
Open Access, Volume 11
A rare complication of robot assisted total knee replacement – “Spontaneous recurrent hemarthrosis and its management”
Rehman MZ*; Winkworth C; Chivate R; Aslam N
Specialty Doctor, Worcestershire Acute Hospitals, NHS Trust, UK.
M Zain Rehman
FRCS (Tr & Orth), Specialty Doctor, Worcestershire Acute Hospitals, NHS Trust, UK.
Email: m.zain-urrehman@nhs.net
Received : February 27, 2025,
Accepted : April 11, 2025
Published : April 15, 2025,
Archived : www.jclinmedcasereports.com
Keywords: Spontaneous recurrent hemarthroses; Robotic Total knee replacement; Angiography.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Rehman MZ (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Rehman MZ, Winkworth C, Chivate R, Aslam N. A rare complication of robot assisted total knee replacement – “Spontaneous recurrent hemarthrosis and its management”. Open J Clin Med Case Rep. 2025; 2344.
Introduction
Spontaneous Recurrent hematemesis following total knee replacement is a relatively rare complication being reported in up to 1.6% of patients [1]. It requires a diff erent and swift management plan as compared to any other knee swelling. Presentation can vary from 2 months to 1.5 years, [2] and it can lead to further complications including limited range of movement, severe stiff ness resulting in compromised functionality [3,4]. Etiology is not well understood but it can be due to instrumentation leading to direct vessel injury including popliteal and geniculate arteries, arteriovenous fistula and pseudoaneurysms [5,6]. The aim of this case report is to contribute to the early identification and management of the rare complication. We present a case involving the early onset of recurrent spontaneous hemarthrosis following robot-assisted total knee replacement surgery.
Case Report
A 69-year-old male underwent right side robotic assisted total knee replacement for severe grade 4 knee osteoarthrosis in August 2023. His surgery was uneventful and he was discharged home with routine physiotherapy protocol and venous thromboprophylaxis. He was recovering well until 4 weeks after surgery when he presented in the emergency department with acute onset of pain and swelling of the right knee. He was able to weight bear and didn’t have any spike of fever. There wasn’t any history of bleeding disorder and he had already completed his 2 weeks of VTE prophylaxis medications. Clinical examination showed moderate to large diff use swelling around the knee, mildy raised temperature as compared to the other side, no significant erythema or redness. He had a range of motion of the knee from 10-90°. His blood tests for inflammatory markers showed C-Reactive Protein (CRP) 5 mg/dL and White Cell Count (WBC) of 6.8×109/ L. Radiographs of the right knee showed loss of supra and infra patellar fat pad suggestive of gross joint eff usion (Figures 1 & 2). His knee was aspirated with around 100 ml of dark colored frank blood which raised the suspicion of venous bleeding. The cultures were negative. He was sent home with advice of icing and elevation of knee at rest.
As he had recurrent knee swelling, after discussion with the vascular surgeons and interventional radiologists, they advised a lower limb computed tomographic angiogram to see any vascular abnormalities. It showed no large vascular abnormality. However, there was moderate hemarthrosis. The CT images were significantly obscured due to streak artefacts from metallic implants
In view of continued knee joint swelling, the patient underwent right lower limb angiography the following week through the right femoral artery approach which identified a Pseudoaneurysm arising from the inferior medial genicular artery. This was embolized using 250 microns’ particles- embospheres and 2mm push able coils. Selective angiogram performed from superior medial and lateral genicular artery showed abnormal blush and pruning was done using 250-micron embospheres (Figures 3,4 & 5). An Ice pack was placed over the knee while instilling embolic agent particles to cause vasoconstriction of the skin arterial supply to avoid ischemia.
On his 6 months’ follow-up appointment he had fully recovered, was able to perform his daily activities and didn’t have any further episode of swelling.

Figure 1, 2: Post-operative Anteroposterior and lateral radiographs of Knee showing total knee replacement in place and gross joint eff usion in form of loss supra and infra patellar fat pad.
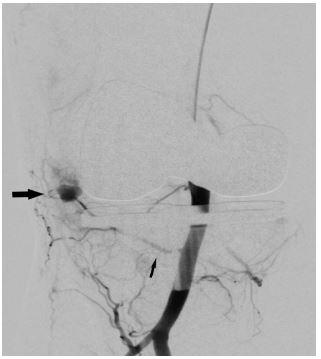
Figure 3: Angiography done through catheter in popliteal artery shows pseudoanuerysm (Solid arrow) arising from inferior medial geniculate artery (thin arrow).

Figure 4: Post-operative Anteroposterior and lateral radiographs of Knee showing total knee replacement in place and gross joint eff usion in form of loss supra and infra patellar fat pad.

Figure 5: Post embolization using particles- embospheres and coils (solid arrow) angiography shows non opacification of the pseudoaneurysm.
Discussion
Recurrent spontaneous hemarthrosis can be difficult to manage if not diagnosed promptly leading to severe limitation of movements and stiff ness of the knee. After ruling out infection a course of conservative treatment is advised, failure of which can lead to appropriate intervention [4]. There are many approaches towards recurrent spontaneous hemarthrosis of the knee after total knee replacement described in the literature including a paper by Saksena [1] which described an algorithmic approach and mentioned to stop all anti-coagulation medications and patient blood tests should be done to rule out any coagulopathies. After icing and resting the knee if a large hemarthrosis persists, it should be aspirated and immobilized.
Angiography by involving Interventional radiologist has been described the first line procedure in diagnosis of such cases [7]. This technique is also useful in ruling out arteriovenous fistulas and pseudoaneurysms [8,9]. Once the diagnosis in confirmed , selective arterial embolization of the geniculate arteries is the procedure of choice which decreases the blood flow to the soft tissues and synovium around the total knee replacement. Weidner [4] described a case series which reported as Geniculate arterial embolization lead to resolution of hemarthrosis in 12 of 13 patients (92.3%). The one clinical failure likely represented a case of misdiagnosed periprosthetic joint infection. In their study, the average interval between arthroplasty and embolization was 47 months (Range 2 to 103 months), and the average time from onset of hemarthrosis to embolization was 4.1 months (Range 1 to 11 months).
In another series of five patients reported by Bagla et al. [3] which presented with spontaneous hematemesis after total knee replacement, selective arterial embolization was performed with spherical embolic particles (diameter range, 100-700 μm). Angiography demonstrated synovial hypervascularity with geniculate artery “tumor blush” appearance in all patients. The average time to resolution of eff usion was 2.6 weeks, with no recurrences reported during follow-up (mean, 25.4 month; range, 16-48 months).
In previous literature, spontaneous recurrent hemarthrosis after total knee replacement has been reported as a late complication [4] but, in our case, it presented quite early i.e. within 4 weeks’ time of surgery. Kindsfater and Scott case series [10] showed the average interval between implantation of the prosthesis and the first bleed to be 24.2 months. Out of thirty, nine knees responded to conservative care alone. The remaining 21 knees continued to have recurrent bleeds requiring surgical intervention. They described the histologic findings including focal synovial hyperplasia and significant hemosiderin deposition.
On the other hand Guevara et al. [11] showed the significance of identifying other cases including blood dyscrasias, as their presence led to repeat embolization and limited clinical success. In a series of eight cases by Dhondt et al. [12] mentioned that angiography revealed hypertrophic vascular synovium in seven patients with an additional false aneurysm in one patient.
After embracing the innovation of robotic assisted total knee replacement around the globe, we should be mindful of spontaneous recurrent hemarthrosis in cases of recurrent swelling. Treatment modalities including conservative management as mentioned above should be trialed, further steps after diagnosis using angiography should be leading to selective arterial embolization, which has showed promising results.
Conclusion
After robotic assisted total knee replacement, in cases of recurrent swelling a high index of suspicion is imperative for the early diagnosis of spontaneous hemarthrosis. After a trial of conservative management, infection and blood coagulopathy should be ruled out. Further steps should be angiography for diagnosis and selective arterial embolization of the geniculate arteries for appropriately selected patients.
References
- Saksena J, Platts AD, Dowd GSE. Recurrent haemarthrosis following total knee replacement. The Knee. 2010; 17: 7–14.
- Worland RL, Jessup DE. Recurrent hemarthrosis after total knee arthroplasty. J Arthroplasty. 1996; 11: 977–8.
- Bagla S, Rholl KS, van Breda A, Sterling KM, van Breda A. Geniculate artery embolization in the management of spontaneous recurrent hemarthrosis of the knee: case series. J Vasc Interv Radiol JVIR. 2013; 24: 439–42.
- Weidner ZD, Hamilton WG, Smirniotopoulos J, Bagla S. Recurrent Hemarthrosis Following Knee Arthroplasty Treated with Arterial Embolization. J Arthroplasty. 2015; 30: 2004–7.
- Purudappa PP, Sharma OP, Ashraf M, Sambandam SN. Spontaneous Recurrent Hemarthrosis Post Total Knee Arthroplasty Treated with Selective Embolization – A Case Report and Review of Literature. J Orthop Case Rep. 2020; 10: 22–5.
- Rand JA. Vascular complications of total knee arthroplasty. Report of three cases. J Arthroplasty. 1987; 2: 89–93.
- Saksena J, Platts AD, Dowd GSE. Recurrent haemarthrosis following total knee replacement. The Knee. 2010; 17: 7–14.
- Ibrahim M, Booth RE, Clark TWI. Embolization of traumatic pseudoaneurysms after total knee arthroplasty. J Arthroplasty. 2004; 19: 123–8.
- Haddad FS, Prendergast CM, Dorrell JH, Platts AD. Arteriovenous fistula after fibular osteotomy leading to recurrent haemarthroses in a total knee replacement. J Bone Joint Surg Br. 1996; 78: 458–60.
- Kindsfater K, Scott R. Recurrent hemarthrosis after total knee arthroplasty. J Arthroplasty. 1995; 10: S52-55.
- Guevara CJ, Lee KA, Barrack R, Darcy MD. Technically Successful Geniculate Artery Embolization Does Not Equate Clinical Success for Treatment of Recurrent Knee Hemarthrosis after Knee Surgery. J Vasc Interv Radiol JVIR. 2016; 27: 383–7.
- Dhondt E, Vanhoenacker FM, D’ Archambeau O, Snoeckx A, Defreyne L. Angiographic findings and therapeutic embolization of late hemarthrosis after total joint arthroplasty. Skeletal Radiol. 2009; 38: 31–6.
- Saksena J, Platts AD, Dowd GSE. Recurrent haemarthrosis following total knee replacement. The Knee. 2010; 17: 7–14.
- Purudappa PP, Sharma OP, Ashraf M, Sambandam SN. Spontaneous Recurrent Hemarthrosis Post Total Knee Arthroplasty Treated with Selective Embolization – A Case Report and Review of Literature. J Orthop Case Rep. 2020; 10: 22–5.
- Rand JA. Vascular complications of total knee arthroplasty. Report of three cases. J Arthroplasty. 1987; 2: 89–93.
- Kindsfater K, Scott R. Recurrent hemarthrosis after total knee arthroplasty. J Arthroplasty. 1995; 10: S52-55.
- Guevara CJ, Lee KA, Barrack R, Darcy MD. Technically Successful Geniculate Artery Embolization Does Not Equate Clinical Success for Treatment of Recurrent Knee Hemarthrosis after Knee Surgery. J Vasc Interv Radiol JVIR. 2016; 27: 383–7.
