
Open Access, Volume 11
Prevalence of acute postoperative pain in cancer patients treated by a pain unit
Pola-Méndez Mirtha Nayeli1*; Guillen-Núñez María Del Rocío2
1Algology Resident, National Cancer Institute, Mexico.
2Department of Pain, National Cancer Institute, Mexico.
Pola Mendez Mirtha Nayeli
National Cancer Institute, Av. San Fernando 22, 14080 Mexico.
Email: mirtha_pola@hotmail.com
Received : February 27, 2025,
Accepted : March 21, 2025
Published : March 28, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Acute Postoperative Pain (APP) represents one of the greatest challenges faced by medical personnel, its management continues to be complicated in patients regardless of age and sex, as well as the comorbidities they present. It is documented that the importance of APP lies in its high frequency, inadequate treatment and the repercussions it has on the patient’s evolution and recovery.
Objective: Identify the prevalence of acute postoperative pain in cancer patients treated by the pain clinic of the National Cancer Institute during the period from January 2021 to December 2022.
Methods: Observational, descriptive and retrospective study, conducted from January 2021 to December 2022. For the statistical analysis, the SPSS version 25 program was applied. For the descriptive analysis, Pearson’s chi-square test was used to determine statistical significance. The signification thresholds were established at a level of p<0.05.
Results: Out of a universe of 1577 patients, 55 met the inclusion criteria, requesting interconsultation at the pain clinic in the first 24 hours after surgery. 52.7% were women and 43.7% men. The group with the highest incidence of APP was in >60 years (29.1%). Pain intensity was assessed through the ENA at 24, 48 and 72 hours; at 24 hours, moderate ANS (n=34) 61.8% was reported, at 48 hours mild ANS (n=35) 63.6% was reported, and at 72 hours most patients reported mild ANS (n=34) 61.8%. Opioids and non-opioid analgesics were used in 96.3% of patients for the treatment of DAP. Multimodal analgesia was used in 100% cases.
Conclusion: Uncontrolled acute postoperative pain can increase morbidity and mortality and treatment costs. This study addresses acute postoperative pain and the treatment provided by a pain unit, considering that the earlier the preventive treatment of pain is started, the better the results will be obtained.
Keywords: Acute postoperative pain; Postoperative pain; Cancer patient; Surgery; Analgesic treatment.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Nayeli PMM (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Pola-Méndez MN, Guillen-Núñez MDR. Prevalence of acute postoperative pain in cancer patients treated by a pain unit. Open J Clin Med Case Rep. 2025; 2338.
Introduction
The International Association for the Study of Pain (IASP) defines pain as an unpleasant sensory and emotional experience, associated with actual or potential tissue damage. The IASP proposed this definition in 2020 [1], which seeks to describe the complexity of pain and individualize the subjective and very personal experience of pain in each patient.
This entity can be classified according to temporality, pathophysiology, intensity, and etiology. According to its temporality, pain can be classified as acute pain and chronic pain.
Acute pain is a dynamic, complex, and unpleasant psychophysiological response to tissue damage and related acute inflammatory processes, which arises in response to injury, disease, or tissue inflammation. Ideally, acute pain goes away on its own and is limited to a set period, carrying out a protective biological function that reduces risky behaviors and promotes tissue recovery and healing. Although in a primitive environment acute pain promotes survival, in medical settings such as recovery from surgery, the physiological processes that accompany it, if left unchecked, can predispose to harmful influences on health [2].
Acute Postoperative Pain (APP) represents one of the greatest challenges faced by medical personnel, its management continues to be complicated in patients regardless of age and gender, as well as the comorbidities they present. It is documented that the importance of PDA lies in its high frequency, inadequate treatment and the repercussions it has on the patient’s evolution and recovery [3]. The prevalence of acute postoperative pain varies according to the time elapsed since the operation, the type of surgery, the predisposing factors, as well as the treatments for it [4]. It is estimated that approximately 80% of patients who undergo surgical interventions report acute postoperative pain and of this population, 75% affirm that the intensity of the pain is moderate to severe [5].
Suboptimal postoperative pain relief can lead to clinical and psychological changes, leading to increased morbidity and mortality rates, as well as treatment costs, as well as decreased postoperative quality of life [4]. Moreover, it is estimated that 5 out of 10 patients with acute postoperative pain will transition to a chronic process, called persistent or chronic postoperative pain, which will eventually lead to minor depression and pain-related catastrophizing [6].
In major surgeries, poorly controlled postoperative pain is associated with several adverse outcomes: It increases the risk of surgical wound infection, delays wound healing and increases the risk of cardiovascular and pulmonary complications [7], among others. These complications increase the economic burden of hospital readmissions, emergency room visits, and burden on caregivers [8]. A multicentre observational study was conducted in 2015 in which pain was observed after 18 different surgical procedures and identified that severe pain on the first postoperative day was directly correlated with the development of Chronic Postoperative Pain (CPSP) at 12 months after surgery. A 10% increase in the time spent with severe pain on the first postoperative day was associated with a 30% increase in the incidence of CPSP at 12 months [9].
Postoperative analgesia is essential for the patient’s functional recovery [8]. The safest, most effective, and best tolerated multimodal analgesic combinations depend on the type of surgery, the patient, and other factors, such as the length of the procedure and the patient’s comorbidities. Most multimodal combination regimens are based on a combination of opioid and non-opioid analgesics, in which the non-opioid analgesic can be an NSAID’s (Non-Steroidal Analgesics) or paracetamol (acetaminophen); other therapeutic groups such as gabapentin, N-Methyl-D-Aspartate receptor antagonists, alpha-2-agonists, local anesthetics, among others, can also be prescribed. In some cases, intravenous ketamine or lidocaine may be appropriate in the immediate postoperative period for hospitalized patients. Opioids, as well as NSAIDs, should be administered at the lowest effective dose for the shortest effective period, the selection of appropriate pharmacological treatments should be based on evidence, such as data on the Number Needed to Treat (NNT), analgesic effects, ability to reduce inflammation, and available formulations. Other therapeutic tools described with good levels of evidence are non-pharmacological interventions, such as physiotherapy, psychological interventions, local measures (RICE therapy: Rest-Ice-Compress-Elevate) among others.
Methods
Retrospective, observational and descriptive study. Patients diagnosed with acute postoperative pain with analgesic treatment granted by the Pain Clinic of the National Cancer Institute during the period from January 2021 to December 2022 were included. The data collected were recorded on a data collection sheet. For the statistical analysis, the SPSS version 25 program was applied. For the descriptive analysis, Pearson’s Chi-square test was used to determine statistical significance. Significance thresholds were set at a level of p<0.05.
Research ethics
This project, within the classification of risk to which the research subject is subjected, according to the General Health Law on health research, corresponds to a «risk-free investigation» since the data were collected from the patient’s file without intervening in the case management protocol.
Results
A total of 1557 files were reviewed according to the information provided by the INCANET statistical service with the keywords «postoperative pain», «acute postoperative pain» and «postoperative pain» during the study period. From this review of records, 55 patients were treated by the pain clinic in the immediate postoperative period, so this was the number of patients included in our study.
Total sample (n=55), a greater number of patients were women (n=29), representing 52.7%, while the male gender (n=26) represented 47.3% of the cases that presented with acute postoperative pain and required attention by a pain unit at the National Cancer Institute (Table 1).
The age group in which the highest incidence of acute postoperative pain was found was in people over 60 years of age, representing 29.1% (Table 1).
Table 1: Overwiev of the results.
| n | % | ||
|---|---|---|---|
| Sex | Male | 26 | 47.3% |
| Female | 29 | 52.7% | |
| Total | 55 | 100 % | |
| Age | 19-30 | 7 | 12.70% |
| 31-40 | 10 | 18.2% | |
| 41-50 | 8 | 14.50% | |
| 51-60 | 14 | 25.50% | |
| >60 | 16 | 29.1% | |
| Total | 55 | 100 % |
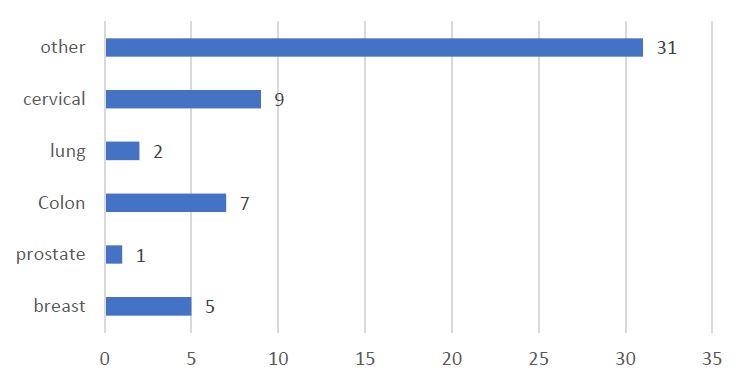
Graph 1: Cancer diagnosis.
In relation to oncological diagnoses, it was identified that the most frequent diagnosis was others (integrating in this group patients with renal cancer, gastric cancer, pancreatic cancer) (n=31) which is equivalent to 56.3% of the total sample; in second place is the diagnosis of cervical cancer (n=9) representing 16.3%, in third place colon cancer (n=7) with 12.7%, and the least frequent were breast cancer (n=5) with 9%, lung cancer (n=2) 3.6%, prostate cancer (n=1) with 1.8% and ovarian cancer and myeloma were not registered (Graph 1).
With respect to the type of surgical event to which the patients were subjected, abdominal surgery (n=27) was in first place, representing 49%, thoracic surgery (n=14) in 25.4% of patients, gynecological surgery and others (n=4) representing 7.2% respectively, in a smaller proportion was amputation (n=3) with 5.4%. breast surgery (n=2) 3.6% and nephrectomy (n=1) with 1.8% (Graph 2).
Table 2 shows the surgical history of the patients, observing that 13 patients had not undergone any surgical procedure previously, of which 7 were men (26.9%) and 6 women (20.6%); 42 patients had a history of previous surgeries represented by the female gender (n=23) 79.31 % and men (n=19) 73% of the total by gender.
Table 2: Surgical history.
| Sex | Male | Female | Total | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Previous surgeries | No | 7 | 26.92 | 6 | 20.69 | 13 | 23.64 |
| Si | 19 | 73.08 | 23 | 79.31 | 42 | 76.36 | |
| Total | 26 | 100 | 29 | 100 | 55 | 100 | |
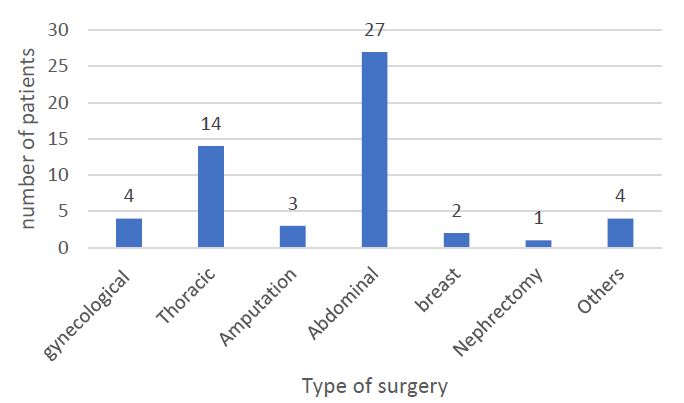
Graph 2: Type of surgery performed.
Table 3: Number of patients with chronic pain and previous analgesic treatment.
| Male | Female | Total | |||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Chronic pain | No | 7 | 26.92 | 5 | 17.24 | 12 | 21.8 |
| Previous | Si | 19 | 73.08 | 24 | 82.76 | 43 | 78.2 |
| Total | 26 | 100 | 29 | 100 | 55 | 100 | |
| Analgesic treatment | No | 2 | 7.69 | 1 | 3.45 | 3 | 5.5 |
| Previous | Si | 24 | 92.31 | 28 | 96.55 | 52 | 94.5 |
| Total | 26 | 100 | 29 | 100 | 55 | 100 | |
Table 4: Analgesics used in postoperative pain.
| Male | female | Total | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Opioid | 25 | 45.45 | 28 | 50.9 | 53 | 96.36 |
| Local anestesic | 4 | 15.38 | 10 | 38.46 | 14 | 25.45 |
| NMDA receptor antagonists | 0 | 0 | 2 | 7.69 | 2 | 3.64 |
| Alpha 2agonists | 3 | 11.54 | 0 | 0 | 3 | 5.45 |
| Simpleanalgesic | 17 | 65.38 | 22 | 84.62 | 39 | 70.91 |
| Gabapentinoids | 4 | 15.38 | 5 | 19.23 | 9 | 16.36 |
| NSAIDs | 16 | 61.54 | 15 | 57.69 | 31 | 56.36 |
| Tricyclic antidepressants | 1 | 3.85 | 3 | 11.54 | 4 | 7.27 |
Considering the important history of patients who underwent surgical procedures, in general terms, 21.8% did not have chronic pain prior to surgery and 78.2% had chronic pain prior to surgery, of which the highest percentage is represented by the female gender (Table 3).
According to the treatments used after the surgical procedure, it was observed that in 93.36% of cases, opioid analgesics were indicated in combination with non-opioid analgesics (NSAIDs, simple analgesics, gabapentinoids, TCAs, etc.) (Table 4).
Pain intensity was measured using the analog numerical scale (SEN) in postoperative patients, after starting the treatment established by the pain clinic at 24, 48 and 72 hours. At 24 hours, most reported a moderate ANS (intensity of 4 to 6) (n=34) 61.8%, at 48 hours a mild ANS (intensity of 1 to 3) (n=35) 63.6% and at 72 hours most patients continued to report an ANS classified as mild (n=34) 61.8% (Table 5).
Table 5: ENA (Analog Numeric Scale) comparison.
| 24h | 48h | 72h | ||||
|---|---|---|---|---|---|---|
| Tipo | n | % | n | % | n | % |
| Absent | 2 | 3.6 | 5 | 9.1 | 8 | 14.5 |
| Slight (1-3) | 9 | 16.4 | 35 | 63.6 | 34 | 61.8 |
| Moderate (4-6) | 34 | 61.8 | 9 | 16.4 | 11 | 20 |
| Severe (7-10) | 10 | 18.2 | 6 | 10.9 | 2 | 3.6 |
| Total | 55 | 100 | 55 | 100 | 55 | 100 |
| Pearson's chi-square 24 h versus72 h: 0.095 | ||||||
Discussion
Pain, despite being as old as man, being a subjective experience is not easy to define. According to a study conducted in Georgia in 2022, approximately 80% of patients who undergo surgical procedures report acute postoperative pain and of this percentage, 75% report that the intensity of the pain ranges from moderate to severe, another study reports similar figures where from a survey of 300 patients undergoing surgical procedures, 86% course with postoperative pain and 75% reported moderate to severe intensity [4,5].
In our study, it was found that patients undergoing surgery, treated by the pain clinic, had moderate acute postoperative pain in 61.8% in the first 24 hours after the surgical procedure performed, which is a slightly lower percentage than the reported literature, this may be due to the fact that a large proportion of patients with an oncological diagnosis have pain that is already treated prior to surgery. Which could influence the expression of pain in the postoperative period.
Postoperative pain control should ideally be carried out through multimodal analgesia strategies, both pharmacological and non-pharmacological measures. In this order of ideas, we were able to identify that almost in the total of our sample, an opioid analgesic was used for the control of acute postoperative pain in combination with other pharmacological groups [11]. Although world literature considers non-opioid pharmacological measures to be the first choice, we must remember that the population studied is of an oncological nature, which weighs opioid prescription.
In our study, opioid analgesics were prescribed in 53 patients with analgesic adjuvant with simple analgesics, gabapentinoids, NSAIDs, tricyclic antidepressants, local anesthetics, alpha 2 agonists, NMDA receptor antagonists considering the patient’s context and adjusting doses according to renal function. It is relevant to mention that 78.2% of our patients had chronic pain prior to the surgical procedure.
Conclusion
Acute postoperative pain when treated suboptimal can increase morbidity and mortality, treatment costs and quality of life after surgery, however, it is important to mention that there is currently an arsenal of pharmacological therapies for the treatment of it.
This study evaluated the prevalence of acute postoperative pain, and the therapeutic measures prescribed for a population of cancer patients undergoing a surgical event attended by a pain unit, observing that, of the total sample, through the implementation of multimodal pharmacological measures, most patients reported mild pain in the immediate postoperative period.
Derived from the fact that it is a retrospective study with a small sample size, this trial shows the need to conduct a prospective study to evaluate the prevalence of chronic postoperative pain and opioid prescription in this subpopulation of patients who continue after 12 months after the surgical event, as well as to identify whether the type of surgery and the duration of the surgery influence the outcomes in relation to the incidence and prevalence of postoperative pain.
Declarations
Conflict of interests: The authors declare that they have no conflicting interests.
Funding: The authors declare that they do not receive financial support for this article.
Contributions from authors: All authors contributed to the realization of this work. All Authors they also declare that they have read and approved the final version of the manuscript.
References
- Raja Sn, Carr Db, Cohen M, Finnerup Nb, Flor H, Gibson S, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. 2020.
- Chapman C Richard, et al. The transition of acute postoperative pain to chronic pain: an integrative overview of research on mechanisms. The journal of pain. 2017; 18: 359.e1-359.e38.
- López gonzalez J, et al. análisis de la eficacia y seguridad del bloqueo iliofascial continuo para analgesia postoperatoria de artroplastia total de rodilla. rev. soc. esp. dolor (online). 2012; 19: 231-238.
- Nanuli Ninashvili Tbilisi. Prevalence and intensity of acute post-operative pain and management aspects in adult patients: a cross-sectional tertiary hospital-based stud; state medical university; article in experimental & clinical medicine Georgia. 2022
- Paladini A, Rawal N, Coca Martinez M, Mehdi Trifa, Montero A. Advances in the management of acute postsurgical pain: a review. 2023.
- Papaioannou M, Skapinakis P, Damigos D, Mavreas V, Broumas G, Palgimesi A. the role of catastrophizing in the prediction of postoperative pain. pain med. 2009; 10: 1452.
- Gan TJ. poorly controlled postoperative pain: prevalence, consequences, and prevention. J pain res. 2017; 10: 2287-98.
- Rex Parka, Mohammed Mohiuddina, Ramiro Arellanoa, Esther Pogatzki-Zahnb, Gregory Klara, Ian Gilron; Prevalence of postoperative pain after hospital discharge: systematic review and meta-analysis. 2023; pr98: e1075.
- Shuang Liu, Leigh Kelliher. Physiology of pain—a narrative review on the pain pathway and its application in the pain management; digestive medicine research. 2022.
- Aasvang EK, Gmaehle E, Hansen JB, Gmaehle B, Forman JL, Schwarz J, et al. Predictive risk factors for persistent postherniotomy pain. The Journal ofv the American Society of Anesthesiologists. 2010; 112: 957-969.
- Chou R, Gordon Db, De Leon-Casasola Oa, Rosenberg Jm, Bickler S, Brennan T, et al. management of postoperative pain: a clinical practice guideline from the american pain society, the american society of regional anesthesia and pain medicine, and the american society of anesthesiologists’ committee on regional anesthesia, executive committee, and administrative council. j pain. 2016; 17: 131-57.
- DC Rosenberger, EM Pogatzki-Zahn. Chronic post-surgical pain e update on incidence, risk factors and preventive treatment options, University Hospital Munster, Munster, Germany. British Journal of Anaesthesia. 2022.
