pain | 2 |
| Cups fallingoff frequently | 1 |
Table 5:
| Effect | Occurrences Noted |
|---|---|
| Improved elbowextension | 1 |
| Full graspand release motionin left hand | 1 |
| Improved heel strike at home | 1 |
| Improved gait speedand foot clearance on treadmill | 2 |
| Reduced nervepain over time | 1 |
| Better musclerelaxation and appearance | 2 |
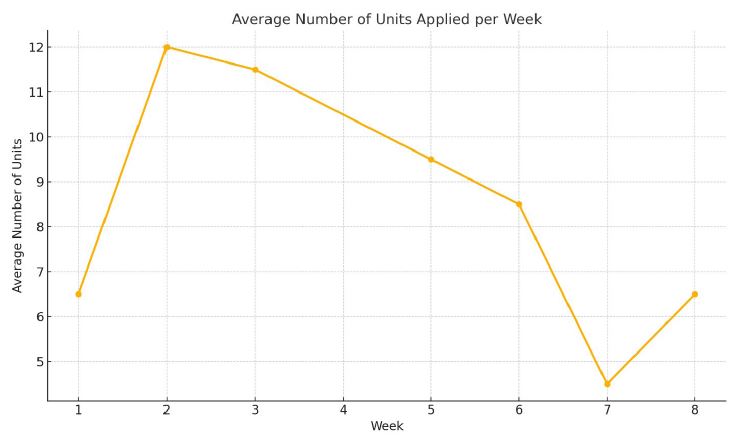
Figure 1:
Outcome measures to assess spasticity and tone include the Modified Ashworth Scale and Modified Tardieu Scale. These were chosen due to strong psychometric properties to assess tone and spasticity and changes in these measures [8,9], as well as their clinical utility and frequency of use in clinical settings. Results are included in Table 1.
Discussion
This pilot case study presented a novel approach to spasticity management. It examined the application of dry cupping therapy in a patient with left-sided spasticity secondary to a chronic stroke, who had received no prior spasticity management. Over an 8-week period, improvements in muscle tone, sensation, motor capacity, range of motion, and functional performance were observed, with minimal adverse effects. The intervention targeted spastic muscles in the upper and lower extremities, demonstrating a reduction in spasticity as measured by the Modified Ashworth and Modified Tardieu Scales and improved functional outcomes, including a substantial increase in Observational Gait Scale scores and slight progress in gait efficiency on the 6 Minute Walk Test.
Results from the Modified Ashworth and Modified Tardieu Scales will be discussed by joint
The ankle measurements indicate moderate variability in the dynamic component of spasticity over time, with R2 - R1 differences ranging from three to 12 degrees. The ankle appears to have a relatively low dynamic component in most weeks, indicating that spasticity is not the primary restriction for ankle range of motion. Rather, this would be due to a restriction in the joint itself (musculoskeletal in nature). The ankle joint had a slight increase in muscle tone, with a catch (1+) notable upon initial evaluation. This maintained for a period, then eventually decreased to a 1. Of significance, this score (1) was maintained throughout the remainder of the study, despite cessation of cupping therapy administration to the gastrocnemius.
The knee shows a progressively decreasing dynamic component over time. This pattern may suggest a decrease in spasticity and improved ROM, possibly due to the intervention. The hamstring demonstrated minimal spasticity initially (1), with a decrease to no spasticity (0). Of significance, this change was also maintained throughout the course of the study, despite cessation of cupping therapy administration to the hamstring once a score of 0 was achieved across multiple sessions.
The wrist flexors show variability in the R2 - R1 difference, ranging from 4 to 20 degrees, indicating inconsistent changes in the dynamic component of spasticity. However, by Week 8, the difference reduced to 4 degrees, suggesting a lower dynamic component, potentially indicating a reduction in spasticity. The wrist flexors demonstrated slight increase in muscle tone, with a catch (1+) notable upon initial evaluation. This was maintained for a period, then eventually decreased to a 1.
The elbow flexors display the largest and most variable dynamic component, with R2 - R1 differences ranging from 8 to 71 degrees. This indicates that spasticity is significantly restricting elbow range of motion and remains the primary barrier to full elbow function. The elbows demonstrated the greatest degree of spasticity upon initial evaluation (3), with a consistent increase in muscle and difficulty performing passive movement. This decreased to a 1+, which was maintained throughout the study.
MCID was achieved for all muscle groups on the Modified Ashworth Scale [8]. Achieving MDC on the Modified Tardieu Scale was seen at the elbow and wrist flexors, specifically change in R1, and at the elbow flexors for change in R2 [9]. Due to the current MDC values and initial deficits in range of motion, these changes were not seen in the lower extremity joints (i.e. MDC was more degrees of change than the patient was lacking in those joints). The Modified Ashworth Scale demonstrates adequate to excellent test-retest reliability, as well as adequate intra-rater reliability [8]. The Modified Tardieu Scale demonstrates excellent test-retest reliability [9].
From these results, we can conclude that the addition of cupping therapy to the patient’s treatment sessions significantly improved his tone and spasticity. We can also confidently conclude this noted change was attributed to actual change in the patient’s condition rather than random variation or measurement error. The results signify that changes achieved are beyond the threshold for meaningful gains in terms of improving a patient’s condition, function, or quality of life. Incorporating these psychometric properties and analysis has allowed us to ensure valid interpretation of changes in the outcome measures. We have also bridged the gap between statistical outcomes and real-world clinical impact, ensuring that reported changes are both measurable and relevant to the patient’s well-being.
Anecdotally, both investigators felt the patient’s change in gait quality had significantly improved from when he began the study. He was more agreeable to trialing an orthotic by the end of the study, as his comfort with wearing the device had improved. We believe this may be attributed to reduced tone impacting its fit at the ankle. His primary therapist also noted that the 8-week period in which cupping therapy was administered was the greatest improvement they had seen in his gait quality, consistency, and carryover since beginning his outpatient therapy visits.
It is worth commenting on not achieving the MCID for the 6 Minute Walk Test and 10 Meter Walk Test. While this may initially present a concern for the implication of cupping therapy on function, this finding does align with multiple other studies. Specifically, literature across age groups and demographics demonstrates that changes in the body structures and functions domain of the ICF model, for example strength, range of motion, and tone, do not necessarily lead to meaningful gains in function or associated outcome measures [16-21]. Rather, addressing these deficits to increase participation in functional task practice does ensure meaningful improvements in the participation domain [16-21]. This literature also supports a holistic approach and integration across domains of the ICF model [16-21]. From this, we can gather that while the immediate changes our patient demonstrated in tone and spasticity did not significantly improve his gait during the study, they did allow him to improve his participation in functional practice during his subsequent physical therapy sessions. This integration should ultimately facilitate meaningful improvements in his participation.
This assessment was echoed by both the patient and his spouse during the four week follow up conversation. Their report was an improvement in the patient’s status following the intervention, though no significant changes in activities of daily living were noted. Their subsequent recommendation was that more patients should be involved in this practice and that cupping therapy should begin sooner after a stroke occurs.
The success of this intervention highlights the potential of dry cupping therapy to offer a cost-effective, minimally invasive alternative for spasticity management. These findings align with limited evidence in the existing literature suggesting that cupping may reduce muscle stiffness and improve local circulation [1]. The apparent carryover effect seen in this study, such as sustained reductions in spasticity despite cessation of cupping in certain muscle groups, warrants further exploration. However, the variability in response between muscle groups, such as the persistent spasticity in the elbow flexors, points to the need for better understanding of the therapy’s mechanisms and application parameters. It is our recommendation that these results be expanded upon in the form of additional case studies, a case series, cohort studies, or randomized controlled trials. A randomized controlled trial would allow for highest quality assessment and further establish appropriate patient demographics and treatment parameters.
Strengths of the study include patient compliance, the use of standardized outcome measures, and offering a novel contribution to literature. The patient adhered well to the intervention schedule, with an 81% attendance rate. This aligns with standard attendance rates in outpatient clinics [22]. The use of validated scales and repeated assessments by the same investigators ensured consistency. This is one of the first studies to systematically explore dry cupping for spasticity in a neurological population, adding to a limited body of evidence.
Limitations of the study can be contributed to the sample size, protocol variability, and noted adverse effects. As a single case study, the findings lack external validity and cannot yet be generalized to broader populations. With no established guidelines for cupping in neurological populations, the intervention relied on clinical judgment, which may limit reproducibility at this time. While minor, transient nerve pain experienced by the patient underscores the need for careful monitoring and further study of potential risks. All of these limitations can be addressed by growing the body of literature surrounding this topic.
Conclusion
This pilot case study provides preliminary evidence supporting the use of dry cupping therapy as an adjunctive intervention for managing spasticity. Notable improvements in muscle tone, as evidenced by changes in the Modified Ashworth Scale and Modified Tardieu Scale, were observed alongside qualitative improvements in functional performance. While the 6-Minute Walk Test and 10-Meter Walk Test did not meet minimal clinically important differences, enhancements in gait quality and caregiver-reported improvements underscore the potential for cupping therapy to facilitate functional participation and quality of life. Results demonstrate its feasibility, tolerability, cost-effectiveness, and sustained carryover. This may influence clinical practice by providing an alternative intervention for clinicians.
The findings emphasize the importance of addressing body structure and function impairments as a means to optimize participation in functional tasks. Cupping therapy demonstrated minimal adverse effects, cost-effectiveness, and ease of administration, making it a feasible option for integration across clinical settings. However, limitations such as small sample size, lack of standardized protocols, and variability in response highlight the need for further rigorous research, including randomized controlled trials.
Future investigations should aim to determine optimal dosage parameters, explore its applicability across diverse neurological populations, and examine the long-term effects on both spasticity and functional outcomes. By expanding the body of evidence, cupping therapy could serve as a valuable, patient-centered intervention to enhance rehabilitation outcomes in neurologic populations.
Declarations
Informed consent: Informed consent was obtained from the participant prior to initiation of the study. This case study follows CARE guidelines and met our institutional Health Insurance Portability and Accountability Act (HIPAA) policy requirements for disclosure of protected health information.
Funding: There were no sources of funding for this study. There are no conflicts of interest to report.
References
- Hager B, Akin F, Brant S, Lopez J, Roth C. Use of Cupping for Spasticity Management in Neurologic Populations: A Scoping Review. 2024.
- Bhimani R, Anderson L. Clinical understanding of spasticity: implications for practice. Rehabilitation research and practice. 2014: 279175.
- Sathian K, Buxbaum LJ, Cohen LG, Krakauer JW, Lang CE, Corbetta M, et al. Neurological principles and rehabilitation of action disorders: common clinical deficits. Neurorehabilitation and neural repair. 2011; 25: 21S–32S.
- Sakel M, Saunders K, Faruqui R, Keene J, Wilkinson DT. Living with spasticity during the covid‐19 pandemic: a qualitative study of patient, carer and physician experiences. Health Expectations. 2024: 27.
- Howard IM, Patel AT. Spasticity evaluation and management tools. Muscle & Amp Nerve. 2023; 67: 272-283.
- Wang Y, An C, Song S, Lei F, Wang Y. Cupping therapy for knee osteoarthritis: a synthesis of evidence. Complementary Medicine Research. 2018; 25: 249-255.
- Çetinkaya A, Fidan E, Göksu S, Bozat BG, Demír Ş. Evaluation of the protective effect of the cup therapy on the epileptic seizure in rats. Konuralp Tıp Dergisi. 2021; 13: 606-613.
- Shirley Ryan AbilityLab. 2021. Ashworth Scale/Modified Ashworth Scale. 2024, from https://www.sralab.org/rehabilitation-measures/ashworth-scale-modified-ashworth-scale#stroke
- Shirley Ryan AbilityLab. 2016. Tardieu Scale/Modified Tardieu Scale. 2024, from https://www.sralab.org/rehabilitation-measures/tardieu-scalemodified-tardieu-scale
- Amazon.com. Professional cupping therapy set with extension tube. Available at: https://www.amazon.com/Professional-Cupping-Extension-Choi-Corp/dp/B003D19U0O. 2024.
- Siddiqui SA, Shoaib M, Sultana A. Exploring hijama (cupping therapy) for sciatica relief: an integrative review of unani practices. Journal of Drug Delivery and Therapeutics. 2024; 14: 116-119.
- Rehman WU, Maroof L, Khan MH, Israr M, Shah Q, Rehman U, et al. Effect of cupping therapy on biochemical and hematological parameters. National Journal of Life and Health Sciences. 2023; 2: 76-80.
- Borstad A, Schmalbrock P, Choi S, Nichols‐Larsen DS. Neural correlates supporting sensory discrimination after left hemisphere stroke. Brain Research. 2012; 1460: 78-87.
- Yoon HS, Cha YJ, Sohn MK, You JSH. Effect of rehabilitation on the somatosensory evoked potentials and gait performance of hemiparetic stroke patients. Technology and health care: official journal of the European Society for Engineering and Medicine. 2018; 26: 145–150.
- Academy of Neurologic Physical Therapy. 6-minute walk test pocket guide. 2019.
- Ahn SN. Participation based intervention with acquired brain injury: Systematic review and meta-analysis. Restor Neurol Neurosci. 2020; 38: 419-429.
- Jarl Gustav, Ramstrand Nerrolyn. A model to facilitate implementation of the International Classification of Functioning, Disability and Health into prosthetics and orthotics. Prosthetics and Orthotics International. 2018; 42: 468-475.
- Gothe NP, Mullen SP, Wójcicki TR, Mailey EL, White SM, Olson EA, et al. Trajectories of change in self-esteem in older adults: exercise intervention effects. Journal of Behavioral Medicine. 2011; 34: 298-306.
- Kim J, Lee B. The effect of mirror therapy on functional recovery of upper extremity after stroke: a randomized pilot study. Journal of Experimental Stroke &Amp; Translational Medicine. 2017: 10.
- Coley C, Kovelman S, Belschner J, Cleary K, Schladen M, Evans SH, et al. Pedbothome: a video game–based robotic ankle device created for home exercise in children with neurological impairments. Pediatric Physical Therapy. 2022; 34: 212-219.
- Sook-Lei Liew, A mit Sethi, Jaclyn Stephens, Michelle Woodbury. Recovery of Function After Acquired Neurological Injury. Am J Occup Ther. 2024; 78: 7802070010.
- Onigbinde Obalolu. The Prevalence of No-Shows and Cancellations Rate in Outpatient Physical Therapy Practice and Its Relationship to Age and Gender. International Journal of Physiotherapy. 2021: 8.
