
Open Access, Volume 11
Variant of Wellens’ syndrome: A case of critical stenosis in the right coronary artery Harimoto
Kuniyasu Harimoto, MD*; Tatsuya Kawasaki, MD, PhD
Department of Cardiology, Matsushita Memorial Hospital, Osaka, Japan.
Kuniyasu Harimoto
Department of Cardiology, Matsushita Memorial Hospital, Moriguchi, Osaka 570-8540, Japan.
Tel: +81-66992-1231, Fax: +81-66992-4845;
Email: harimoto.kuniyasu@jp.panasonic.com
Received : January 23, 2025,
Accepted : February 12, 2025
Published : February 14, 2025,
Archived : www.jclinmedcasereports.com
Keywords: Electrocardiography; Myocardial infarction; Right coronary artery; Wellens’ syndrome.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Harimoto K (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Harimoto K, Kawasaki T. Variant of Wellens’ syndrome: A case of critical stenosis in the right coronary artery. Open J Clin Med Case Rep. 2025; 2328.
Description
A 74-year-old woman presented with multiple episodes of chest pain. She reported that the symptoms had begun three days earlier and were triggered by exertion, such as walking outside in the cold. On the day of presentation, chest pain radiating to the left shoulder and chin woke her at 3 am and lasted approximately 30 minutes. Nine hours later, she was referred to the cardiology department of our hospital. On arrival, the patient was pain free and appeared well. She had a history of hypertension and was taking amlodipine 2.5 mg daily. Her vital signs and physical examination were unremarkable.
Electrocardiography revealed slight ST-segment elevation, along with terminal T-wave inversion, in the inferior leads, and minimal ST-T changes in the lateral leads (A), compared with the findings from four months earlier (B). Chest radiography and echocardiography were unremarkable. The high-sensitivity troponin T level was 0.165 ng/mL (reference value: ≤0.014), and the creatine kinase level was 88 U/L (reference range: 41 to 153). A diagnosis of acute coronary syndrome was made, and emergency coronary angiography revealed semi-occlusion in the middle portion of the right coronary artery (C, arrow) with no collateral flow from the left coronary arteries (D). Subsequent coronary intervention with stent implantation was successfully performed, and her postoperative course was uneventful, with no creatine kinase elevation above the upper limit of normal.
It is well established that ST-T segment abnormalities, with the exception of ST-segment elevation, are not reliable markers for identifying the ischemic site in the left ventricle [1,2]. However, biphasic T waves or deeply inverted T waves in leads V2 and V3 during a pain-free period — known as Wellens’ syndrome — are highly specific for critical stenosis of the proximal left anterior descending artery [3,4]. Similarly, in the current patient, the biphasic electrocardiographic changes (i.e., ST-segment elevation and terminal T-wave inversion) in the inferior leads were thought to be associated with critical stenosis of the right coronary artery, even though the patient was asymptomatic and had no wall motion abnormalities on echocardiography. This condition may be considered a variant of Wellens’ syndrome, because the critical stenosis involved the right coronary artery rather than the left anterior descending artery. It is worth noting that electrocardiographic changes in the right-sided variant of Wellens’ syndrome may be less pronounced than in the classic form, as demonstrated in the present case. Prompt coronary assessment and intervention, if necessary, should be considered in patients suspected of having either type of Wellens’ syndrome, as the classic form may eventually lead to myocardial infarction [3,5].
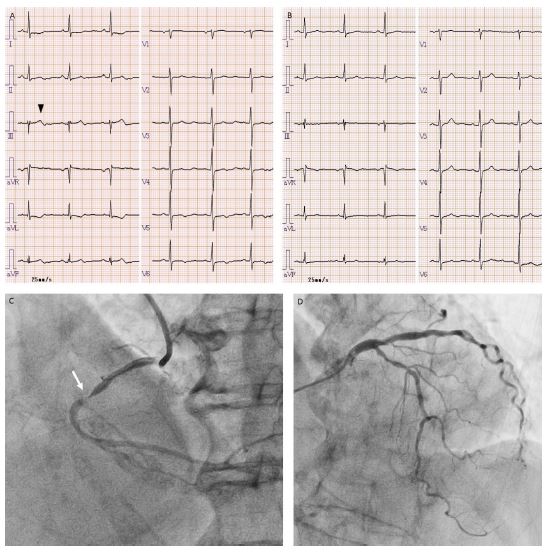
Figure 1: Electrocardiography and coronary angiography.
Electrocardiography at presentation (A) shows slight ST-segment elevation and terminal T-wave inversion in the inferior lead, typically in lead III (arrowhead), along with ST-T segment abnormalities in the lateral leads. None of these abnormalities were present in the findings from four months earlier (B). Emergency coronary angiography reveals semi-occlusion in the middle portion of the right coronary artery (C, arrow) and mild to moderate stenoses in the left anterior descending and left circumflex arteries, with no collateral flow to the distal portion of the right coronary artery (D).
Electrocardiography at presentation (A) shows slight ST-segment elevation and terminal T-wave inversion in the inferior lead, typically in lead III (arrowhead), along with ST-T segment abnormalities in the lateral leads. None of these abnormalities were present in the findings from four months earlier (B). Emergency coronary angiography reveals semi-occlusion in the middle portion of the right coronary artery (C, arrow) and mild to moderate stenoses in the left anterior descending and left circumflex arteries, with no collateral flow to the distal portion of the right coronary artery (D).
Disclosures: The authors state that they have no conflict of interest (COI).
References
- Fuchs RM, Achuff SC, Grunwald L, Yin FC, Griffith LS. Electrocardiographic localization of coronary artery narrowings: studies during myocardial ischemia and infarction in patients with one-vessel disease. Circulation. 1982; 66: 1168-76.
- Kang X, Berman DS, Lewin HC, Miranda R, Agafitei R, Cohen I, et al. Comparative localization of myocardial ischemia by exercise electrocardiography and myocardial perfusion SPECT. J Nucl Cardiol. 2000; 7: 140-5.
- de Zwaan C, Bär FW, Wellens HJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982; 103: 730-6.
- Al-Assaf O, Abdulghani M, Musa A, AlJallaf M. Wellen’s Syndrome: The Life-Threatening Diagnosis. Circulation. 2019; 140: 1851-2.
- Honda S, Kawasaki T. Wellens’ Syndrome. N Engl J Med. 2022; 387: e25.
