
Open Access, Volume 11
Femoral artery reconstruction with profunda reimplantation using femoral vein interponation following prosthetic patch infection: A case report and review of the literature
Yanina Kozovska1; Robert Finichi1; Elena Ulloa1; Beatrix Cucurux1; Georgios Sachsamanis1,2*
1Department of Vascular and Endovascular Surgery, Martha Maria Hospital, Nürnberg, Germany.
2Department of Vascular and Endovascular Surgery, University Medical Center Regensburg, Regensburg, Germany.
Georgios Sachsamanis
Department of Vascular and Endovascular Surgery, Martha Maria Hospital, Nürnberg, Germany.
Email: sachsamanis@hotmail.com
Received : January 19, 2025,
Accepted : February 10, 2025
Published : February 14, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Atherosclerotic lesions at the femoral bifurcation are a frequent cause of lower extremity claudication or chronic limb threatening ischemia. Endarterectomy of the common femoral artery and the profunda femoris is a well-established procedure with low mortality and morbidity rates, providing excellent long-term patency outcomes. It can be additionally executed as hybrid procedure, combined with recanalization of atherosclerotic lesions of the superficial femoral or crural arteries [1-3].
Arteriotomy closure is typically performed with an autologous or prosthetic patch, as primary closure of the vessel can lead to narrowing of the lumen. Commonly used materials include saphenous vein or bovine patches [3,4].
Nevertheless, infection of prosthetic patches can result in severe complications, such as vessel erosion and acute bleeding, frequently necessitating emergency surgical intervention for patch removal and reconstruction of the femoral bifurcation [5].
Herein we present the case of a patient who underwent femoral endarterectomy for acute limb ischemia, followed by wound dehiscence and patch infection, ultimately managed through reconstruction of the femoral bifurcation using the superficial femoral vein as interponation with reinsertion of the profunda femoris. Additionally, we discuss the possible treatment modalities for prosthetic femoral patch infection.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Sachsamanis G (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Kozovska Y, Finichi R, Ulloa E, Cucurux B, Sachsamanis G. Femoral artery reconstruction with profunda reimplantation using femoral vein interponation following prosthetic patch infection. A case report and review of the literature. Open J Clin Med Case Rep. 2025; 2327.
Case Presentation
A 68-year-old male was admitted in our accidents and emergencies department complaining of acute pain of his right lower extremity for the last three to four hours. Past medical history included hypertension, chronic kidney disease and severe alcohol abuse. He had additionally a below-the-knee amputation of his left lower extremity due to peripheral artery disease. No vascular surgery procedures were reported on the right side. Clinical examination revealed a cold, pale lower right extremity with absent femoral pulse. A computer tomography angiography showed a complete obstruction of his right common femoral artery due to extensive atherosclerosis. The right iliac axis was free of obstruction. The superficial femoral, the anterior tibial and the posterior tibial arteries were patent but heavily calcified.
After written informed consent, the patient was taken to the operating theater for femoral revascularization. An endarterectomy of the right common femoral artery, the profunda femoris and the proximal superficial femoral artery was performed after exposure of the femoral bifurcation. A biological prosthetic patch was used for closure of the arteriotomy. During the postoperative period, the patient developed a surgical site infection, which was initially managed conservatively through intravenous antibiotics, local debridement and negative pressure wound therapy. However, the condition of the patient deteriorated with rising infection parameters and pus secretion from the surgical site. Additionally, due to the alcohol abuse, the patient was severely incompliant regarding the antibiotic and the negative pressure wound therapy.
A surgical management was decided with exploration of the operative trauma and deep wound debridement. Additionally, a complete resection of the femoral bifurcation was performed with removal of the prosthetic graft and reconstruction of the femoral bifurcation using the distal superficial femoral vein from the contralateral extremity. The profunda femoris was reinserted in the vein interponation in an end-to-side fashion (Figure 1). Primary closure of the wound was performed with deep subcutaneous sutures. During the post-operative period, the patient developed acute kidney injury, which was managed without dialysis. He was discharged on the 8th postoperative day with good healing tendency of the surgical wound. After approximately 6 months no reinterventions were required.
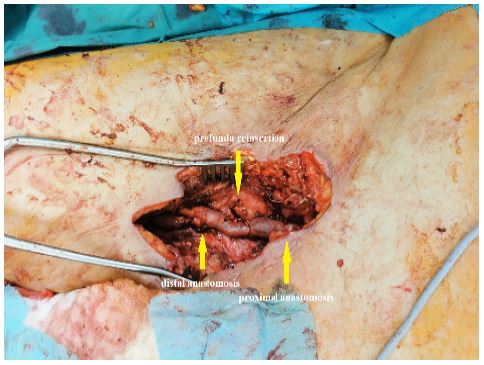
Figure 1: Intraoperative figure depicting the femoral vein interponation with reinsertion of the profunda femoris in an end-to-side fashion.
Discussion
Patch angioplasty with either prosthetic or autologous material following femoral endarterectomy is a common surgical procedure associated with good long-term patency rates. However, postoperative infection of the surgical site can lead to infection of the prosthetic patch, which can be a potentially disastrous complication with high mortality rates [6]. In a recent report from 2025, Okadome et al. compared the early outcomes of patients undergoing femoral endarterectomy with patch angioplasty using vein and bovine pericardial patches. Their study showed a 2.5% rupture (4/157 limbs) of vein patches and 4.7% (4/86) of bovine pericard patches (p=0.46) [7]. In another report from 2017, Dobrilovic et al. reported a 29% (2/7) early rupture rate of extracellular matrix patch following femoral artery repair [8].
A number of therapeutic approaches have been described for management of surgical site infection following femoral endarterectomy. A conservative approach with antibiotic therapy is rarely a viable option and is associated with high complication rates and increased mortality of approximately 50% [9]. Negative Pressure Wound Therapy (NPWT) following deep tissue debridement is another therapeutic alternative which can promote tissue granulation and accelerate wound healing. In a systematic review from Acosta et al., a number of different negative pressure wound therapy methods have been described for management of vascular surgical site infections, with the results being promising regarding prophylactic care of closed incisions [10]. NPWT is however also associated with complications such as bleeding and uncertain eradication of the infection [11].
Surgical management with removal of the infected patch and eventually reconstruction of the femoral artery is the best approach in cases of deep tissue infections where the prosthetic patch is very likely infected. In these cases, either autologous grafts (saphenous vein, femoral vein), cryopreserved allografts or in some cases even prosthetic materials can be used for femoral reconstruction. In a retrospective analysis between 2012 and 2018, Sapienza et al. reported the results of 26 patients who underwent operative management of prosthetic patch infection following femoral endarterectomy. They used great saphenous vein in 22 cases (85%) and cephalic vein in four cases (15%) for femoral reconstruction with a 5-year primary patency rate of 70% and limb salvage rate of 81% [5]. In another report from Furlough et al. cryopreserved arterial allografts were used in a number of infected vascular beds (57 cases), demonstrating a 30-day and late conduit complication rate of 14% and 15.8% respectively [12].
In our case, due to the medical history and incompliance of the patient we have decided that the best course of action was the complete removal of the infected vessel segment including the prosthetic patch and the reconstruction of the femoral bifurcation with reimplantation of the profunda femoris using the distal femoral vein from the contralateral lower extremity. Under the authors opinion this method has the best results in heavily infected vascular beds, effectively minimizing postoperative complications and maintaining vessel patency. A reconstruction using the great saphenous vein is a viable alternative and technically easier method, it can lead however to mismatch of the vessel lumen in the reconstructed area.
Conclusion
Prosthetic graft infection following femoral endarterectomy can pose a serious complication with high mortality rates. Femoral reconstruction with complete removal of the infected vessel segment including the patch and interponation using the femoral vein can be a viable alternative, minimizing postoperative complications and maintaining vessel patency.
References
- Nordanstig J, Behrendt CA, Baumgartner I, Belch J, Bäck M, Fitridge R, et al. Editor’s Choice – European Society for Vascular Surgery (ESVS) 2024 Clinical Practice Guidelines on the Management of Asymptomatic Lower Limb Peripheral Arterial Disease and Intermittent Claudication. Eur J Vasc Endovasc Surg. 2024; 67: 9-96.
- Conte MS, Bradbury AW, Kolh P, White JV, Dick F, Fitridge R, et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. Eur J Vasc Endovasc Surg. 2019; 58: S1-S109.
- Siracuse JJ, Gill HL, Schneider DB, Graham AR, Connolly PH, Jones DW, et al. Assessing the perioperative safety of common femoral endarterectomy in the endovascular eral. Vasc Endovasc Surg. 2014; 48: 27-33.
- Rerkasem K, Rothwell PM. Systematic review of randomized controlled trials of patch angioplasty versus primary closure and different types of patch materials during carotid endarterectomy. Asian J Surg. 2011; 34: 32-40.
- Sapienza P, Napoli F, Tartaglia E, Venturini L, Sterpetti AV, Brachini G, et al. Infection of Prosthetic Patches after Femoral Endarterectomy: An Unreported Complication. Ann Vasc Surg. 2019; 56: 11-16.
- Derksen WJ, Verhoeven BA, van de Mortel RH, Moll FL, de Vries JPM. Risk factors for surgical-site infection following common femoral artery endarterectomy. Vasc Endovasc Surg. 2009; 43: 69-75.
- Okadome J, Morisaki K, Matsuda D, Guntani A, Kurose S, Kyuragi R, et al. Comparison of Early Outcomes in Patients Who Underwent Common Femoral Thromboendarterectomy with Vein versus Bovine Pericardial Patches. Ann Vasc Surg. 2025; 110: 498-504.
- Dobrilovic N, Soukas P, Sadiq I, Goldstein L, Raman J. Early complications of biologic extracellular matrix patch after use for femoral artery repair. J Vasc Surg. 2017; 65: 705-710.
- Saleem BR, Meerwaldt R, Tielliu IF, Verhoeven EL, van den Dungen JJ, Zeebregts CJ. Conservative treatment of vascular prosthetic graft infection is associated with high mortality. Am J Surg. 2010; 200: 47-52.
- Acosta S, Björck M, Wanhainen A. Negative-pressure wound therapy for prevention and treatment of surgical-site infections after vascular surgery. Br J Surg. 2017; 104: e75-e84.
- Andersson S, Monsen C, Acosta S. Outcome and Complications Using Negative Pressure Wound Therapy in the Groin for Perivascular Surgical Site Infections after Vascular Surgery. Ann Vasc Surg. 2018; 48: 104-110.
- Furlough CL, Jain AK, Ho KJ, Rodriguez HE, Tomita TM, Eskandari MK. Peripheral artery reconstructions using cryopreserved arterial allografts in infected fields. J Vasc Surg. 2019; 70: 562-568.
