
Open Access, Volume 11
Infective endocarditis or not? That is the question
Sanraksha Mayya1*; Tejas Bende1; Tushar Deore2; Mangesh Danej3; Geethu Joe4; Rajeev Soman5
1Fellow, Department of Infectious Diseases, Jupiter Hospital, Pune, India
2Consultant Orthopaedic Spine Surgeon, Jupiter Hospital, Pune, India
3Consultant Cardiologist, Jupiter Hospital, Pune, India
4Consultant Microbiologist, Jupiter Hospital, Pune, India
5HOD and Consultant, Department of Infectious Diseases, Jupiter Hospital, Pune, India
Sanraksha Mayya
Department of Infectious Diseases, Jupiter Hospital, Pune, India.
Tel: +919359546657;
Email: sanraksha.mayya@gmail.com
Received : December 16, 2024,
Accepted : January 20, 2025
Published : January 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
This case is illustrative of the dilemma whether Infective Endocarditis (IE) existed or not in the setting of a patient with blood culture positive with an organism typical of IE (Streptococcus gordonii), who had cardiac abnormalities and vertebral osteomyelitis.
Keywords: Infective endocarditis; Streptococcus gordonii; 2023 Duke-ISCVID criteria.
Abbreviations: IE: Infective Endocarditis; CECT: Contrast Enhanced Computed Tomography; MRI: Magnetic Resonance Imaging; TEE: Transoesophageal Echocardiogram.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Mayya S (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Mayya S, Bende T, Deore T, Danej M, Joe G, Soman R. Infective endocarditis or not? That is the question. Open J Clin Med Case Rep. 2025; 2321.
Introduction
Whether Infective Endocarditis (IE) is present in a patient or not, determines many aspects of treatment and prognosis and is therefore a crucial clinical consideration.
Case Presentation
60-year-old gentleman was admitted due to low backache and fever for eight days. There was tenderness in the left paraspinal lumbar region at L2-L3 level and an ejection systolic murmur in the left parasternal region. On further enquiry, the patient mentioned that he had the murmur since childhood but was never evaluated for it.
An ultrasound guided psoas abscess drainage was done. Gram stain showed many pus cells and gram-positive cocci in pairs and chains. The patient was started on treatment with daptomycin 700 mg (10 mg/kg dose) intravenously once a day. This drug would cover methicillin susceptible as well as methicillin resistant staphylococcus aureus and streptococcus species. Pus culture from the psoas abscess grew Streptococcus gordonii (bacterial identification and antibiotic susceptibility testing done by VITEK 2 automated system). Two sets of blood cultures drawn two hours apart grew Streptococcus gordonii as well, with susceptibility to benzylpenicillin and ceftriaxone.
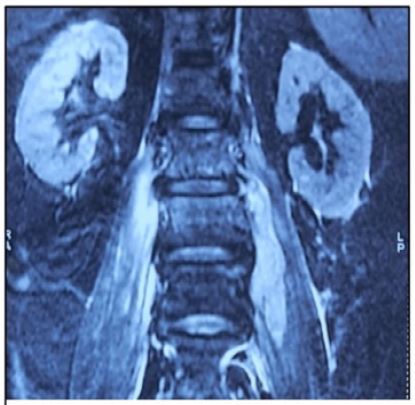
Figure 1: MRI spine with L2-L3 spondylodiscitis with bilateral psoas abscess.
Daptomycin was switched to ceftriaxone 2-gram 12 hourly for six weeks after identification and antibiotic susceptibility testing report was received. Histopathological examination of the abscess revealed an organising acute on chronic inflammation. Two sets of blood cultures that were repeated at the end of treatment were sterile.
Discussion
This case is illustrative of the dilemma whether IE existed or not in the setting of a patient with blood culture positive with an organism typical of IE, who had cardiac abnormalities and vertebral osteomyelitis.
The patient had two sets of blood cultures growing an organism, Streptococcus gordonii, that is typical for Infective Endocarditis (IE). This is a major criterion in the 2023 Duke-ISCVID criteria [1]. The patient’s profile also fulfilled three minor criteria: fever, a predisposing cardiac condition namely, pulmonary valve stenosis, and vertebral osteomyelitis (which could be due to an embolic phenomenon).
Although not in the 2023 Duke-ISCVID criteria, the propensity of various streptococci in cases with bacteraemia to produce IE is species dependent and the prevalence of IE is as follows in descending order: S. mutans (47.9%), S.gordonii (44.2%), S.sanguinis (34.6%), S.gallolyticus (30.2%), S.mitis/oralis (19.4%) [2].
Points against the diagnosis were that isolated pulmonary valve IE is extremely rare. Secondly, although no vegetations were found, other findings of valve destruction were also not present. Thirdly, a right sided endocarditis would usually be expected to cause pulmonary embolism rather than systemic embolism. Mitral annular calcification is a rare predisposing condition for IE which raised the possibility of left sided IE as well. However, that was ruled out by TEE.
The patient fulfilled one major and three minor criteria, and therefore had definite endocarditis by 2023 Duke-ISCVID criteria, in spite of absence of a vegetation on echocardiogram.
There was a small possibility of a vegetation in the pulmonary artery itself which would be missed by conventional echocardiography. However, had it been present, it would have been detected as a filling defect in the CECT thorax.
IE in the absence of an echocardiographic evidence of a vegetation appears to be uncommon, although according to a twenty-year-old study, only 87.1% of patients with definitive endocarditis, as per modified Duke criteria, had evidence of vegetations on echocardiography [3].
Cardiac CT has a somewhat limited role in native valve endocarditis except in cases where TEE is contraindicated. It has a slightly lower sensitivity of 91% as compared to 97% of TEE for detecting valvular vegetations. However, it is excellent at evaluating complications of IE such as abscesses, fistulae and pseudoaneurysms [4].
Although fluorodeoxyglucose Positron Emission Tomography (PET) scan is an excellent test for prosthetic valve endocarditis, it has a low sensitivity in native valve endocarditis and is not recommended for routine use as in this situation [4].
Conclusion
Finally, the dilemma of whether IE was present or not in this case was becoming difficult with evidence for and against almost evenly balanced. However, this would not matter from a therapeutic perspective as there was no indication for surgical management of IE in this patient and 6 weeks treatment with ceftriaxone would be adequate for both IE and vertebral osteomyelitis.
References
- Fowler VG, Durack DT, Selton-Suty C, Athan E, Bayer AS, Chamis AL, et al. The 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: Updating the Modified Duke Criteria. Clin Infect Dis. 2023; 77: 518-526.
- 2. Chamat-Hedemand S, Dahl A, Ostergaard L, Arpi M, Fosbol E, Boel J, et al. Prevalence of Infective Endocarditis in Streptococcal Bloodstream Infections Is Dependent on Streptococcal Species. Circulation. 2020; 142: 720-730.
- Murdoch DR, Corey GR, Hoen B, Miró JM, Fowler VG Jr, Bayer AS, et al. International Collaboration on Endocarditis-Prospective Cohort Study (ICE-PCS) Investigators. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch Intern Med. 2009; 169: 463-73.
- Horgan SJ, Mediratta A, Gillam LD. Cardiovascular imaging in infective endocarditis: a multimodality approach. Circulation: Cardiovascular Imaging. 2020; 13: e008956.
