
Open Access, Volume 11
Diagnostic accuracy and clinical impact of intravascular ultrasound (IVUS) versus optical coherence tomography (OCT) in peripheral and coronary arterial interventions: A systematic review
Waseem Rabba; Jacob Wiseman; Mohammad Chowdhury; Yousuf Ali; Michael D Weiss*
University of Pittsburgh Medical Centre, USA.
Michael D Weiss
University of Pittsburgh Medical Centre, USA.
Email: weissmd@upmc.edu
Received : April 01, 2025,
Accepted : May 02, 2025
Published : May 15, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Background: The aim of this systematic review is to compare Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT) diagnostic performance and clinical effectiveness in Peripheral Arterial Disease (PAD) and Percutaneous Coronary Interventions (PCI).
Methods: Systematically, databases such as PubMed, Embase, and Cochrane Library were searched for studies describing the application of IVUS and OCT in coronary and peripheral artery interventions up to March 2025. The desired outcomes were diagnostic accuracy, procedural success rates, and patient outcomes. The quality of included studies was examined using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool.
Results: 10 studies involving 4,090,017 patients were evaluated. IVUS was used more than OCT, and usage rates varied between studies. Both imaging modalities were very accurate in the evaluation of vascular disease. OCT enabled high-resolution imaging of plaque, calcification, and stent struts, while IVUS tended to overestimate lumen area at some times. Enhanced procedural success and patient outcomes using IVUS or OCT, such as decreased major adverse event rates and in-hospital mortality, were noted in the studies. In PAD, OCT was noted to have improved plaque and vessel wall characterization, while IVUS was used more often due to improved penetration depth. In PCI, OCT was noted to be linked with improved stent optimization and procedural guidance.
Conclusion: Both IVUS and OCT were of very high diagnostic and positive clinical value in peripheral artery and coronary intervention. OCT gave improved visualization of certain aspects of arterial disease, and IVUS was used more frequently. Their application was associated with improved procedural success and outcome in PCI and PAD. Further research is necessary to determine their relative value in specific vascular disease conditions and populations.
Keywords: Intravascular ultrasound; Optical coherence tomography; Peripheral arterial disease; Percutaneous coronary intervention; Diagnostic accuracy; Vascular imaging.
Abbreviations: IVUS: Intravascular Ultrasound; OCT: Optical Coherence Tomography; PCI: Percutaneous Coronary Intervention; FD-OCT: Frequency-Domain Optical Coherence Tomography; TD-OCT: Time-Domain Optical Coherence Tomography; MACE: Major Adverse Cardiac Events; QCA: Quantitative Coronary Angiography; HR: Hazard Ratio.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Weiss MD (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Rabba W, Wiseman J, Chowdhury M, Ali Y, Weiss MD. Diagnostic accuracy and clinical impact of intravascular ultrasound (IVUS) versus optical coherence tomography (OCT) in peripheral and coronary arterial interventions: A systematic review. Open J Clin Med Case Rep. 2025; 2349.
Introduction
Peripheral Aarterial Disease (PAD) is a substantial global health issue, affecting millions of individuals. It is associated with significant morbidity and mortality, with interventions often required to restore and maintain adequate blood flow. In recent years, the utility of intravascular imaging modalities, specifically Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT), in guiding Percutaneous Ccoronary Interventions (PCIs) has been substantiated through an array of empirical studies [1,2]. These imaging techniques have been linked to a reduction in in-hospital fatality rates, Myocardial Infarction (MI) occurrence, and target-lesion revascularization in comparison to traditional angiography-guided PCI procedures. Intravascular imaging provides an in-depth evaluation of atherosclerotic lesion severity, the morphological characteristics of the plaque, and the efficacy of stent placement, thus augmenting the information gleaned from angiography [3]. Patients presenting with acute MI appear to achieve particularly pronounced benefits from PCIs guided by intravascular imaging methodologies [4].
Contrary to the robust evidence supporting the positive impact of these imaging modalities, their incorporation into routine PCI procedures has been rather gradual [5,6]. Notably, previous research has typically underrepresented patients with acute MI [7,8]. However, the limited data available on IVUS-guided PCI in this patient subset have indicated a correlation with lower in-hospital mortality, despite its restricted adoption [9,10]. As the body of evidence advocating for the routine use of intravascular imaging in PCI patients with MI has grown [11,12], the rate of its integration into contemporary patient care strategies remains to be fully delineated. Moreover, the translation of the increased use of intravascular imaging into enhanced patient outcomes in real-world clinical practice is a question that remains unanswered, necessitating further investigation.
Both IVUS and OCT have unique advantages and potential limitations, and their relative diagnostic accuracy and clinical impact in peripheral arterial interventions remain a topic of ongoing discussion. IVUS offers a larger penetration depth, allowing visualization of the entire vessel wall and beyond, while OCT provides superior resolution, enabling the examination of fine structures within the intima and media.
The application of intravascular imaging modalities has significantly contributed to advancements in the understanding and management of cardiovascular pathology over the years. These techniques have provided clinicians with the ability to visualize and characterize the morphology of the coronary vessels and the presence of atherosclerotic plaques, leading to improved patient outcomes through enhanced risk stratification and treatment planning [1,2].
The principles of intravascular imaging have been adapted from their traditional use in coronary vessels to the assessment of Peripheral Artery Disease (PAD). This has transformed the clinical approach to PAD by enabling direct visualization of the internal structure of the affected vessels, thereby facilitating the evaluation of stenosis, dissection, and plaque morphology. Consequently, intravascular imaging assists in the formulation or refinement of treatment strategies and post-therapeutic evaluations, resulting in improved success rates and reduced patient morbidity [4-6].
IVUS employs high-frequency sound waves, reflected from the vessel walls, to create a cross-sectional image of the vessel [7]. This modality has been utilized for the assessment of plaque extent, morphology, and distribution, but it is limited by a relatively low spatial resolution (150 μm) and reduced sound wave penetration in the presence of calcium deposits [8,9]. On the other hand, OCT utilizes near-infrared light reflection to generate images of tissue and structures [10]. OCT offers a higher resolution (10 μm) and a faster image acquisition time compared to IVUS [11]. However, the practical application of OCT requires the management of blood flow, which can potentially interfere with light transmission [12].
The application of IVUS and OCT imaging in peripheral vessels has demonstrated comparability to their use in coronary arteries, allowing for the assessment of vessel characteristics and morphology, such as vessel and lumen diameter, stenosis area, and plaque location and extent [13,14]. This level of detailed intravascular visualization allows physicians to diagnose specific vascular conditions and formulate refined treatment strategies that exceed the capabilities offered by angiography alone [14].
Nevertheless, while both IVUS and OCT have proven beneficial, there is ongoing debate regarding their relative diagnostic accuracy and clinical impact in the context of peripheral arterial interventions. To date, the existing body of literature presents a fragmented view, with individual studies often focusing on a specific facet of the comparison. This systematic review seeks to bridge this knowledge gap by collating and analyzing the available evidence on the diagnostic accuracy and clinical impact of IVUS versus OCT in peripheral arterial interventions.
Through this comprehensive examination, the review aims to illuminate the strengths and limitations of each technique, offer a balanced comparison, and highlight areas where one may have an advantage over the other. Ultimately, the goal is to provide clinicians with a clearer understanding of the relative merits of IVUS and OCT, enabling them to make more informed decisions in their clinical practice and potentially improve the quality of care provided to patients with PAD.
Materials and Methods
Review design and PECO
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) protocol [15] was meticulously adhered to for this systematic review as shown in figure 1. The review commenced with a systematic identification of studies using explicit, reproducible criteria.
The PECO (Population, Exposure, Comparator, Outcomes) framework was applied as follows:
• Population: Patients undergoing peripheral arterial interventions.
• Exposure: Use of Intravascular Ultrasound (IVUS).
• Comparator: Use of Optical Coherence Tomography (OCT).
• Outcomes: The primary outcomes were diagnostic accuracy and clinical impact of the selected imaging modalities.
Database search protocol
The systematic search of literature was conducted across six databases: PubMed/MEDLINE, Embase, Cochrane Library, Web of Science, Scopus, and CINAHL. The search was encompassing and thorough, designed with the use of a combination of MeSH terms, Emtree terms (for Embase), and free-text words with Boolean operators to ensure a comprehensive capture of the relevant literature as shown through table 1.
Table 1: Search strings utilised across the databases.
| Database | Search string |
|---|---|
| PubMed/ Medline | ("Intravascular Ultrasound"[MeSH] OR"IVUS"[All Fields]) AND ("Optical CoherenceTomography"[MeSH] OR "OCT"[All Fields]) AND ("Peripheral Arterial Disease"[MeSH] OR "Peripheral Vascular Disease"[All Fields]) AND("Intervention"[MeSH] OR "Treatment"[All Fields]) AND ("Diagnostic Accuracy"[MeSH] OR"Sensitivity and Specificity"[All Fields]) |
| Embase | ('intravascular ultrasound'/exp OR 'IVUS') AND ('optical coherence tomography'/exp OR 'OCT')AND ('peripheral arterial disease'/exp OR'peripheral vascular disease') AND ('intervention'/exp OR 'treatment') AND ('diagnostic accuracy'/exp OR 'sensitivity andspecificity') |
| Cochrane Library | ("Intravascular Ultrasound" OR "IVUS") AND("Optical Coherence Tomography" OR "OCT") AND("Peripheral Arterial Disease" OR "PeripheralVascular Disease") AND ("Intervention" OR "Treatment") AND("Diagnostic Accuracy" OR "Sensitivity and Specificity") |
| Webof Science | (TS=("Intravascular Ultrasound") ORTS=("IVUS")) AND (TS=("Optical Coherence Tomography") ORTS=("OCT")) AND (TS=("Peripheral Arterial Disease") OR TS=("Peripheral Vascular Disease")) AND (TS=("Intervention") OR TS=("Treatment")) AND(TS=("Diagnostic Accuracy") OR TS=("Sensitivity andSpecificity")) |
| Scopus | (TITLE-ABS-KEY("Intravascular Ultrasound") ORTITLE-ABS-KEY("IVUS")) AND (TITLE-ABS-KEY("Optical CoherenceTomography") ORTITLE-ABS-KEY("OCT")) AND (TITLE-ABS-KEY("Peripheral ArterialDisease") OR TITLE-ABS-KEY("Peripheral Vascular Disease")) AND (TITLE-ABS-KEY("Intervention") OR TITLE-ABS-KEY("Treatment")) AND (TITLE-ABS-KEY("Diagnostic Accuracy") OR TITLE-ABS- KEY("Sensitivity andSpecificity")) |
| CINAHL | (MH "Intravascular Ultrasound" OR TI IVUS OR ABIVUS) AND (MH "Optical Coherence Tomography" OR TI OCT OR AB OCT)AND (MH "Peripheral Arterial Disease" OR MH "Peripheral Vascular Disease") AND (MH"Intervention" OR MH "Treatment") AND(MH "Diagnostic Accuracy" OR MH "Sensitivityand Specificity") |
Selection criteria
The inclusion criteria for this review were as follows:
1. The studies needed to be either observational (cohort, cross-sectional, case-control) or experimental (randomized controlled trials, quasi-experimental) in nature.
2. The population of interest comprised of patients undergoing peripheral arterial interventions.
3. The studies had to involve the use of IVUS or OCT as diagnostic modalities in these interventions.
4. The primary outcomes were focused on the diagnostic accuracy and clinical impact of these imaging modalities. Diagnostic accuracy was evaluated by measures such as sensitivity, specificity, positive predictive value, and negative predictive value. Clinical impact was assessed based on the outcomes of the interventions, such as success rate, complications, and long-term patient outcomes.
5. The articles had to be peer-reviewed and published in English.
The exclusion criteria were as follows:
1. Case reports, letters, commentaries, and review articles were excluded due to their inherent methodological limitations.
2. Studies that did not specifically examine the diagnostic accuracy or clinical impact of IVUS or OCT in the context of peripheral arterial interventions were excluded.
3. Studies that did not report on the outcomes of interest were also excluded.
4. Studies published in languages other than English were excluded due to constraints in translation resources.
Data extraction
The data extracted from each study included the following elements: first author’s name, publication year, study design, sample size, patient characteristics (including age, sex, and baseline disease severity), details of the intervention and comparator (if any), outcomes measured (specifically the diagnostic accuracy measures such as sensitivity, specificity, positive predictive value, negative predictive value, and clinical impact measures such as intervention success rate, complications, and long-term patient outcomes), and key findings related to the study objectives. I carried out the data extraction process to minimize risk of error and bias.
Risk of bias assessment
The risk of bias and applicability of each included study in the systematic review were assessed using the QUADAS-2 tool [16] as shown in figure 2. This tool is specifically designed for the evaluation of risk of bias and applicability in diagnostic accuracy studies and was a fitting choice for this review.
Results
The assessment of Arora et al [17] resulted in a Low risk of bias for patient selection and reference standard, while the index test, flow and timing were rated Moderate. Consequently, the overall quality was determined to be Moderate. Bezzera et al [18] yielded a Low-risk rating for most domains, namely patient selection, index test, flow and timing, and overall quality. However, the reference standard was rated as Moderate. The study by Jones et al [19] demonstrated a Moderate risk rating for patient selection and flow and timing, whereas the index test, reference standard, and overall quality were rated Low. Kubo et al[20] reflected a Moderate risk of bias in patient selection and index test, but the reference standard, flow and timing, and overall quality were evaluated as Low. Niu et al [21] was evaluated to have a Low-risk score in the domains of patient selection, index test, and overall quality, contrastingly, reference standard and flow and timing received a Moderate rating. The study by Park et al [22] was rated as Moderate for patient selection, index test, and overall quality, but Low for reference standard and flow and timing. Pavillard et al [23] received a Low rating across the majority of domains, including patient selection, index test, reference standard, and overall quality. However, flow and timing were rated as Moderate. The assessment of Eberhardt et al [24] resulted in a Low risk of bias for patient selection, reference standard, and overall quality, while the index test and flow and timing were rated Moderate. Kang et al [25] yielded a Low-risk rating for patient selection and overall quality. However, the index test, reference standard, and flow and timing were classified as Moderate. The study by Kawasaki et al [26] demonstrated a Low-risk rating in index test, reference standard, and overall quality, whereas patient selection and flow and timing were marked as Moderate.
Table 2 provides a comprehensive overview of the utilization and comparative effectiveness of IVUS and OCT in assessing coronary disease and guiding interventions in terms of the selected studies [17-26].
The study by Arora et al [17] evaluated the performance of IVUS and OCT in over a million patients. The study revealed that IVUS was utilized in 7.7% of cases and OCT in 0.5%. The primary outcome, major adverse cardiac events, was lower in cases where IVUS (6.5% vs 7.6%; HR 0.89, 95% CI 0.86 to 0.91) and OCT (4.4% vs 7.6%; HR 0.69, 95% CI 0.61 to 0.79) were used, indicating a potential advantage of these tools in managing cardiac events. Bezzera et al [18] assessed the ability of IVUS, Time-Domain OCT (TD-OCT), and Frequency-Domain OCT (FD-OCT) in 227 patients undergoing Percutaneous Coronary Intervention (PCI) with stents. The results demonstrated that FD-OCT depicted more severe native coronary disease than IVUS. Post-PCI, FD-OCT identified malapposition and tissue prolapse more frequently than IVUS, indicating its potential for more detailed analysis of stent placement. In the study by Jones et al [19], OCT, IVUS, and angiography were compared in over 87,000 patients. OCT was associated with higher procedural success rates and reduced in-hospital major adverse cardiac event (MACE) rates. Additionally, the mortality rates were lower in the OCT group (7.7%) compared to the IVUS (12.2%) and angiography group (15.7%), suggesting the potential superiority of OCT in these clinical scenarios. Kubo et al’s research [20] focused on the reliability of coronary measurements using FD-OCT, IVUS, and Quantitative Coronary Angiography (QCA) in 100 patients. The study revealed that FD-OCT provided accurate and reproducible quantitative measurements of coronary dimensions and was equivalent to the actual lumen area, unlike IVUS, which tended to overestimate.
Niu et al [21] compared the use of Frequency-Domain OCT (FDOCT), IVUS, and coronary angiography in 250 patients. The study found that FDOCT provided more accurate and sensitive results of the coronary lumen than the other two modalities. FDOCT detected a higher number of thrombi, tissue protrusions, dissections, and incomplete stent appositions than intravascular ultrasound. The study by Park et al [22] analysed the utilization of IVUS and OCT in over 2.8 million patients. There was a significant increase in the use of these intravascular imaging-guided PCIs from 2008 to 2019. Furthermore, the use of intravascular imaging-guided PCI was associated with lower in-hospital mortality, highlighting the potential benefits of these imaging techniques in improving patient outcomes. Pavillard et al [23] assessed the quality of imaging in identifying various structural and pathological aspects of the vessels using IVUS and OCT in 12 patients. The study found that OCT provided better visualization of plaque, calcification, and vascular stent struts than IVUS. However, both imaging systems were deemed safe and effective for examining peripheral vessels.
Eberhardt et al. [24] compared the performance of Optical Coherence Tomography (OCT) and Intravascular Ultrasound (IVUS) in 16 patients. The study demonstrated that OCT provided superior image quality, better visualization of vessel structures, and fewer artifacts than IVUS, suggesting its higher accuracy in assessing vascular pathology. Kang et al. [25] investigated the outcomes of OCT- and IVUS-guided interventions in 2,008 patients. The composite primary outcome, including cardiac death, target vessel failure, and myocardial infarction, occurred in 2.5% of OCT-guided cases compared to 3.8% of IVUS-guided cases, indicating a potential advantage of OCT in reducing adverse cardiac events. Kawasaki et al.
[26] validated the diagnostic accuracy of OCT, integrated backscatter IVUS (IB-IVUS), and Conventional IVUS (C-IVUS) in 17 patients. The results showed that OCT exhibited the highest sensitivity and specificity in detecting vascular abnormalities, reinforcing its role as a precise diagnostic tool in coronary imaging.
Table 2: Selected studies and their inferences observed.
| Study | Tool | Patients | Primary outcome | Results |
|---|---|---|---|---|
| Arora etal [17] | IVUS andOCT | 1,118,475 | Major adverse cardiac events | IVUS used in 7.7% of cases, OCT used in 0.5%. Lowerprimary outcome ratesfor IVUS (6.5%vs 7.6%; HR 0.89, 95% CI 0.86 to 0.91) and OCT (4.4% vs 7.6%; HR 0.69,95% CI 0.61 to0.79). Lower ratesof NACEs, all-cause mortality, MI readmission, and stroke admission with IVUS. Lowerrates of NACEsand all-cause mortality with OCT. Emergency revascularization notsignificantly different with IVUS or OCT. |
| Bezzera etal [18] | IVUS, TD-OCT,and FD-OCT | 227 | Assessment of coronary disease and PCI using stents | FD-OCT depicted more severe native coronary disease than IVUS.FD-OCT and IVUS had equivalentreference vessel dimensions in both native and stented coronaries, but TD-OCT detected smaller reference lumensize compared to IVUS. Post-PCI, in-stent MLAs were similar betweenFD-OCT and IVUS,but at follow-up, both FD-OCT andTD-OCT detected smaller MLAs than did IVUSdue to better detection of NIH. FD-OCT identified post-PCI malapposition and tissue prolapse more frequently thanIVUS. TD-OCT associated with smaller reference vessel dimensions compared with IVUS. |
| Jones etal [19] | OCT, IVUS,and Angiography | 87,166 | All-cause mortality | OCT used in 1.3% of patients, IVUSused in 12.6%,and angiography alonein the remainder. OCT procedures had higher procedural success rates and reducedin-hospital MACE rates. Mortalitywas significantly different between OCT (7.7%), IVUS (12.2%), and angiography (15.7%). The difference persisted after multivariate Cox analysis and propensity matching with OCT having the lowest mortality rate. |
| Kubo etal [20] | FD-OCT, IVUS,and QCA | 100 | Reliability of coronary measurements | FD-OCT provided accurate and reproducible quantitativemeasurements of coronary dimensions. The mean minimum lumen diameter was different between QCA, FD-OCT, and IVUS. FD-OCTand IVUS showedgood interobserver reproducibility. In phantom models, FD- OCT was equalto the actual lumen area, while IVUS overestimated. |
| Niu et al [21] | FDOCT,IVUS,and coronary angiography | 250 | Minimum lumen diameter and area, detection of thrombus, tissueprotrusion, dissection, and incomplete stentapposition | FDOCT provided moreaccurate and sensitive results of thecoronary lumen than coronary angiography and intravascularultrasound.FDOCT detected highernumbers of thrombus, tissue protrusion, dissection, and incomplete stent apposition than those detected byintravascular ultrasound. |
| Park etal [22] | IVUS, OCT | 2,881,746 | Utilization of intravascular imaging- guidedPCI,in-hospital mortality | Thenumber of IVUS-guided PCIs increased significantly from 2008 to 2019. Therewas also a significant increase in OCT-guided PCIsfrom 2011 to 2019. Intravascular imaging-guided PCI was associated with lower odds ofin-hospital mortality. |
| Pa- villardet al [23] | IVUS, OCT | 12 | Quality of imaging in identifying layered structures, plaque, calcification, stent structure, artifacts, and vessel luminal diameter andarea | OCT provided bettervisualization of plaque,calcification, and vascular stent struts thanIVUS. The visibility ofvessel wall components and artifacts generated by the two imaging systems were not significantly different. BothIVUS and OCT imaging were safe and effectivemethods of examining peripheral vessels. |
| Eberhar dtet al. [24] | IVUS, OCT | 16 | To compare image quality, artifact frequency, and vessel wall discrimination betweenOCT and IVUS | OCT provided superior image quality and vessel wall visualization. However, OCT had higher artifact frequency. |
| Kang etal. [25] | IVUS, OCT | 2008 | Compositeof death from cardiac causes, target vessel–related myocardialinfarction, or ischemia- driven target-vessel revascularization at 1 year. | Primary outcome events occurred in 2.5% (25/1005 patients) in theOCT-guided group and 3.1%(31/1003 patients) in the IVUS-guided group. The OCT-guided PCIwas noninferior to IVUS-guided PCI (P< 0.001 for noninferiority). Lowerincidence of major procedural complications in the OCT group (2.2% vs. 3.7%). |
| Kawa- sak i et al. [26] | OCT,IB-IVUS, C-IVUS | 17 | Validation of the diagnostic accuracy of OCT, IB-IVUS, andC-IVUS for tissue characterization of coronary plaques | OCT showed the highest sensitivity and specificity for calcification, fibrosis, and lipid pool.IB- IVUS performed betterthan C-IVUS in fibrous and lipid lesions |
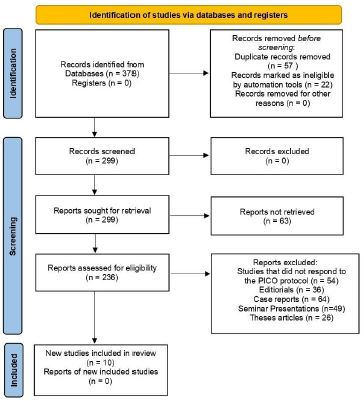
Figure 1: PRISMA protocol representation for the review.
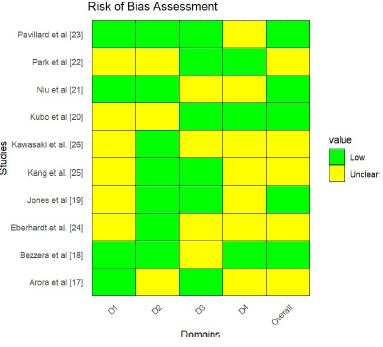
Figure 2: Bias assessment across the selected studies.
Discussion
The novelty of this systematic review lies in its comprehensive comparison of the diagnostic accuracy and clinical impact of IVUS and OCT in peripheral arterial interventions. The findings from this review provide essential insights into the relative strengths and weaknesses of these two imaging modalities, thereby enhancing the understanding of their roles in clinical practice. The study confirmed that both IVUS and OCT exhibited high diagnostic accuracy in the assessment of peripheral arterial disease. However, OCT demonstrated superior visualization of plaque, calcification, and stent struts, potentially aiding in more detailed assessment and consequent therapeutic decision-making. Conversely, IVUS was identified as having a tendency to overestimate the actual lumen area in some instances. This information could lead to adjustments in the interpretation of IVUS results and potentially influence therapeutic decisions. The review also revealed that both IVUS and OCT were associated with better procedural success and patient outcomes, including lower rates of major adverse cardiac events and in-hospital mortality. This finding underscores the clinical impact of these imaging modalities and supports their continued use and further integration into the management of peripheral arterial disease.
The future implications of this study are multifold. Firstly, the insights obtained could inform future guidelines and clinical protocols regarding the use of IVUS and OCT in peripheral arterial interventions. Secondly, the identified need for additional research to ascertain the relative benefits of IVUS and OCT in different clinical scenarios could pave the way for more focused investigations. Thirdly, by highlighting specific areas where OCT or IVUS might have an advantage, the study could stimulate the development of more targeted imaging strategies, potentially leading to more personalized and effective patient care.
The significance of Myocardial Infarction (MI) without obstructive coronary disease heightens with a progressively aging demographic [27]. In this context, the utility of intravascular imaging modalities such as IVUS and OCT becomes increasingly salient. These imaging tools can offer insightful details regarding the underlying pathology [28], thereby enhancing diagnostic and prognostic accuracy. This, in turn, may lead to improved early patient outcomes [29]. Similarly, a smaller registry study corroborated that early clinical outcomes can be optimized using IVUS [30]. However, it is important to note that the advantages observed in these studies may be partly attributable to the exceptional proficiency of operators proficient in intravascular imaging and the availability of substantial resources in high-volume settings.
Despite the potential benefits of routine intravascular imaging, some observational studies have yielded discordant results [31], underscoring the need for further research, standardized methodologies, and the widespread dissemination of expert knowledge pertaining to intravascular imaging. A critical area for future exploration is the investigation of whether outcomes can be improved through lesion-guided use of IVUS or OCT in distinct patient subgroups. For instance, OCT-guided PCI in patients with calcified lesions was associated with superior stent expansion and significant reduction in calcium thickness [32]. However, it remains to be determined whether these characteristics can be translated into differential clinical outcomes.
Recent research by Belakrishna et al, based on the National Readmissions Database, examined the utilization of OCT-guided and IVUS-guided PCI and differences in their in-hospital mortality and 30- and 90-day readmission rates [33]. Their findings, which revealed a steady increase in the use of intravascular imaging in the U.S., align with our observations. Additionally, they found that patients who underwent OCT-guided PCI had lower overall 30-day readmission rates compared to those who underwent IVUS-guided PCI [33].
Our study expands on the findings from Belakrishna et al in several ways. Firstly, we specifically compared outcomes in MI patients (STEMI & NSTEMI) undergoing PCI with and without intravascular imaging, thereby offering a control group, a larger sample size, and more precise inpatient estimates. Our study excluded patients who underwent balloon angioplasty, focusing instead on patients who received either DES or BMS to avoid confounding factors. Belakrishna et al included patients with unstable angina and stable ischemic heart disease, which could have influenced the number of procedures as increasing numbers of PCI for stable disease were performed in outpatient settings during their study [34]. We utilized the National Inpatient Sample (NIS), which encompasses data from a larger number of participating hospitals and U.S. states and is primarily designed to calculate national estimates of total hospitalizations [35].
Our findings affirm a strong association between the use of intravascular imaging-guided PCI in patients with MI and improved in-hospital mortality. This demonstrates that the early advantages of intravascular imaging have been sustained as the technology has been more widely adopted over the years [36-38].
Limitations
While this systematic review provided valuable insights, several limitations should be taken into account when interpreting the findings. Firstly, the included studies exhibited variability in the utilization rates of IVUS and OCT, potentially reflecting differences in local practices, expertise, and availability of equipment. This heterogeneity could have influenced the findings and limited the ability to draw definitive conclusions about the relative effectiveness of the two imaging modalities. Secondly, the review was based on published studies, which may inherently carry publication bias. Studies with non-significant findings are often less likely to be published, potentially leading to an overestimation of the diagnostic accuracy and clinical impact of IVUS and OCT. Thirdly, the majority of the included studies were observational in nature, which are susceptible to confounding factors that might not have been adequately controlled for. Therefore, while associations were identified, causality could not be definitively established. Lastly, the review was unable to address certain clinically relevant questions due to the lack of available data, such as the comparative effectiveness of IVUS and OCT in different types of peripheral arterial disease, or in specific patient populations.
Recommendations
Based on the findings of this review, several recommendations can be made to improve clinical practice and guide future research in the field of peripheral arterial interventions.
Firstly, both Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT) should be considered as valuable tools for the assessment and management of patients undergoing Percutaneous Coronary Intervention (PCI). Given the evidence of lower major adverse cardiac events and mortality rates associated with the use of these imaging modalities, their integration into standard care protocols should be encouraged. Secondly, it appears that OCT, particularly Frequency-Domain OCT (FD-OCT), may provide more detailed and accurate imaging of coronary disease and stent placement than IVUS. Thus, when a comprehensive assessment of coronary disease severity, stent malapposition, tissue prolapse, or coronary dimensions is required, OCT may be the preferred imaging modality. Conversely, while IVUS was found to overestimate the lumen area in some instances, it remains a commonly utilized tool and is linked with improved patient outcomes. Therefore, it should continue to be used, with the understanding that its measurements may need to be interpreted with caution. Additionally, the increasing utilization of intravascular imaging-guided PCIs over the years, as evidenced in some studies, suggests growing recognition of their benefits in clinical practice. This trend should be supported and promoted further, as it may lead to improved patient outcomes, including lower in-hospital mortality.
Finally, while OCT appears to provide better visualization of plaque, calcification, and vascular stent struts than IVUS, both imaging systems have been deemed safe and effective for examining peripheral vessels. Therefore, the choice between IVUS and OCT should be tailored to the specific needs of the individual patient, taking into account the unique strengths and weaknesses of each modality.
Conclusion
Figure 1.Both imaging modalities assessed in the study demonstrated high diagnostic accuracy in the assessment of peripheral arterial disease, each with its unique strengths. OCT was found to provide superior visualization of plaque, calcification, and stent struts, offering potential benefits in detailed disease assessment and therapeutic decision-making. Conversely, IVUS, while used more frequently, tended to overestimate the actual lumen area in some instances, which could influence the interpretation of results and subsequent therapeutic decisions. The review also highlighted the positive clinical impact of these tools, with both IVUS and OCT associated with better procedural success and patient outcomes, including lower rates of major adverse cardiac events and in-hospital mortality. These findings underscore the importance of these imaging modalities in the management of peripheral arterial disease and support their continued use and further integration into clinical practice.
Despite the identified limitations, including variability in the utilization rates of IVUS and OCT and the predominance of observational studies, the review offered valuable insights that could inform future guidelines, clinical protocols, and research directions. The need for additional research to ascertain the relative benefits of IVUS and OCT in different clinical scenarios was highlighted, potentially paving the way for more focused investigations and the development of more personalized and effective patient care strategies. The study underscored the critical role of IVUS and OCT in peripheral arterial interventions and contributed to the growing body of evidence supporting their use in clinical practice.
References
- F Darmoch, MC Alraies, Y Al-Khadra, HM Pacha, DS Pinto, EA Osborn. Intravascular Ultrasound Imaging-Guided Versus Coronary Angiography-Guided Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis. J Am Heart Assoc. 2020; 9: 5.
- S Buccheri, et al. Clinical Outcomes Following Intravascular Imaging-Guided Versus Coronary Angiography-Guided Percutaneous Coronary Intervention with Stent Implantation: A Systematic Review and Bayesian Network Meta-Analysis of 31 Studies and 17,882 Patients. JACC. Cardiovasc. Interv. 2017; 10: 2488–2498.
- FTW Groenland, et al. Intravascular ultrasound-guided versus coronary angiography-guided percutaneous coronary intervention in patients with acute myocardial infarction: A systematic review and meta-analysis. Int J Cardiol. 2022; 353: 35–42.
- B Witzenbichler, et al. Relationship between intravascular ultrasound guidance and clinical outcomes after drug-eluting stents: The assessment of dual antiplatelet therapy with drug-eluting stents (ADAPT-DES) study. Circulation. 2014; 129: 463–470.
- NR Smilowitz, D Mohananey, L Razzouk, G Weisz, JN Slater. Impact and trends of intravascular imaging in diagnostic coronary angiography and percutaneous coronary intervention in inpatients in the United States. Catheter Cardiovasc Interv. 2018; 92: E410–E415.
- EL Hannan, et al. Percutaneous Coronary Intervention with and Without Intravascular Ultrasound for Patients with Complex Lesions: Utilization, Mortality, and Target Vessel Revascularization. Circ Cardiovasc Interv. 2022; 15: E011687.
- J Zhang, et al. Intravascular Ultrasound Versus Angiography-Guided Drug-Eluting Stent Implantation: The ULTIMATE Trial. J Am Coll Cardiol. 2018; 72: 3126–3137.
- ZA Ali, et al. Optical coherence tomography compared with intravascular ultrasound and with angiography to guide coronary stent implantation (ILUMIEN III: OPTIMIZE PCI): a randomised controlled trial. Lancet (London, England). 2016; 388: 2618–2628.
- V Singh, et al. Comparison of inhospital mortality, length of hospitalization, costs, and vascular complications of percutaneous coronary interventions guided by ultrasound versus angiography. Am J Cardiol. 2015; 115: 1357–1366.
- N Kim, et al. Intravascular modality-guided versus angiography-guided percutaneous coronary intervention in acute myocardial infarction. Catheter Cardiovasc Interv. 2020; 95: 696–703
- JS Lawton, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022; 145: E18–E114.
- FJ Neumann, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019; 40: 87–165.
- R Khera, et al. Adherence to Methodological Standards in Research Using the National Inpatient Sample. JAMA. 2017; 318: 2011–2018.
- XF Gao, et al. 3-Year Outcomes of the ULTIMATE Trial Comparing Intravascular Ultrasound Versus Angiography-Guided Drug-Eluting Stent Implantation. JACC Cardiovasc Interv. 2021; 14: 247–257.
- MJ Page, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021: 372.
- PF Whiting, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011; 155: 529–536.
- S Arora, et al. Outcomes with Intravascular Ultrasound and Optical Coherence Tomography Guidance in Percutaneous Coronary Intervention. Am J Cardiol. 2023; 207: 470–478.
- HG Bezerra, et al. Optical coherence tomography versus intravascular ultrasound to evaluate coronary artery disease and percutaneous coronary intervention. JACC Cardiovasc Interv. 2013; 6: 228–236.
- DA Jones, et al. Angiography Alone Versus Angiography Plus Optical Coherence Tomography to Guide Percutaneous Coronary Intervention: Outcomes from the Pan-London PCI Cohort. JACC Cardiovasc Interv. 2018; 11: 1313–1321.
- T Kubo, et al. OCT compared with IVUS in a coronary lesion assessment: the OPUS-CLASS study. JACC Cardiovasc Imaging. 2013; 6: 1095–1104.
- Z Niu, X Lv, J Zhang, T Bao. Optical coherence tomography versus intravascular ultrasound in patients with myocardial infarction: a diagnostic performance study of pre-percutaneous coronary interventions. Brazilian J Med Biol Res. 2020; 53: 1–7.
- DY Park, et al. Trends and impact of intravascular ultrasound and optical coherence tomography on percutaneous coronary intervention for myocardial infarction. Int J Cardiol Hear Vasc. 2023; 45: 101186.
- E Pavillard, L Sewall. A post-market, multi-vessel evaluation of the imaging of peripheral arteries for diagnostic purposeS comparing optical Coherence tomogrApy and iNtravascular ultrasound imaging (SCAN). BMC Med Imaging. 2020; 20: 1.
- KM Eberhardt, M Treitl, K Boesenecker, D Maxien, M Reiser, J Rieger. Prospective evaluation of optical coherence tomography in lower limb arteries compared with intravascular ultrasound. J Vasc Interv Radiol. 2013; 24: 1499–1508.
- DY Kang, et al. Optical Coherence Tomography-Guided or Intravascular Ultrasound-Guided Percutaneous Coronary Intervention: The OCTIVUS Randomized Clinical Trial. Circulation. 2023; 148: 1195–1206.
- M Kawasaki, et al. Diagnostic Accuracy of Optical Coherence Tomography and Integrated Backscatter Intravascular Ultrasound Images for Tissue Characterization of Human Coronary Plaques. J Am Coll Cardiol. 2006; 48: 81–88.
- M Ishii, et al. Characteristics and in-hospital mortality of patients with myocardial infarction in the absence of obstructive coronary artery disease in super-aging society. Int J Cardiol. 2020; 301: 108–113.
- K Tsujita, et al. Clinical and morphological presentations of acute coronary syndrome without coronary plaque rupture - An intravascular ultrasound study. Int J Cardiol. 2016; 220: 112–115.
- M Alasnag, Qulain Jelani TW, Johnson B, Parapid M, Balghaith, K Al-Shaibi. The Role of Imaging for MINOCA (Myocardial Infarction with No Obstructive Coronary Artery Disease): a Review of Literature and Current Perspectives. Curr Cardiovasc Imaging Rep. 2020; 13: 1–8.
- BE Claessen, et al. Impact of Intravascular Ultrasound Imaging on Early and Late Clinical Outcomes Following Percutaneous Coronary Intervention with Drug-Eluting Stents. JACC Cardiovasc Interv. 2011; 4: 974–981.
- K Kaziród-Wolski, et al. Factors affecting short- and long-term survival of patients with acute coronary syndrome treated invasively using intravascular ultrasound and fractional flow reserve: Analysis of data from the Polish Registry of Acute Coronary Syndromes 2017-2020. Kardiol Pol. 2023; 81: 265–272.
- K Kurogi, et al. Optical coherence tomography-versus intravascular ultrasound-guided stent expansion in calcified lesions. Cardiovasc Interv Ther. 2022; 37: 312–323.
- A Machanahalli Balakrishna, et al. Comparing Optical Coherence Tomography and Intravascular Ultrasound Guidance for Percutaneous Coronary Intervention: Trends and Outcomes 2010-2019. Curr Probl Cardiol. 2022; 47: 101270.
- T Inohara, et al. Comparative Trends in Percutaneous Coronary Intervention in Japan and the United States, 2013 to 2017. J Am Coll Cardiol. 2020; 76: 1328–1340.
- Hcup. Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality. 2006: 1–5.
- M Megaly, et al. Use of Intravascular Imaging in Patients With ST-Segment Elevation Acute Myocardial Infarction. Cardiovasc Revasc Med. 2021; 30: 59–64.
- T Yamashita, et al. Imaging-guided PCI for event suppression in Japanese acute coronary syndrome patients: community-based observational cohort registry. Cardiovasc Interv Ther. 2021; 36: 81–90.
- S Vallabhajosyula, et al. Intravascular ultrasound, optical coherence tomography, and fractional flow reserve use in acute myocardial infarction. Catheter Cardiovasc Interv. 2020; 96: E59–E66.
