
Open Access, Volume 11
Prevalence of low back pain in the National Institute of Cancer
Grezzia Isareyda Avellaneda Peralta1*; María del Rocio Guillén Núñez2; Angel Manuel Juárez Lemus2; Ana Karen Castillo Desaida1; Mirtha Nayeli Pola Méndez1; César Roberto Candia Bobadilla3
1Anesthesiologist, Algologist, National Institute of Cancer, Mexico.
2Anesthesiologist, Interventional Pain Physician, National Institute of Cancer, Mexico.
3Anesthesiologist, National Institute of Cancer, Mexico.
Grezzia Isareyda Avellaneda Peralta
Anesthesiologist, Algologist, National Institute of Cancer, 22 San Fernando Ave, Section XVI, Tlalpan 14080 CDMX, Mexico.
Tel: 4431080136; Email: grezziavellaneda@gmail.com
Received : March 19, 2025,
Accepted : April 11, 2025
Published : April 15, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Background: The United Nations has recognized that low back pain is a common condition experienced by most people and it is the leading cause of disability around the world. It generates substantial cost that impact the economy. The prevalence can range from 10 to 80%, depending on the population studied.
Objective: To identify the prevalence of low back pain in cancer patients treated by the Pain Medicine Department of the National Cancer Institute in Mexico in the period from January 1, 2022 to December 31, 2023.
Materials and methods: It is an observational, descriptive, cross-sectional and retrospective study; that copilates records from 01-01-2022 to 31-12-2023; it included demographic variables, risk factors, type of cancer, stage of the cancer, etiology lumbar pain, presence of radicular pain, pain intensity scales and performance status scales, treatment approach to manage low back pain, opioid prescription, performance of percutaneous procedures to manage pain; the analysis was carried out using the SPSS statistical program version 25, through descriptive statistics, presenting frequencies, proportions, measures of central tendency and dispersion.
Results: During this period, a total of 4,253 files of patient’s records were reviewed, only 977 patients’ files met the inclusion criteria. A amount of 658 were women and 319 were male; 797 patients manage lumbar pain with an opioid prescription, 151 with non-opioid medication and 29 with non-pharmacological management. The leading oncological disorders were breast cancer (219 patients) and prostate/urogenital cancer (169 patients).
Conclusion: This study has found that the prevalence of low back pain in the Pain Medicine Department of the National Cancer Institute is 11.64%.
Keywords: Low back pain; Cancer; Prevalence.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Avellaneda Peralta GI (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Avellaneda Peralta GI, Guillén Núñez MR, Juárez Lemus AM, Castillo Desaida AK, Pola Méndez MN, Candia Bobadilla CR. Prevalence of low back pain in the National Institute of Cancer. Open J Clin Med Case Rep. 2025; 2343.
Introduction
According to the World Health Organization (WHO), about 20 million new cases of cancer were diagnosed in 2022, which represents a high incidence worldwide [1]. Regarding low back pain, the WHO mentions that in 2020 it affected 619 million people worldwide (10% of the world’s population) [2]. Also, it is worth mentioning that “it is the main cause of disability” [2]. The Global Burden of Disease (GBD) Study estimates that both disability and disease-related costs will increase in the following decades [3]. In 2019, the Mexican Ministry of Health considered low back pain as the second most common cause of medical consultation, with a prevalence of up to 60% in older adults [4]. The National Institute of Social Security (IMSS) also reports that more than 300,000 consultations for low back pain were provided in 2017 [5], considering it the most frequent disorder among workers and the second cause of work disability [5]. Low back pain is defined as pain in the back of the body that goes from the lower margin of the 12th rib to the lower fold of the buttock, with or without pain radiation to the lower extremities that lasts at least one day [3]. Anatomically, it is the pain that extends from the 12th rib to the iliac crest [6]. There are physical and psychological risk factors, as well as an unhealthy lifestyle, all of them can increase the risk of an episode of low back pain [7]. In cancer patients the third most common site of metastasis is the bone, its prevalence is 5 to 30%, within these, the metastases to vertebral bodies represent 70% of the total [8]. Also, it is relevant to mention that it is one of the causes of low back pain [8] leading to spinal instability in up to 10% of the patients [9]. Low back pain can be classified by its temporality, in acute, subacute and chronic, and by its pathophysiological mechanism in nociceptive low back pain, neuropathic low back pain and nociplastic low back pain (central sensitization) [6]. According to its etiology, it can be divided into three categories: non-specific low back pain, mechanical low back pain or low back pain that radiates to one o both limbs [6,7,10]. The diagnostic approach in patient with low back pain is carried out through the medical record and physical examination, including the neurological one [6,7]. The use of imaging tests is not recommended in non-specific low back pain, however, in patients with red flags, including in it cancer patients, it is necessary to do imaging tests to rule out any emergency causes [6]. The treatment of low back pain involves non-pharmacological management, drug treatments, interventional pain management and even surgical management [11]. Pharmacological management includes the prescription of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and muscle relaxants for the acute phase, it is required the use of opioids and serotonin-norepinephrine reuptake inhibitors antidepressants in very selected cases, as part of the treatment of chronic low back pain [12].
Primary outcome
Identify the prevalence of low back pain in cancer patients who were treated for the Pain Medicine Department of the National Institute of Cancer in México for a period of time from January 1st 2022 to December 31st 2023.
Secondary outcomes
The following factors were included in this study: Sociodemographic factors, the etiology of low back pain, oncological pathologies and clinical stage, pain intensity measured by Verbal Numerical Rating Scale (vNRS) and Verbal Rating Scale (NRS), the treatment used for low back pain and if it includes opioids, most frequent comorbidities, performance status scale, patients who underwent a interventional pain procedures for low back pain, patients facing radiating pain to limbs, body mass index, association with smoking and which patients are cancer survivors or have an active cancer.
Methods
Study Design
This is a retrospective, observational, cross-sectional study that included patients treated in Pain Medicine Department of the National Institute of Cancer in the period of time from January 1st 2022 to December 31st 2023. After the approval of the Ethical Committee for Clinical Investigation of this Institution, we realized the research in records’ patients and included patients who met the inclusion criteria. We used the keywords “low back pain,” “lumbar region pain,” and “lumbosacral pain” in the hospital computer system “INCANET,” after filtering data, the system threw up 4253 patients records, we reviewed each one of them and 977 patients’ records met the inclusion criteria. To estimate the universe, we consider the total number of consultations given by the Pain Medicine Department in 2022 and 2023, on average four consultations per patient a year are given by this department, so we consider our universe 8393 patients. We gather all the data needed to complete the sheets’ variables from the total number of patients included in this study (n=977) with a diagnoses of low back pain (Anexure 1).
Patient Selection
Inclusion criteria: Patients treated in the Pain Medicine Department during the period of time from January 1st, 2022 to December 31st, 2023 who were diagnosed with low back pain and whose records had all the information required for the study.
Exclusion criteria: Records with incomplete data for the determination of low back pain.
Statistical analysis
Data collected was analyzed using SPSS V.25.0. For the descriptive analysis, frequencies and percentages were used for nominal or ordinal qualitative variables, and for quantitative variables, measures of central tendency and dispersion and range were used for those with normal distribution. For nominal variables, frequency (n) and proportion (%) measures were used.
The inferential analysis was carried out with Pearson’s chi-square test or Fisher’s exact test for qualitative variables, while for quantitative variables the ANOVA test was used. The Kolmoron-Smirnov and Shapiro-Wilk normality tests were considered for quantitative variables, finally, for variables with abnormal distribution, normalization was performed with a logarithm with base 10. A value of p< 0.05 was used as statistically significant.
Results
The prevalence of low back pain in this group of patients was 11.64% (Figure 1). In this population, 67.3% (n=658) were women and 32.6% (n=319) were men. Regarding age, 10.74% (n=105) were between 18 and 44 years old, 41.14% (n=402) between 45 and 59, 37% (n=362) between 60 and 74, 10.9% (n=107) between 75 and 89 and 0.001% (n=1) were 90 more (Figure 2).
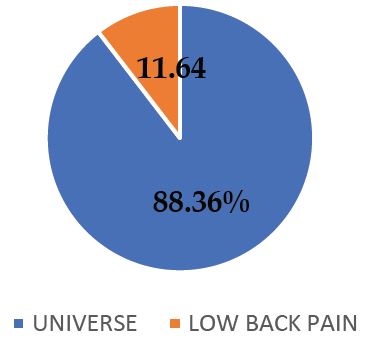
Figure 1: Prevalence of low back pain.
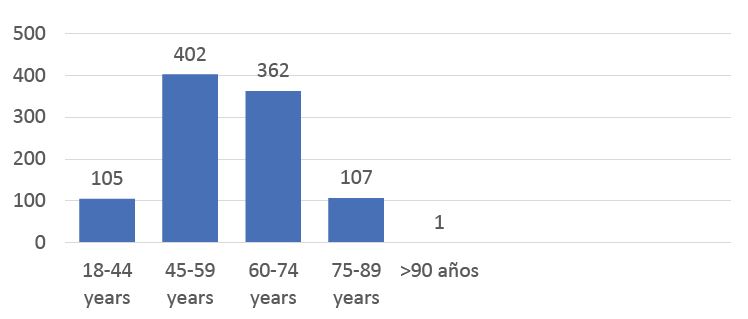
Figure 2: Age (years).
Considering the oncologic conditions, the most common one was breast cancer with 22.41% (n=219), 17.29% (n=169) was prostate/genitourinary cancer, 2.86% (n=28) was colorectal cancer, 3.27% (n=32) lung cancer, hematological cancer was 14.22% (n=139) and gynecologic cancer (mostly cervical cancer) that was 24.25% (n=237), the rest of them included bone cancer, any head and neck neoplasia, pancreatic and liver cancer, gastrointestinal cancer (other than colon cancer), tumor of soft tissue and skin, and other not classify in these categories, had a very small percentage less than 10% (Figure 3).
The main cause of low back pain was not determined, it was 39.2% (n=383%), the second most common cause was degenerative conditions with 28.65% (n=280) of the patients, 23.33% (n=228) were caused by metastases, and the rest of it like trauma or miofacial pain represented 5% of the total patients with low back pain (3.27%). Also, we observed more than two causes of low back pain in some patients (metastasis and degenerative) about 3.27% (Figure 4).
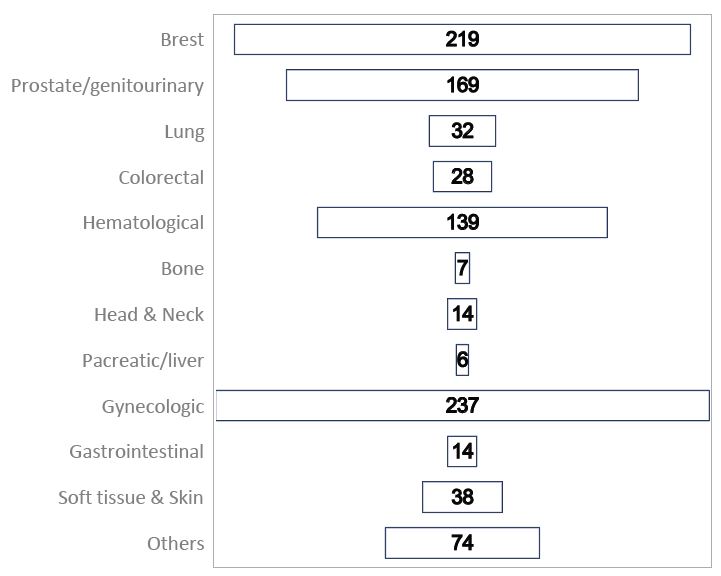
Figure 3: Oncologic conditions.
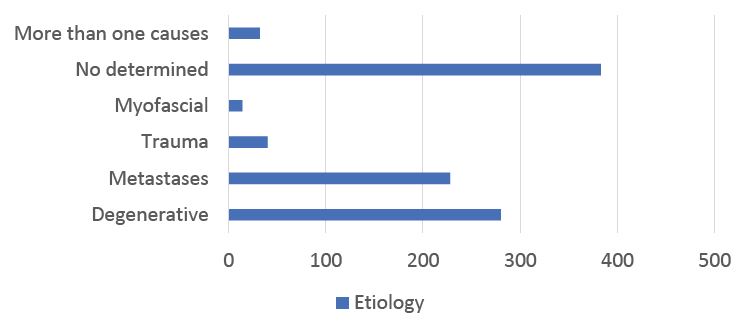
Figure 4: Etiology of low back pain in cancer patients.
Low back pain with radiating pain to limbs was found in 43.1% (n=421) of the patients. According to the data, 18.2% (n=178) of the total patients included in this study underwent one or more interventional pain procedure to treat pain.
The most common comorbidities found were diabetes and hypertension, followed by psychiatric diseases, rheumatic diseases and fiobromyalgia. The 28.3% of the cases (n=276) had one comorbidity, the 12.5% (n=122) had two comorbidities and the 1.94% (n=15) had three comorbidities, although 57.7% (n=564) had none. About 30.19% (n=295) were hypertensive, the 19.6% (n=191) were diabetic, 6.5% (n=63) had some sort of psychiatric condition, 1.2 % (n=13) had a rheumatic disease and 0.4% (n=4) of the total had fibromyalgia.
Pain intensity was evaluated by the verbal Numerical Rated Scale (vNRS) and de Numerical Rated Scale (NRS), we observed that the NRS at the consultation was on average 5.76 (±3.79), NRS of the background pain on average 5.65 (±4.15) and NRS breakthrough pain on average 7.19 (±2.78). These measures can read into mild in 20.5% of the patients, moderate in 36.8% and severe in 26.4%. Also, 16.3% of the total of the patients of this study had no pain at the consultation (Table 1).
Table 1: Pain Intensity measured by vNRS.
| Total of the patients | N=977 | 100% |
|---|---|---|
| Intensity | n | % |
| Mild | 200 | 20.47 |
| Moderate | 359 | 36.74 |
| Severe | 258 | 26.40 |
| Nopain | 160 | 16.37 |
Table 2: ANOVA Comparison of pain according to the NRS and the treatment used.
| PAIN | TREATMENT | N | MEDIA | SD | p |
|---|---|---|---|---|---|
| NRS | Non opioid | 154 | 6.14 | 4.419 | 0.002* |
| At theconsultation | Opioid | 794 | 5.61 | 3.625 | |
| Non pharmacological | 28 | 8.04 | 4.014 | ||
| Total | 976 | 5.76 | 3.793 | ||
| NRS | Non opioid | 154 | 6.46 | 4.713 | 0.000* |
| Background | Opioid | 794 | 5.41 | 4.003 | |
| Non pharmacological | 28 | 7.75 | 4.124 | ||
| Total | 976 | 5.65 | 4.155 | ||
| NRS | Non opioid | 154 | 6.33 | 3.363 | 0.000* |
| Breakthrough | Opioid | 794 | 7.29 | 2.621 | |
| Non pharmacological | 28 | 9.04 | 2.631 | ||
| Total | 976 | 7.19 | 2.789 |
The Karnovsky Scale was used to assess the performance status scale, finding normal activity in 65.9% of the patients (n=643), inability to work in 27.6% (n=269) and dependent activity in 6.6% of them (n=65).
Regarding the treatments that the patients received to control their low back pain, 15.45% (n=151) were treated with non-opioid medication, 81.6% (n=797) were under the prescription of opioids, and 2.96 (n=29) had nonpharmacological treatment. It’s important to mention that according to their daily morphine dose, 17.91% (n=175) were “naïve” patients and 82% were using opioid medication, the 18.5% (n=180) were considered non-tolerant, and 63.6% (n=622) were considered opioid-tolerant with a MDD >60mg/day.
Concerning risk factors, body mass index was assessed to categorize patient weight, observing that 5.2% of them had a BMI <18.5 kg/m2 classified as underweight, 36.5% of them were in a normal weight range 18.5-24.9 kg/m2 (n=357), 34.5% were overweight (25-29.9 kg/m2) (n=337) and 23.7% (n=232) were identified as >30 kg/m2 classified as obesity. The 34% (n=79) of patients with obesity and 32% (n=212) with overweight had been diagnosed with degenerative low back pain.
Of the 977 patients, 71.5% (n=699) did not smoke and 28.5% (n=278) did, and 21.7% (n=212) of them had a smoking rate consuming <10 packs/year, the rest of the smokers had a smoking rate greater than 10 packs/year represented less than 5%.
On the other hand, 72.7% (n=710) of the total number of patients had active oncological disease and 27.3% (n=267) were cancer survivors.
Active cancer and pain intensity were correlated using the verbal Numerical Rating Scale. The results obtained were more patients with moderate and severe pain intensity when they had active oncological disease. Of these, 36% (n=257) had moderate pain and 26% (n=188) had severe pain, comparing with survivors who had mild pain in 73% (n=197).
Finally, a comparative table was made between pain according to the NRS and the treatment used, to which the ANOVA test was applied, finding significance in the three measurements (current pain, background and breakthrough pain; p 0.000), showing the following:
• Pain at the consultation measurement, pain is lower in the opioid group, followed by the non-opioid group and finally in those without pharmacological treatment (5.61 vs 6.14 vs 8.04).
• In the background pain measurement, pain is lower in the opioid group, followed by the non-opioid group and finally in those without pharmacological treatment (5.41 vs 6.46 vs 7.75).
• In the breakthrough pain measurement, pain is lower in the non-opioid group, followed by opioid users and finally those without pharmacological treatment (6.33 vs 7.29 vs 9.04) (Table 2).
Discussion
It has been described that at least until 2022, the main types of cancer worldwide were lung, breast and colorectal [1]. Breast cancer was the most common one in up to 20% of cases, followed by genitourinary cancer that includes prostate in up to 17% of cases [13]; comparing it to our research it was possible to determine that the prevalence in the most common types of cancer is similar to that described in the literature, since the two main types of tumors found were breast cancer in 22.41% and genitourinary (including prostate) 17.29%; hematological tumors (included mostly multiple myeloma, lymphoma and leukemia, etc.) were the 3rd most frequent cause, with 14.22% of all patients; in 4th place, cervical cancer was identified in 24.5% of patients; the rest of the oncological diagnoses occurred in frequencies less than 10%, so the results of our study are similar to those reported in the world literature. According to the etiology of low back pain, we identified in the population evaluated firstly undetermined cause in 39%, the secIt has been described that at least until 2022, the main types of cancer worldwide were lung, breast and colorectal [1]. Breast cancer was the most common one in up to 20% of cases, followed by genitourinary cancer that includes prostate in up to 17% of cases [13]; comparing it to our research it was possible to determine that the prevalence in the most common types of cancer is similar to that described in the literature, since the two main types of tumors found were breast cancer in 22.41% and genitourinary (including prostate) 17.29%; hematological tumors (included mostly multiple myeloma, lymphoma and leukemia, etc.) were the 3rd most frequent cause, with 14.22% of all patients; in 4th place, cervical cancer was identified in 24.5% of patients; the rest of the oncological diagnoses occurred in frequencies less than 10%, so the results of our study are similar to those reported in the world literature. According to the etiology of low back pain, we identified in the population evaluated firstly undetermined cause in 39%, the second most frequent cause was of degenerative in 28.65% and in third place with 23.5% it was due to bone metastases, which agrees with the international reports, where it is mentioned that bone metastases is a frequent site of affectation up to 70%, of which the spine is affected in a percentage range of 5 to 30% of all cancer patients, a percentage similar to our study [8].
In 2021, the Journal The Lancet, published an article on low back pain that mentions that the prevalence of pain radiated to limbs due to herniated disc ranges from 2-4% and is more common between 30 and 50 years of age6. In our population, 43.1% had a pain radiated to limbs, which is way over what is reported worldwide in the non-cancer population, which may be due to some factors, such as metastasis to vertebral bone associated with vertebral fractures with secondary radicular compression as well as co-morbid factors of the patients (overweight, obesity, etc.) that could favor radicular compression and cause neuropathic low back pain.
The top most common presentation age of low back pain in our study was from 44 to 75 years (78.2%), pointed out that the group of patients from 45 to 59 years old were about 41%. The data reported in different articles differs of what we found, it is mentioned that the highest rate of affectation by low back pain is in older adults in up to 60% of cases [4]. The above can be attributed to the fact that since this is an oncological population, depending on the type of tumor, the age ranges may vary according to each specific cancer, which can also cause the age of presentation of low back pain to vary.
However, the literature describes that low back pain is more frequent in the female sex, up to 20% higher compared to the male sex [7], which was similar to what was observed in our research, identifying a greater number of cases in women (67.3% versus 32.7%).
Another relevant finding was the types of pharmacological treatment prescribed in our patients with low back pain. Of the total sample, 81.5% were taking opioids, which is not at all consistent with the treatment guidelines for low back pain. We attribute this discrepancy to the fact that the study included an oncological population with active disease in 72.7% of them, justifying the prescription of opioids, which constitutes the first line of pharmacological treatment according to different international guidelines for moderate or severe pain [11,12].
On the other hand, when observing whether there was a correlation between BMI (overweight or obesity) and low back pain of degenerative cause, we observed that of 58.2% of our population with BMI >25 kg/m2, the 19% of them had low back pain of degenerative cause, which shows that overweight/obesity can influence the presentation of this pathology15.
Finally, regarding the prevalence of low back pain in the adult population, it has been described that in Mexico it ranges between 10 and 30% [10], in our oncological population was 11.64%, therefore, it can be assured that the data collected are reliable and provide good validity to the research.
Conclusions
In the present study, we identified that the prevalence of low back pain in cancer patients was 11.64%, considering that it is a frequent reason for consultation in the department of pain medicine, however, the pharmacological management differs from the usual treatment of this entity in non-cancer patients. Likewise, we identified that in many cases the treatment prescribed was useful to provide adequate pain relief in our patients.
It is important to consider in the future, the performance of a prospective trial to observe the behavior of this painful condition and its clinical presentation in cancer patients to determine if the use of opioid analgesics is the cornerstone in cancer patients with low back pain.
Declarations
Funding: This study received no funding.
Ethical approval: This study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent: This study was a database-based study and therefore informed consent was not applicable.
Conflicts of interest disclosure: The authors declare that they have no financial conflicts of interest with regard to the content of this report.
Availability of data and materials: The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
This study was a database-based study and therefore research registration was not applicable.
References
- World. 2024. “Global Cancer Burden Growing, amidst Mounting Need for Services.” Who.int. World Health Organization: WHO. February 2024. https://www.who.int/en/news/item/01-02-2024-global-cancer-burden-growing--amidst-mounting-need-for-services.
- The Lancet Rheumatology. 2023. “The Global Epidemic of Low Back Pain.” The Lancet Rheumatology 5 (6): e305–5. https://doi.org/10.1016/s2665-9913(23)00133-9.
- Ferreira, Manuela L, Katie de Luca, Lydia M Haile, Jaimie D Steinmetz, Garland T Culbreth, Marita Cross, Jacek A Kopec, et al. 2023. “Global, Regional, and National Burden of Low Back Pain, 1990–2020, Its Attributable Risk Factors, and Projections to 2050: A Systematic Analysis of the Global Burden of Disease Study 2021.” The Lancet Rheumatology 5 (6): e316–29. https://doi.org/10.1016/s2665-9913(23)00098-x.
- Salud, Secretaría de. n.d. “011. Lumbalgia, Segunda Causa Más Común de Consulta de Primer Contacto.” Gob.mx. https://www.gob.mx/salud/prensa/011-lumbalgia-segunda-causa-mas-comun-de-consulta-de-primer-contacto?idiom=es-MX.
- “En El IMSS, Más de 300 Mil Consultas Por Lumbalgia En 2017 | Sitio Web ‘Acercando El IMSS al Ciudadano.’” n.d. Www.imss.gob.mx. http://www.imss.gob.mx/prensa/archivo/201810/246.
- Knezevic, Nebojsa Nick, Kenneth D Candido, Johan W S Vlaeyen, Jan Van Zundert, and Steven P Cohen. 2021. “Low Back Pain.” The Lancet 398 (10294). https://doi.org/10.1016/s0140-6736(21)00733-9.
- Vlaeyen, Johan W. S., Chris G. Maher, Katja Wiech, Jan Van Zundert, Carolina Beraldo Meloto, Luda Diatchenko, Michele C. Battié, Marielle Goossens, Bart Koes, and Steven J. Linton. 2018. “Low Back Pain.” Nature Reviews Disease Primers 4 (1). https://doi.org/10.1038/s41572-018-0052-1.
- Sahgal, Arjun, Sten D Myrehaug, Shankar Siva, Giuseppina L Masucci, Pejman J Maralani, Michael Brundage, James Butler, et al. 2021. “Stereotactic Body Radiotherapy versus Conventional External Beam Radiotherapy in Patients with Painful Spinal Metastases: An Open-Label, Multicentre, Randomised, Controlled, Phase 2/3 Trial.” The Lancet Oncology 22 (7): 1023–33. https://doi.org/10.1016/s1470-2045(21)00196-0.
- Planchard, Ryan F, Daniel Lubelski, Jeffery Ehersman, Safwan Alomari, Ali Bydon, Sheng-fu Lo, Nicholas Theodore, and Daniel M Sciubba. 2021. “Surgical Stabilization for Patients with Mechanical Back Pain Secondary to Metastatic Spinal Disease Is Associated with Improved Objective Mobility Metrics: Preliminary Analysis in a Cohort of 26 Patients.” World Neurosurgery 153 (June): e28–35. https://doi.org/10.1016/j.wneu.2021.06.034.
- Urits, Ivan, Aaron Burshtein, Medha Sharma, Lauren Testa, Peter A. Gold, Vwaire Orhurhu, Omar Viswanath, et al. 2019. “Low Back Pain, a Comprehensive Review: Pathophysiology, Diagnosis, and Treatment.” Current Pain and Headache Reports 23 (3). https://doi.org/10.1007/s11916-019-0757-1.
- Alemanno, Federica, Elise Houdayer, Daniele Emedoli, Matteo Locatelli, Pietro Mortini, Carlo Mandelli, Alberto Raggi, and Sandro Iannaccone. 2019. “Efficacy of Virtual Reality to Reduce Chronic Low Back Pain: Proof-of-Concept of a Non-Pharmacological Approach on Pain, Quality of Life, Neuropsychological and Functional Outcome.” Edited by Jane Elizabeth Aspell. PLOS ONE 14 (5): e0216858. https://doi.org/10.1371/journal.pone.0216858.
- Zhou, Tianyu, David Salman, and Alison H McGregor. 2024. “Recent Clinical Practice Guidelines for the Management of Low Back Pain: A Global Comparison.” BMC Musculoskeletal Disorders 25 (1). https://doi.org/10.1186/s12891-024-07468-0.
- Tringale, Kathryn R., Natalie Gangai, Andrew Chua, Kendra Godwin, Gloria Guman, Ilya Laufer, Kathleen N.S. Cathcart, et al. 2023. “Spine MRI Identifies Clinically Relevant Findings in Patients with Cancer Presenting with Back Pain.” Spine 49 (6): 419–25. https://doi.org/10.1097/brs.0000000000004803.
- Manchikanti, Laxmaiah. 2020. “Low Back Pain and Diagnostic Lumbar Facet Joint Nerve Blocks: Assessment of Prevalence, FalsePositive Rates, and a Philosophical Paradigm Shift from an Acute to a Chronic Pain Model.” Pain Physician 5;23 (9;5): 519–29. https://doi.org/10.36076/ppj.2020/23/519.
- Chen, Lingxiao, Qingyu Sun, Roger Chou, David B. Anderson, Baoyi Shi, Yujie Chen, Xinyu Liu, Shiqing Feng, Hengxing Zhou, and Manuela L. Ferreira. 2024. “Low Back Pain-Driven Inpatient Stays in the United States: A Nationwide Repeated Cross-Sectional Analysis.” International Journal of Surgery (London, England) 110 (3): 1411–19. https://doi.org/10.1097/JS9.0000000000000951.
