
Open Access, Volume 11
Ultrasonographic evaluation of thyroid oncocytic follicular carcinoma: A report of two cases with literature review
Siyu Duan Yang1,2; Wenhao Qu1,2; Yanfang Wang2; Fang Nie2*
1The Second Clinical Medical School, Lanzhou University, China.
2Department of Ultrasound Medical Center, The Second Hospital of Lanzhou University, Gansu Province Medical Engineering Research Center for Intelligence Ultrasound, Gansu Province Clinical Research Center for Ultrasonography, China.
Fang Nie
Department of Ultrasound, Lanzhou University Second Hospital, Chengguan District, Lanzhou, Gansu 730000, China.
Tel: 13993163088;
Email: ery_nief@lzu.edu.cn
Received : March 25, 2025,
Accepted : April 17, 2025
Published : April 30, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Oncocytic Follicular Carcinoma (OFC), a rare thyroid malignancy accounting for 1.3–5% of thyroid cancers, requires aggressive surgical and follow-up strategies due to its high invasiveness. This study presents two female cases with preoperative ultrasound demonstrating complex cystic-solid masses lacking classic malignant features (no microcalcifications, regular margins). Postoperative pathology confirmed OFC with capsular invasion, and laboratory tests revealed elevated Thyroglobulin (TG) in both patients. These cases highlight that OFC may masquerade as benign cystic-solid nodules, and combined ultrasonography and TG testing can improve preoperative diagnostic accuracy for this aggressive subtype.
Keywords: Oncocytic thyroid follicular carcinoma; Ultrasound; Follicular carcinoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Fang N (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Siyu Duan Y, Wenhao Q, Yanfang W, Fang N. Ultrasonographic evaluation of thyroid oncocytic follicular carcinoma: A report of two cases with literature review. Open J Clin Med Case Rep. 2025; 2346.
Case Presentations
Case 1
A female in her 50s was admitted to our hospital with a 10-year history of thyroid nodule and 1-year history of progressive dyspnea. The nodule had enlarged significantly over the past year, accompanied by occasional nocturnal dyspnea and dysphagia.
Imaging findings: 2D ultrasound revealed a 6.3 × 5.0 × 2.7 cm mixed-echo mass in the left thyroid lobe, with regular morphology, well-defined margins, heterogeneous echotexture, multiple anechoic areas, and abundant intratumoral vascularity (C-TIRADS 3). Contrast-enhanced neck CT suggested nodular goiter with possible follicular adenoma.
Laboratory results: Thyroid function: Thyroxine: 53.1 nmol/L (normal: 55.4–161.25 nmol/L, mild hypothyroidism); hyroglobulin (TG): >300 ng/mL (normal: 0.83–68 ng/mL, markedly elevated); Vascular endothelial growth factor (VEGF): 229.1 pg/mL (normal: 0–142.2 pg/mL).
Surgical & pathological findings: Total thyroidectomy was performed. Final pathology confirmed left thyroid oncocytic follicular neoplasm. Multifocal capsular invasion was identified on serial sectioning. Immunohistochemistry (CD31 staining for endothelial cells) revealed intraluminal tumor thrombi in vascular spaces, diagnostic of oncocytic follicular carcinoma with vascular invasion.
Case 2
A female in her 60s presented with a 10-month history of thyroid nodules and recent cervical swelling with tenderness.
Imaging findings: Ultrasound revealed multiple mixed-echo nodules in both thyroid lobes: Left lobe: 2.2×1.7 cm (predominantly solid); Right lobe: 2.7×1.9 cm (predominantly solid).
Features: aspect ratio <1, regular shape, well-defined margins, peripheral and intranodular vascularity (C-TIRADS 3). Contrast-enhanced neck CT suggested nodular goiter with multiple adenomas.
Laboratory results: Thyroglobulin (TG): >300 ng/mL (normal: 0.83–68 ng/mL, markedly elevated). Surgical & Pathological Findings: Total thyroidectomy was performed.
Final pathology showed: Left thyroid tumor with thick fibrous capsule and oncocytic cytoplasm. Focal capsular invasion and extrathyroidal tumor nests confirmed oncocytic follicular carcinoma (morphologically consistent with 2022 WHO criteria).
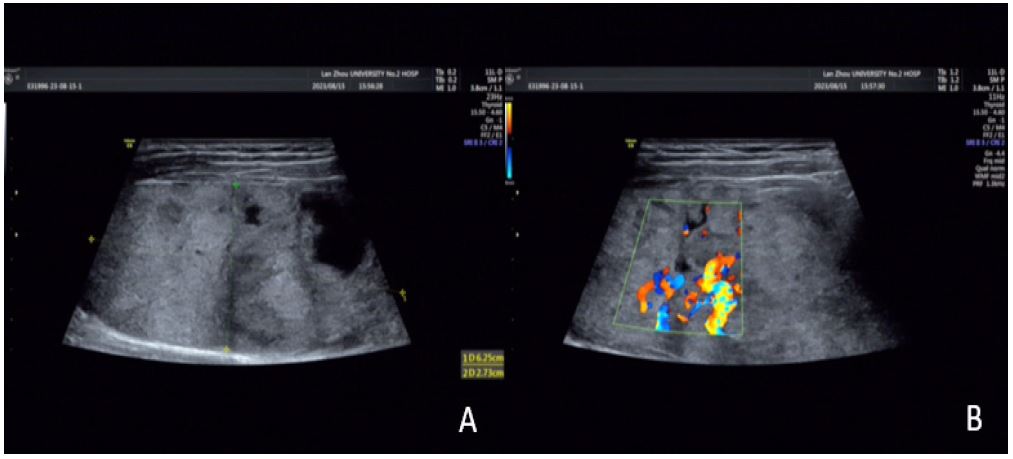
Figure 1: (A) A cystic solid mass of about 6.5 × 5.0 cm in size is seen in the left lobe of the thyroid gland (shown by arrows), with a regular morphology, clear borders, and heterogeneous internal echogenicity, and multiple irregular areas are seen; (B) abundant blood flow signals are seen inside and around the mass (shown by arrows).
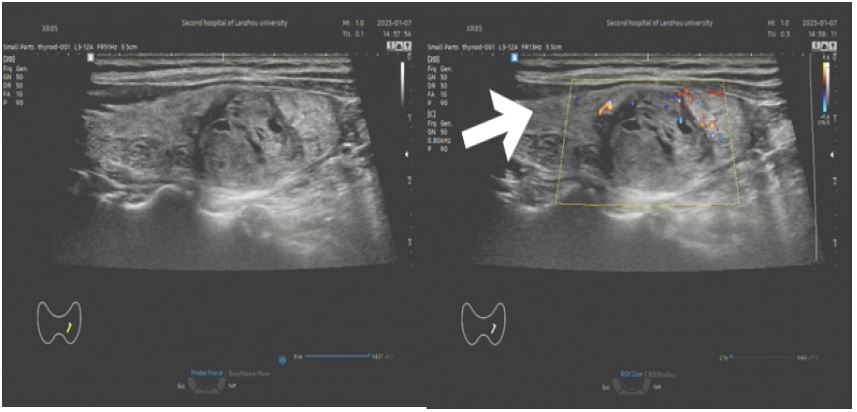
Figure 2: (A) a cystic solid mass of about 2.2 x 1.7 cm in size is seen in the left lobe of the thyroid gland (shown by arrows), with a regular morphology, clear borders, uneven internal echogenicity, and a hypoechoic halo is seen around it; (B) a small amount of short rod-shaped blood flow signals can be seen inside and around the mass (shown by arrows).
Discussion/Conclusion
Thyroid Oncocytic Follicular Carcinoma (OFC), also known as Hürthle cell carcinoma, is a rare malignant thyroid neoplasm, accounting for 1.3%-5% of all thyroid cancers [1]. Notably, the 2022 WHO classification of thyroid tumors has reclassified oncocytic carcinoma as an independent entity, distinct from follicular carcinoma, under the category of follicular-derived malignancies. The term “oncocytic follicular carcinoma” is retained only when the tumor exhibits both oncocytic features and typical follicular architecture [2,3]. OFC is characterized by unique biological behaviors, including higher aggressiveness, increased rates of lymph node metastasis, and a propensity for distant metastasis (with lung and bone metastasis rates of 23%-33%) [4]. These features necessitate more aggressive surgical strategies (e.g., total thyroidectomy with central lymph node dissection) and lifelong follow-up. Currently, systematic reports on the imaging features of OFC are limited. This study aims to elucidate potential patterns in its ultrasound manifestations through two representative cases and a literature review.
Traditional ultrasound features of malignant thyroid nodules (e.g., hypoechogenicity, microcalcifications, and indistinct margins) exhibit low specificity in OFC [5]. In this study, both cases presented preoperatively as mixed cystic-solid masses (average diameter: 3.4 cm) with scattered anechoic areas, well-defined borders, and an absence of typical malignant features. These findings align with the negative correlation between cystic component proportion and malignancy risk. Xin et al. [6] demonstrated that the malignancy risk increases when the solid component exceeds 70% in mixed cystic-solid nodules, consistent with the >80% solid component observed in our cases.
Of particular interest, Zhou et al. [7] identified young age (<45 years), hypoechogenicity, irregular margins, and microcalcifications as independent risk factors for malignancy in their study of 285 mixed cystic-solid nodules. However, in our cases, both patients were >45 years old, and none exhibited these typical malignant features. This suggests that OFC may “masquerade” as benign on ultrasound (e.g., well-defined borders, cystic changes), necessitating a comprehensive evaluation incorporating vascular patterns (both cases exhibited internal blood flow) and clinical features (e.g., elevated thyroglobulin levels).
Thyroglobulin (TG), a specific marker of thyroid follicular cells, demonstrates high sensitivity but low specificity in OFC [8]. In this study, both patients had preoperative TG levels >300 ng/mL (normal reference: 0.83-68 ng/mL), consistent with the reported TG positivity rate in OFC (72%-89%) [8]. Although elevated TG alone cannot confirm malignancy, its dynamic changes are valuable for postoperative monitoring (e.g., recurrence assessment) [9]. Based on our findings, we recommend enhanced ultrasound-guided Fine-Needle Aspiration (FNA) for cystic-solid masses accompanied by elevated TG.
This study highlights two key ultrasound pitfalls in OFC: (1) large cystic-solid masses may be misdiagnosed as benign lesions, and (2) typical malignant features such as microcalcifications and indistinct margins may be absent. In line with recent guidelines, we propose the following recommendations: First, for cystic-solid nodules >3 cm, even with well-defined borders, OFC should be considered. Second, ultrasound evaluation should focus on internal vascular patterns (e.g., penetrating or chaotic blood flow, commonly seen in OFC). Finally, combining TG testing with FNA cytology can improve preoperative diagnostic accuracy.
Declarations
Funding: This study was supported by the Excellent Doctoral Fund Project of the Cuiying Science and Technology Program of the Second Hospital of Lanzhou Universit (Grant number: CY2022-YB-B02) and Science and technology Program Project of Gansu Province (Grant number: 22JR11RA078).
Competing interests: He authors have no relevant financial or non-financial interests to disclose.
Data availability statement: All data generated or analyzed during this study are included in this published article.
References
- Bischoff LA, Ganly I, Fugazzola L, et al. Molecular Alterations and Comprehensive Clinical Management of Oncocytic Thyroid Carcinoma: A Review and Multidisciplinary 2023 Update. JAMA Otolaryngol Head Neck Surg. 2024; 150: 265-272.
- Baloch ZW, Asa SL, Barletta JA, et al. Overview of the 2022 WHO Classification of Thyroid Neoplasms. Endocr Pathol. 2022; 33: 27-63.
- Basolo F, Macerola E, Poma AM, Torregrossa L. The 5th edition of WHO classification of tumors of endocrine organs: changes in the diagnosis of follicular-derived thyroid carcinoma. Endocrine. 2023; 80: 470-476.
- Zhang T, He L, Wang Z, et al. Risk factors for death of follicular thyroid carcinoma: a systematic review and meta-analysis. Endocrine. 2023; 82: 457-466.
- Yu B, Li Y, Yu X, et al. Differentiate Thyroid Follicular Adenoma from Carcinoma with Combined Ultrasound Radiomics Features and Clinical Ultrasound Features. J Digit Imaging. 2022; 35: 1362-1372.
- Xin Y, Liu F, Shi Y, Yan X, Liu L, Zhu J. A Scoring System for Assessing the Risk of Malignant Partially Cystic Thyroid Nodules Based on Ultrasound Features. Front Oncol. 2021; 11: 731779.
- Zhou T, Huang H, Dong H, et al. Ultrasound-Based Risk Stratification System for the Assessment of Partially Cystic Thyroid Nodules. Endocr Pract. 2023; 29: 428-435.
- Yamazaki H, Sugino K, Katoh R, et al. Management of follicular thyroid carcinoma. Eur Thyroid J. 2024; 13: e240146.
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016; 26: 1-133.
