
Open Access, Volume 11
Anatomic variation of kidney: A rare finding in a 17 years old with peritonitis secondary to ruptured appendix
Omotayo HA1,2*; Edomwonyi D2; Omotayo MT3
1Department of Anatomy, Lagos State University College of Medicine, Ikeja, Lagos, Nigeria.
2Helping Hands Royal Hospital, Lagos, Nigeria.
3Department of Community Health, Lagos University Teaching Hospital, Lagos, Nigeria.
Omotayo HA
Department of Anatomy, Lagos State University College of Medicine, Ikeja, Lagos, Nigeria.
Helping Hands Royal Hospital, Lagos, Nigeria.
Email: haomotayo@gmail.com & hameed.omotayo@lasucom.edu.ng
Received : December 13, 2024,
Accepted : January 16, 2025
Published : January 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Ectopic kidney is a rare developmental anomaly. Such kidneys may be asymptomatic or present with vague symptoms or remain unknown during the lifetime. Early detection and recognition of an ectopic kidney can prevent long-term complications. We report a 17-year-old boy with ectopic right kidney who presented with intermittent episodes of lower abdominal pain for one month which later becomes generalized with associated fever. On clinical evaluation a tender lump was palpable in the right lower quadrant of the abdomen. Sonography revealed peritonitis secondary to ruptured appendix while Intravenous Urogram shows normal functioning right kidney in the pelvis and normal sited left kidney. Further, full blood count done shows raised leukocytosis. Urine examination had no growth. An assessment of peritonitis was made. The patient was managed on empirical antibiotics, worked up for exploratory laparotomy. A ruptured appendix was seen at laparotomy along with a lump on the mid line identified as the right pelvic kidney which was looking normal. Patients presenting with lower abdominal pain, and a palpable lump in the lower abdomen, one must include ectopic kidney in the differential diagnosis.
Keywords: Acute hydronephrosis; Ectopic kidney; Lumbar kidney; Ruptured appendix.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Omotayo HA (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Omotayo HA, Edomwonyi D, Omotayo MT. Anatomic variation of kidney: A rare finding in a 17 years old with peritonitis secondary to ruptured appendix. Open J Clin Med Case Rep. 2025; 2320.
Introduction
Renal Ectopia or ectopic kidney is a developmental anomaly resulting from failure of the solid organ to migrate to its normal location within the retroperitoneal space. Other than the pelvis, cases of iliac and thoracic kidney have also been reported [14]. An ectopic kidney is a congenital abnormality in which a kidney is located inferior, superior, or on the opposite side of its usual position [15]. Ectopic kidney on the right side above the level of aortic bifurcation is rare [13]. The ectopic pelvic kidney is a rare anomaly about 1:2500 live births, left side being more common [12]. According to Bergman et al. incidence of ectopic kidney is 1:100/500, ectopic thoracic kidney 1:13,000, solitary kidney 1:1000, solitary pelvic kidney 1:2200, one normal and one pelvic kidney 1:3000 and one crossed renal ectopia 1:700 [2].
In general, the most common position is in the pelvis opposite the sacrum and below the aortic bifurcation [7]. The clinical index of suspicion of ectopic kidneys is low due to its rare occurrence and vague presentations.
The most common signs and symptoms related to an ectopic kidney that lead to diagnosis include urinary tract infections, abdominal pain or a lump that can be felt in the abdomen (Gulsum et al., 2000). The risk of hydronephrosis may be increased in renal ectopia due to malrotation of the kidney and anteriorly placed renal pelvis leading to impaired urinary drainage (Cinman et al., 2007). The majority of individuals are asymptomatic and informed of the anomaly on incidental discovery during imaging for other pathologies. Individuals can however present with a lump, abdominal or back pain and are prone to vesico-ureteric reflux and therefore infections as well as stones [11]. In severe cases of anatomical or organ dysfunction, surgical intervention is required posing challenges of its own [4].
However, if a non-functioning kidney is discovered with atrophic renal parenchyma, it is justified to perform a primary nephrectomy. Although the ectopic kidneys may be nonfunctional, cases of lithiasis or formation of renosigmoid fistulae have been reported in relation to a pelvic kidney. In such cases nephrectomy forms the choice of treatment, an effort to save the kidney being made only if the kidney is found to be functioning normally [1].
Ectopic kidney case reports in Nigeria
Ekrikpo et al., [3] reported a case of a 38-year-old Nigerian female with a left intrathoracic ectopic kidney and markedly elevated blood pressure leading to renal failure, second report after Ogunbiyi in 1986.
Ilah et al., [5] reported the second ectopic kidney in neonates; and the first ectopic pelvic kidney in neonates in North Western Nigeria, after Samaila and Shaib in 2010.
Okunade et al., [10] reported a giant hydronephrotic pelvic kidney mimicking an ovarian cyst in a 34-week pregnancy. First of such cases in Nigeria and African Journals.
Case Presentation
A 17 years old who presented at the hospital as a case of referral from a traditional birth attendant place, on account of colicky abdominal pain which was initially at the umbilicus before becoming localized to the right iliac fossa, on and off over a year but later became generalized with associated high grade fever and anorexia. There was associated urinary frequency, urgency and dysuria. There was no history of vomiting, abdominal distention or diarrhea as well as obstructive urinary symptoms.
Examination carried out revealed a patient in painful distress, restless, mildly pale, febrile, anicteric, moderately dehydrated with no pitting pedal edema. He had a blood pressure of 110/70 mmHg and his pulse rate was 100 beats per minute, regular and with full volume. The abdomen was full, with generalized tenderness and a palpable tender mass at the umbilicus and right lower quadrantt. Abdominal ultrasound scan done revealed peritonitis secondary to ruptured acute appendicitis with pelvic abscess. Laboratory investigations revealed a full blood count showing high white blood cell count predominantly leukocytosis, normal serum electrolytes, urea and creatinine, and urine microscopic findings (Table 1). He was rigorously resuscitated with intravenous crystalloids, antibiotics with urine output used to check for adequacy of resuscitation and worked up for exploratory laparotomy with grouping and cross matching of a pint of blood as soon as he stabilizes.
He had exploratory laparotomy after 8 hours of resuscitation with intra - operative finding of a ruptured appendix with abscess at the right iliac fossa. The appendix was excised, base transfixed and abscess drained. A mid-line mass was identified within the mesentery of the ileum which was exposed revealing the right kidney normal looking with arterial supply coming from anterior aspect of the abdominal aorta. The kidney was left back as it was looking normal both in appearance and size. Copious abdominal lavage was done with abdominal drain left behind. Wound was closed in layers and dressings applied.
Post-operative period was uneventful with wound drain removed on the 5th day post operatively and patient discharged home on 9th day post operatively. The patient was seen on regular follow-up and he has remained healthy with normal blood electrolytes, urea and creatinine till date.
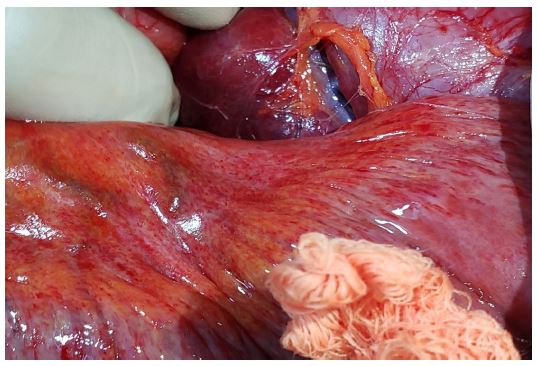
Figure 1: Pelvic ectopic kidney after exposure of messentary (intra-operative finding).

Figure 2: Pelvic ectopic kidney with the messentary (intra-operative finding).
Table 1: The course of endoscopic treatments.
| S/N | Test | Result | Reference range |
|---|---|---|---|
| 1 | Complete bloodcount | ||
| Haemoglobin | 13 | 12-15 g/dL | |
| Packed Cells Volume | 36 | 35-44% | |
| White cells count | 6 | 5.6-16.9 X 109 /L | |
| Platelet count | 250 | 146-429 X 109 /L | |
| 2 | Electrolytes, blood urea and creatinine | ||
| Urea | 6.1 | 3-11 mg/dL | |
| Creatinine | 0.53 | 0.4-0.9 mg/dL | |
| Electrolytes | Within normal ranges | ||
| 3 | Urine microscopy | No growth after48 hours of incubation | |
Discussion
The majority of individuals are asymptomatic and informed of the anomaly on incidental discovery during imaging for other pathologies. Individuals can however present with a lump, abdominal or back pain and are prone to vesicoureteric reflux and therefore infections as well as stones [11]. Okunade et al., [10] reported the first case of a huge hydronephrotic kidney mimicking an ovarian cyst in a 34 weeks pregnancy in Nigeria which was not symtomatic except for an elevated blood pressure which can occur in pre-eclampsia. This was the case in the index patient as the pelvic kidney was misdiagnosed for an abscess due to the presence of a ruptured appendix and absence of symptoms.
According to Muthiah et al. [8], ectopic kidney are commoner on the left which was not the case in this index patient. In severe cases of anatomical or organ dysfunction, surgical intervention is required posing challenges of its own [4] but nephrectomy was not done in this case as it appears normal in shape and size couple with electrocyte, urea and creatinine being normal.
Conclusion
Ectopic pelvic kidney is a rare occurrence and therefore error in its diagnosis may have significant health consequences for the patient. One needs to be careful when dealing with mass lesions of the abdomen in suspected abscess collection and thus pelvic kidney should be a differential diagnosis. A high index of suspicion is required coupled with the involvement of an experienced sonologist to making accurate diagnosis in presence of abdominal mass as it may be asymptomatic. Further imaging such as computerized tomography or magnetic resonance imaging may sometimes be necessary in highly specialized centres to assist the clinician in making the correct diagnosis prior to instituting any surgical intervention.
References
- Belsare SM, Chimmalgi Mamata, Vaidya SA, Sant SM. Ectopic kidney and associated anomalies: A case report. 2002; 51: 236-238.
- Bergman RA, Afifi AK, Myauchi R. In: Illustrated Encyclopedia of Human Anatomic Variation. OPUSA IV: Organ System Urinary System: Kidney, Ureters, Bladder and Urethra. 2014.
- Ekrikpo Udeme, Effa Emmanuel, Akpan Effiong. Case Report Ectopic Thoracic Kidney and End-Stage Renal Disease in a 38-Year-Old Nigerian Academic Editors: S. Case Reports in Nephrology. 2013.
- Healy KA, Margules A, Kundavaram C, Hubosky SG, Lallas CD. Laparoscopic pelvic nephrectomy: essential preoperative and intraoperative considerations. Can J Urol. 2012; 19: 6299-302.
- Ilah Bilkisu Garba, Sakajiki Aminu Muhammad, Aghadueki Smart, Bassey Edem, Kolawole Taofik, Adeniji Akeem Oladiran, Ectopic pelvic kidney in a neonate in Gusau, Zamfara, North Western Nigeria. Sahel Medical Journal. 2015; 18: 89-90.
- Macksood MJ, James RE Jr. Giant hydronephrosis in ectopic kidney in a child. Urology. 1983; 22: 532-5.
- Malek RS, Kelalis PP, Burke EC. Ectopic Kidney in Children and Frequency of Association with Other Malformations. Mayo Clinic Proceedings. 1971; 46: 461-467.
- Muthiah M, Arun K, Bilo D, Adithys M. A case series study of ectopic kidneys. Indian J Med Case Rep. 2013; 2: 52 6.
- Norman S, Christopher JK, Ronan O, Connel P. The Kidneys and Ureters. Bailey and Love’s Short Practice of Surgery. 25th edn. Hodder Education, UK. 2008: 1286-1287.
- Okunade KS, Sekumade A, Sajo A, Daramola E, Okojie O, Ojewola RW, et al. A giant hydronephrotic pelvic kidney mimicking an ovarian cyst in a 34- week pregnancy. Int J Med Biomed Res. 2016; 5: 57-60.
- Pal Dilip, Jain Pritesh, Banerjee Manju. Bilateral Pelvic Kidneys: A Rare Anomaly. Journal of Case Reports. 2016; 6: 411-414.
- Reddy Chandu, Syed N, Namani Namani, Phukon Jewel, Dutta Rajib, Sunitha P, et al. Left ectopic kidney with non rotation: a case report. Nepal Medical College journal: NMCJ. 2010; 12: 123-4.
- Rizvi Ela, Charokar Kailash, Jain Ajay. Ectopic lumbar kidney: a rare presentation. International Surgery Journal. 2018; 5: 3410.
- Sakamoto K, Kojima Y, Takeda R, Terai K, Matsuda M. Solitary pelvic kidney encountered during laparoscopic colectomy. J Minim Access Surg. 2005; 1: 133-5.
- Shapiro Ellen, Bauer Stuart, Chow Jeanne. Anomalies of the Upper Urinary Tract. 2012.
- Williams PL, Bannister LH, Warwick R, et al. Embryology & Development, Urinary System in “Gray’s anatomy,” 38th Ed, Churchill Livingstone, London, UK. 1995; 199-204.
