
Open Access, Volume 11
Exploring the comprehensive impact of pulmonary rehabilitation on recovery in patients with post-COVID interstitial lung disease: A case report
Belle Sharvani*; Priyanka Parida; Manjunatha H
Department of Physiotherapy, Akash Institute of Physiotherapy, India.
Belle Sharvani
Department of Physiotherapy, Akash Institute of Physiotherapy, India.
Email: sharuphysioakash@gmail.com
Received : December 28, 2024,
Accepted : January 27, 2025
Published : January 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Post covid Pulmonary rehabilitation being a comprehensive approach to recovery, a case study was done on patient with interstitial lung disease, dependent on oxygen port for his basic Activities of daily living. Multidisciplinary approach was explored where tailored exercise regime was planned patient centric using FITT principle. The outcome measure SpO2, RPE, FIM and St George’s Respiratory Questionnaire were noted every week to keep a check on the prognosis and to know the impact of pulmonary rehabilitation. The result concluded a significant improvement in FIM score and decrease in RPE, O2 dependency was reduced for basic ADL that in turn enhanced patients’ psychological well-being.
Keywords: Pulmonary rehabilitation; ADL; FIM; FITT; Interstitial lung disease.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Sharvani B (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Sharvani B, Parida P, Manjunatha H. Exploring the comprehensive impact of pulmonary rehabilitation on recovery in patients with post-COVID interstitial lung disease: A case report. Open J Clin Med Case Rep. 2025; 2323.
Background
Globally post covid 19 has triggered Chronic Respiratory Diseases (CRD) disturbring the physiological process of respiratory and cardiovascular fitness leading to deterioration in Activities of daily life [1]. CRD is an umbrella term describing various conditions affecting the lungs and airways like asthma, pneumoconiosis, Interstitial Lung Disease (ILD), and pulmonary sarcoidosis. The Sustainable Development Goal (SDG) defined by the United Nations (UN) is CRD as third leading cause of mortality with a substantial burden and cost globally from 2019 [1]. Hence World Health Organization (WHO) aim in 1/3rd reduction of premature mortality by implementing Pulmonary rehabilitation strategies for the period 2030 [4]. The three key roles outlines as: one billion more individuals enjoying better health and well-being, universal health coverage, and enhanced protection against health emergencies [5].
The Interstitial Lung Diseases (ILDs) are distributed as a group of over 200 chronic lung conditions characterised by inflammation, dyspnoea on exertion, troublesome cough, exercise intolerance, and poor health-related quality of life [2]. A pathologic abnormalities occur predominantly in the lung interstitial, a connective tissue framework surrounding the alveoli, airways and blood vessels. Recently, development of pulmonary fibrosis after COVID-19 infection has been reported, most commonly in those who have undergon e mechanical ventilation [3]. ILDs vary in underlying diagnoses and clinical course where comprehensive supportive care for all ILD subtypes can aid to optimise clinical outcomes and patient wellbeing. The key elements of comprehensive supportive care focusing on interventions delivered by physiotherapists include pulmonary rehabilitation, supplemental oxygen, education, psychosocial support and symptom management.
Pulmonary Rehabilitation (PR), a comprehensive intervention that is tailored exercise training based on patients’ symptoms, education and behaviour change that is designed to improve the physical and psychological condition of people and to promote long-term adherence to health-enhancing behaviours. The PR core components include structured and progressive individually tailored exercise training designed by a rehabilitation team by a multidisciplinary healthcare professional. The rehab aims on self-management education, patient assessment and outcomes measurement and aid in reducing dyspnoea, increases exercise capacity, improves health-related quality of life (HRQoL) and confers social support. Despite its proven benefits, PR remains underused and under resourced [7]. Less than 5% of people with COPD who may benefit from PR receive it. There are studies that recommend focusing solely on PR an FEV1 < 50% predicted. The evidence base for PR has evolved substantially in recent years to include other CRDs and novel models for delivery remotely using telehealth technologies too. Evidence-based guidelines should lead to greater knowledge of the proven benefits of PR, highlight the role of PR, and in turn foster referrals too. However, data for patients with Interstitial Lung Disease (ILD) are limited. This case study aimed to examine an effect on an inpatient pulmonary rehabilitation on functional status and quality of life for a post-covid patient.
Aim
To explore the comprehensive impact of pulmonary rehabilitation on patients’ recovery phase with Post-COVID interstitial lung disease.
Case Description
A case of 74 years old male with a history of Post covid Interstitial Lung Disease and Liver Cirrhosis from 2 to 5 years respectively came to physiotherapy department in a wheelchair with portable oxygen cylinder of 6 L. Patient had Pulmonary consultation and was advised for pulmonary conditioning and rehabilitation along with supportive therapy and medications. An evidence based pre assessment for vitals like Respiratory rate, Oxygen saturation, Blood pressure was carried out followed by outcome scale such as FIM, dyspnoea rate of perceived exertion, St George’s Respiratory Questionnaire were administered as a part of Cardio pulmonary rehabilitation.
Patient symptoms:
• Unable to maintain oxygen saturation at room temperature
• Respiratory Distress in basic ADL
• Oxygen dependency of 6L
• Fatigue level grade 4
• Decreased exercise tolerance
• Decreased ADL
• Decreased MET value
Patient centric goal was:
• To maintain the oxygen saturation at room temperature
• To improve respiratory muscle strength
• To reduce oxygen dependency
• To reduce fatigue level
• To improve breathing pattern
• To improve exercise tolerance
• To improve ADL
• To increase MET value
Intervention
The treatment plan was directed based on patient centric goal and tailored exercise programme was designed for the patients. FITT (Frequency, Intensity, Time, Type) principle, being one of the key principles in prescribing exercise programme was designed weekly based on the parameters that improved and showed variations. The overall treatment duration planned was 45 minutes, with 20 second bouts after each exercise. Oxygen saturation was monitored throughout the exercise to observe the physiological changes in oxygen consumption during individual exercise. FIM instrument and FSS was administrated at time of admission and reassessed weekly.
The instruments used as a part of exercise programme was an Incentive spirometer, Weight cuff (500 g), Thera bands, Pillows, Dumbbells, Balloon, Pulse Oximeter, walker, respiratory muscle trainer, lung expander, acapela, treadmill. Intervention included anaerobic and aerobic circuit training which had three phases: warm up, tailored isometric, isotonic exercise of Respiratory muscles followed by cool-down phase.
The exercise regime was as follows for circuit training.
a) Pursed lip breathing: Pursed lip breathing helps in controlled breathing, relieves shortness of breath, improves gas exchange, and decreases the effort required to breathe. It creates a back pressure producing a small amount of Positive End-Expiratory Pressure (PEEP) which opposes the forces exerted on the airways from the exhalation flow. It helps to support breathing by opening the airways during exhalation and increasing the excretion of volatile acids in the form of carbon dioxide preventing or relieving hypercapnia. Hence pursed lip breathing makes the body relaxed, so before starting the exercise and in interval of each exercise, the patient was instructed to perform 4-5 pursed lip breathing exercises like balloon blow and candle blow.
b) Diaphragmatic breathing exercise: Diaphragmatic breathing exercise was taught to patient with 500gm resistance in semi-Fowler position.
c) Thoracic expansion exercise: Thoracic expansion exercise was practised with the help of dumbbells with full lung expansion with a 2 sec hold in the 1st week and then gradually the hold count and set were increased 2 sec every week to improve the lung volume and capacity. This technique aid in improving the lung expansion.
d) Activities in the bed: Bed activities include cycling (forward & backward), Bridging (unilateral/bilateral), Superman exercise, and Pelvic rotation (hip, knee flexion) were taught and practiced for 10 counts, with a rest period of 2 mins of about 3 sets.
e) Swiss ball exercise: Swiss ball exercises were practised as part of core muscle activation for about 20 repetitions.
f) Stretching: Intercoastal stretching exercises improve the muscle tensile stretch and aid in elasticity and recoil mechanism during lung expansion. Patient was made to do 4 repetitions of manual and assisted stretch during inspiration.
g) Respiratory muscle training: Breathing in or out forcefully through a handheld device like incentive spirometer and acapela was made to do for about 5 repetition 3 cycles.
h) Endurance or interval training: Aerobic training like cycling, walking in parallel, pushing wheelchair was made to as part of ADL.
i) Resistance or weight training: Set of light weights, resistance bands and weight machines were used for training the patient with periodic rest and O2 support.
j) Wall push off: Anaerobic static exercise like wall pushes up by standing facing a wall, hands flat on the wall at chest level followed by slowly lowering face and chest towards the wall.
k) Shoulder press: Modified arm press was taught to patient in sitting position with arms by the side, holding a walking stick in hands, and bringing the stick up to chest.
l) Sit to stand: As a part of ADL sit to stand on a firm chair was made to do for about 5 repetitions with pacing technique to avoid fatigue.
m) Functional Training: A fitness methodology that helps you improve patient strength and stability across a range of movements where patient was asked to perform everyday tasks and recreational activities with intermittent O2 support.
Pre-Assessment vitals: SpO2: 72% with 6 L of O2, FIM scale: 67/126, MET score: 2- sitting, Fatigue severity Scale (FSS) level: 54 (36-normal value)- Grade 4.
Sessions: Weekly 3/45 mins duration with intermittent rest period.
Protocol
| Month | Duration | Exercise | SPO2 | MET | FIM |
|---|---|---|---|---|---|
| August | Week 1-4 | -Preassessment of vitals and outcome scales. -Pursed lip breathing exercise x 5 times -Wheel chair sit to stand with walker 5 rep -Thoracic expansion exercises x3 times x no hold -Diaphragmatic exercise x3 times x3 cycles |
72%-6 L | 2 | 65 |
| September | Week 1- 4 | -Pursed lip breathing exercise x 5 times -Thoracic expansion exercise x 4 times x 2 sec hold progressed to 4 sec -Diaphragmatic breathing exercise x 5 mins progressed with weight 500 g -Aerobic exercises x10min progressed to 12 min with reduced O2 support by 5 L - Swiss ball exercises x 5min |
70%-6 L | 2 | 67 |
| 78%-6 L | 2 | 70 | |||
| 78%-6 L | 3 | 74 | |||
| October | Week 1-4 | - Static exercise (same week exercise) - Swiss ball exercises x 5 min -Thera band exercises -Posture correction exercises -Pacing activities -Acapela and Incentive spirometer for 3 counts -Intercostal stretching 5 rep *3 cycles |
80%-5 L | 3 | 78 |
| 84%-5 L | 3 | 78 | |||
| 84%-4 L | 3 | 82 | |||
| November | Week 2-4 | - Static exercise -Pacing activities -Energy conservation exercises -Treadmill walking with modified Bruce protocol x6min -Incentive Spirometry -Static exercise (same week exercise) -Respiratory muscle training with resistance -Cycling x 5 min -Box breathing (4,7,8) |
86%-4 L | 3 | 82 |
| 86%-3 L | 3 | 85 | |||
| 92%-3 L | 3 | 96 |

Figure 1: Wheel chair mobilization.
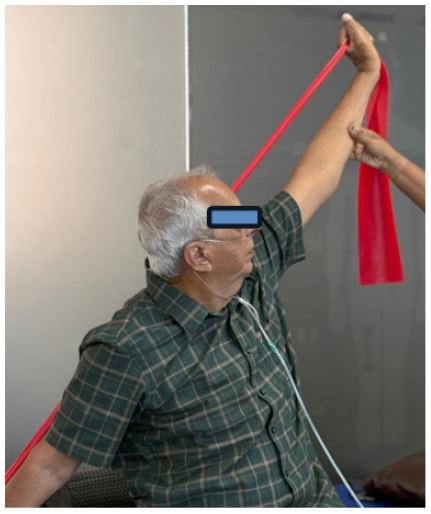
Figure 2: Strengthening training.

Figure 3: ADL training.

Figure 4: Independent walking indoor.
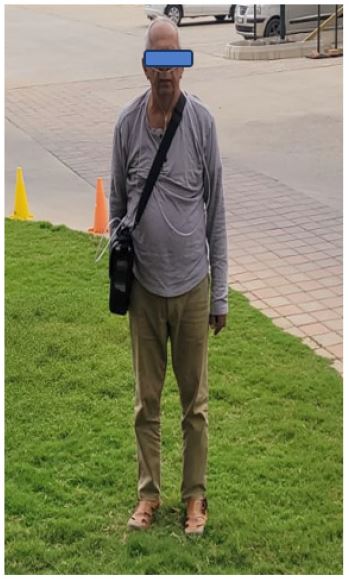
Figure 5: Independent walking outdoor.

Figure 6: Treadmill training.
Results
The graph showed a prognosis of the outcome score as a result of exercise programme tailored for this patient. There was a significant improvement in FIM score and ADL activities, but minimal variation in MET value and saturation level.
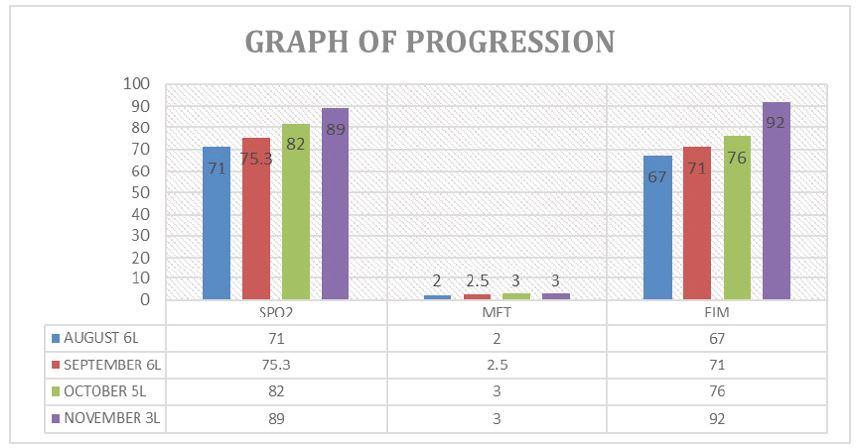
Graph 1:: Showing the progression for 4 months in SPO2, MET and FIM level.
Conclusions
Post covid respiratory muscle weakness and exercise intolerance have made many patients to be depended on mechanical breathing. Rehabilitation therapy for acute respiratory distress syndrome acts as an important adjunct to recovery. Functional training, a fitness methodology that helps to improve muscle strength and stability across a range of movements can benefit in easy ADL activities. Several studies concluded that pulmonary rehabilitation can aid in enhancing exercise capacity, sleep quality, depression and quality of life in terms of health but patient depended on O2 assume as burden to be part of rehabilitation program. Hence this study aimed to do a case study on patient depended on O2 consumption for his daily living activities to have a routine exercise programme in order to be self-depended and prevent further complications. In this case study Rehabilitation from the day of admission to the day of discharge, and the day of follow-up, all the scales and questionnaires were examined. The variation in scores during these four months indicated substantial progress on induvial parameters. Our study also aimed to provide the way for pulmonary rehabilitation programs to be introduced in the majority of hospitals and community centres.s
The study treatment plan was limited to respiratory and functional mechanism, hence psychological component can be considered as key effort for motivation of the patient as a follow up programme. Environmental barriers can be addressed in achieving the ultimate goal of delivering high-quality care. Patient awareness of exercise can aid as advantages that may lead to increased involvement and improvements in functional characteristics and quality of life. No intervention is successful without a proper follow-up, hence telerehabilitation can be incorporated on daily basis as education and continuation for an exercise program.
References
- Nakazawa A, Cox NS, Holland AE. Current best practice in rehabilitation in interstitial lung disease. Therapeutic advances in respiratory disease. 2017; 11: 115–128.
- Anne E Holland. Physiotherapy management of interstitial lung disease. Journal of Physiotherapy. 2022; 68: 158-164.
- Momtazmanesh Sara, et al. Global burden of chronic respiratory diseases and risk factors, 1990–2019: an update from the Global Burden of Disease Study 2019 . eClinical Medicine. 2019 ; 59: 1019 36.
- Chronic respiratory diseases: a global view Labaki, Wassim W et al. The Lancet Respiratory Medicine. 8: 531–533.
- Rochester CL, Alison JA, Carlin B, et al. Pulmonary Rehabilitation for Adults with Chronic Respiratory Disease: An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2023; 208: e7-e26.
- Dowman L, Hill CJ, May A, Holland AE. Pulmonary rehabilitation for interstitial lung disease. Cochrane Database Syst Rev. 2021; 2: CD006322.
- Keating A, Lee A, Holland AE. What prevents people with chronic obstructive pulmonary disease from attending pulmonary rehabilitation? A systematic review. Chron Respir Dis. 2011; 8: 89–99.
- Lu H, Liu N, Hu JY, Wang X, Li Y, Song M, et al. The effectiveness, safety and compliance of Zheng’s supine rehabilitation exercise as a rehabilitation programme among elderly patients with AECOPD. Clin Respir J. 2020; 14: 533–540.
- Hume E, Rochester CL, Vogiatzis I. In: Pulmonary rehabilitation. 2nd ed. Goldstein R, Donner CF, Ambrosino N, editors. Boca Raton, FL: CRC Press; 2021. Enhancing use and delivery of pulmonary rehabilitation. 2021: 29–39.
- Alharbi MG, Kalra HS, Suri M, et al. Pulmonary Rehabilitation in Management of Chronic Obstructive Pulmonary Disease. Cureus. 2021; 13: e18414.
- Sharma BB, Singh V. Pulmonary rehabilitation: An overview. Lung India. 2011; 28: 276-284.
- Nandanwar RR, Singh R, Karanjkar SM, Bhagwani RS. The Impact of Pulmonary Rehabilitation in a Case of Acute Respiratory Distress Syndrome with Bronchopneumonia: A Case Report. Cureus. 2022; 14: e32671.
