
Open Access, Volume 11
EBV encephalitis in an immunocompetent adult with hypoplastic left heart syndrome: A case report
Russell Levi1; David Rubin1; Christina De Lisi2*
1Rowan University School of Osteopathic Medicine, Stratford, NJ, USA.
2Department of Family Medicine, Ocean University Medical Center, Brick, NJ, USA.
Christina De Lisi
Department of Family Medicine, Ocean University Medical Center, Brick, NJ, USA.
Email: christina.delisi@hmhn.org
Received : December 17, 2024,
Accepted : January 14, 2025
Published : January 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: EBV is a rare cause of encephalitis which can present with a broad spectrum of focal and diffuse neurological symptoms. In immunocompetent patients, prompt diagnosis can be difficult, especially in the context of comorbid conditions with similar symptomatology.
Case presentation: We present a case of an immunocompetent 21-year-old male with EBV infection and hypoplastic left heart syndrome presenting with focal neurological deficits. CT Code Stroke Head and follow-up MRI revealed no acute ischemic changes or bleeds, and EBV IgM and EBV VCA titers were positive. The patient received supportive care in the ICU and fully recovered after four days.
Conclusion: We highlight the importance of broad differentials and workup in immunocompetent patients presenting with multiple risk factors for thromboembolism and encephalitis.
Keywords: EBV encephalitis; Immunocompetent adult; Focal neurological deficits; Hypoplastic left heart syndrome; Case report.
Abbreviations: EBV: Epstein-Barr Virus; CMV: Cytomegalovirus; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; US: Ultrasound; ICU: Intensive Care Unit; VCA: Viral Capsid Antigen; NIHSS: National Institute of Health Stroke Scale; ED: Emergency Department.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © De Lisi C (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Levi R, Rubin D, De Lisi C. EBV encephalitis in an immunocompetent adult with hypoplastic left heart syndrome: A case report. Open J Clin Med Case Rep. 2025; 2319.
Introduction
Encephalitis is a broad diagnosis describing parenchymal inflammation of the brain presenting with many focal and diffuse symptoms. The underlying cause of encephalitis can stem from autoimmune, paraneoplastic, metabolic, or infectious pathologies with viral encephalitis being the most common form worldwide [1,2]. Epstein-Barr Virus (EBV) is a highly prevalent herpes virus seen in 90% of adult patients worldwide which has a variety of presentations in both immunocompetent and immunocompromised patients.
The common constellation of EBV includes systemic symptoms such as fever, sore throat, fatigue, malaise, tender lymphadenopathy, and splenomegaly [3,4]. Additionally, EBV can also arise with system-specific pathologies such as malignancies (Primary Central Nervous System Lymphoma, Burkitt Lymphoma, etc.), autoimmune disorders (Systemic Lupus Erythematosus, Rheumatoid Arthritis, Multiple Sclerosis), and neurological infections (meningitis, encephalitis), especially in immunocompromised patients [5-7]. In immunocompetent patients; however, EBV encephalitis is responsible globally for only 0.5-7.5% of cases [8].
Here, we present a case of an immunocompetent 21-year-old male presenting with focal neurological deficits in the context of EBV encephalitis vs. embolic stroke from a hypoplastic left heart.
Case Presentation
A 21-year-old male patient presents to the emergency department with chief complaint of dysarthria with left arm and left leg numbness and tingling. Patient has a past medical history of hypoplastic left heart syndrome status post Fontan palliation and early cirrhosis confirmed on liver biopsy, and current diagnosis of infectious mononucleosis status post medrol dose pack and augmentin. At the time of presentation, his vitals include a blood pressure of 143/67 mmHg, a pulse of 92 bpm, a temperature of 98.2℉, a respiratory rate of 17 breaths per minute, and an SpO2 of 95% on room air.
In the ED the patient denied any current symptoms and the physical exam was negative for any acute neurological findings with an NIHSS of 0. The patient’s parents at bedside endorsed dysarthria prior to arriving in the ED. A code stroke was initiated in the ED and a CT Head and CT angiogram were taken, both with unremarkable findings (Figures 1 & 2). Shortly after, the patient experienced another episode of dysarthria lasting for less than five minutes, to which a second code stroke was called and a perfusion CT was taken, showing increased Tmax in the left occipital lobe (Figure 3). Patient was transferred to the ICU for tenecteplase administration and observation with serial neurovascular checks and consults from neurology, cardiology, infectious disease.
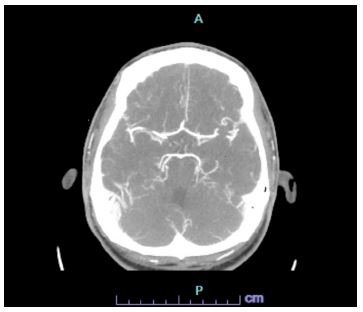
Figure 1: CT head.
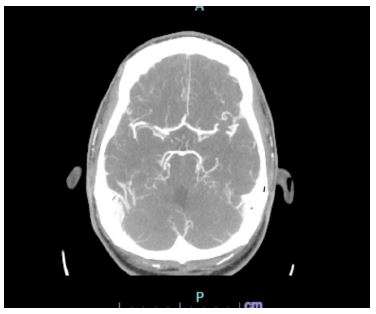
Figure 2: CT angio.

Figure 3: CT perfusion neuro.
While in the ICU, the patient improved and did not have any further acute neurological events. Initial lab work on presentation showed normal CMP and troponins, and was pertinent for atypical lymphocytes, transaminitis. Daily labs showed a mild thrombocytopenia, improvement in the transaminitis, a normal urinalysis, and a negative urine drug screen. Daily labs on the date of discharge showed a mild thrombocytopenia and transaminitis. Neurology recommended an EEG which showed mild diffuse slowing with asymmetry and an MRI which showed no acute infarct or hemorrhage, midline shift, mass effect or evidence of acute ischemic stroke (Figure 4). Infectious disease recommended empiric vancomycin, ceftriaxone and acyclovir and virology was done confirming a positive EBV infection. Due to the patient’s symptomatic improvement, lumbar puncture was not done. Cardiology recommended 2D-echocardiogram with bubble study to rule out embolic stroke which showed a normal cardiac status. Gastroenterology was consulted due to mild transaminitis likely secondary to infectious mononucleosis and recommended a RUQ ultrasound, showing a 4 cm echogenic lesion in the right lobe (Figure 5). Over the course of the patient’s admission in the ICU, the patient did not endorse any neurological or cardiac complaints, reporting only a mild headache and vomiting with normal serial neurological exams.
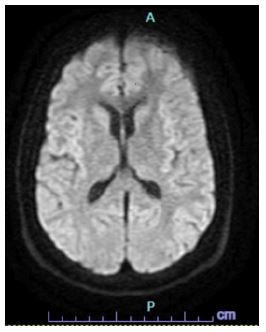
Figure 4: MRI.

Figure 5: RUQ Us.
Based on the normal brain imaging, normal echocardiogram, and positive EBV virology, the most likely etiology of the patient’s focal neurological symptoms was EBV encephalitis. Patient was discharged on day 4 post-admission from the ICU with enalapril 5 mg and aspirin 81 mg and instructions to follow up with his primary physician.
Discussion
EBV encephalitis is a known, yet rare type of viral encephalitis responsible globally for 0.5-7.5% of encephalitis cases in immunocompetent patients [8]. The pathogenesis of EBV encephalitis is unclear, with some sources claiming that it infects lymphocytes which penetrate the blood-brain barrier [9]. Other sources claim that it infects neurons directly, causing lytic cycles which damage and infect surrounding neurons [10]. Symptoms of EBV encephalitis are complex and non-specific, ranging from diffuse neurological deficits of confusion, headache, and seizure, to focal deficits of weakness, ataxia, and dysarthria. When seen with comorbid conditions, the breadth of differentials and complexity of patient presentation add to the difficulty of diagnosing EBV encephalitis. Here, we present such a case of an immunocompetent patient diagnosed with both Hypoplastic left heart syndrome and encephalitis secondary to EBV infectious mononucleosis.
Infectious mononucleosis is a common, self-limited systemic viral illness seen in adolescents and young adults, mostly secondary to EBV with CMV also being seen in immunocompromised patients. The classic constellation of symptoms includes splenomegaly, fever, pharyngitis, and widespread lymphadenopathy, however more insidious symptoms can be present, obscuring a standard clinical picture [4]. As there is no standard diagnostic approach to diagnosis, clinical signs, viral serologies, and heterophile antibody assays are utilized. Currently, EBV serology (anti-VCA IgM, anti-VCA IgG) presents as the most reliable diagnostic tool, with Complete Blood Counts (CBC) with differential and the monospot test having low specificity [11].
Treatment of EBV infectious mononucleosis is mainly supportive, with corticosteroids being used off-label to manage airway obstruction, massive splenomegaly or hemolysis [11,12]. While antivirals were utilized in our patient, multiple studies have shown conflicting data in their use and they are not the current standard of treatment. Osamu Usami et al. show the use of acyclovir in cases of suspected infectious mononucleosis significantly lowered the length of fever [13]. However, Huili Hu et al., showed no significant effects of ganciclovir or acyclovir on disease duration or complications compared to patients not receiving any antiviral medication [14]. Overall, the current literature does not support the use of antivirals for EBV infectious mononucleosis with no current therapies approved for use [15].
Additionally, special consideration in patients with hypoplastic left heart syndrome should be noted. Hypoplastic left heart syndrome induces a state of impaired cardiac function and output, increasing the risk of infection and thromboembolism [16]. As such, in patients suffering from an acute viral illness which has been posited to spread hematogenously through circulating lymphocytes which cross the blood brain barrier, the potential for encephalitis may be increased due to an altered immune response and is worth considering in patients with hypoplastic left heart syndrome [17].
Conclusion
Our case highlights a rare presentation of focal neurological deficits secondary to EBV encephalitis in an adult patient with comorbid hypoplastic left heart syndrome. Since both pathologies induce hypercoagulable states and are rare causes of thromboembolism, physicians should keep in mind a broad set of viral and ischemic differentials and initiate prompt workup of both.
Declarations
Acknowledgement: We thank the patient for giving us consent to publish this case report.
Statement of ethics: Informed consent was obtained from the patient’s mother with consent from the patient.
Conflict of interest statement: The authors have no conflicts of interest to disclose.
Funding sources: This study was not supported by any sponsor or funder.
Author contributions: Conceptualization: R.L., C.D; Drafting: R.L., D.R; Review and Editing: R.L., D.R; Citations: R.L., DR; Oversight and guidance: C.D.
Data availability statement: All data generated are presented in the case report and the online supplementary information. Further inquiries can be directed to the corresponding author.
References
- Bloch KC, Glaser C, Gaston D, Venkatesan A. State of the Art: Acute Encephalitis. Clin Infect Dis. 2023; 77: e14-e33.
- Costa BKD, Sato DK. Viral encephalitis: a practical review on diagnostic approach and treatment. J Pediatr (Rio J). 2020; 96: 12-19.
- Houldcroft CJ, Kellam P. Host genetics of Epstein-Barr virus infection, latency and disease. Rev Med Virol. 2015; 25: 71-84.
- Sylvester JE, Buchanan BK, Silva TW. Infectious Mononucleosis: Rapid Evidence Review. Am Fam Physician. 2023; 107: 71-78.
- Patel PD, Alghareeb R, Hussain A, Maheshwari MV, Khalid N. The Association of Epstein-Barr Virus with Cancer. Cureus. 2022; 14: e26314.
- Robinson WH, Younis S, Love ZZ, Steinman L, Lanz TV. Epstein–Barr virus as a potentiator of autoimmune diseases. Nature Reviews Rheumatology.2024; 20: 729–740.
- Peuchmaur M, Voisin J, Vaillant M, Truffot A, Lupo J, Morand P, et al. Epstein-Barr Virus Encephalitis: A Review of Case Reports from the Last 25 Years. Microorganisms. 2023; 11: 2825.
- Pandey N, Chawala A, Kandhi S, Dhallu M, Chilimuri S. Epstein-Barr virus encephalitis presenting as acute disseminated encephalomyelitis: A challenging diagnostic dilemma. Cureus. 2023.
- Srifuengfung G, Suppakitjanusant P, Chaisrimaneepan N. EBV-Associated CNS Infection in an Immunocompetent Adult: A Case Report and Literature Review. 2024.
- Jha HC, Mehta D, Lu J, et al. Gammaherpesvirus infec-tion of human neuronal cells. MBio. 2015; 6: e01815-e01844.
- Kimberlin DW. Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition. American Academy of Pediatrics. 2024.
- Rezk E, Nofal YH, Hamzeh A, Aboujaib MF, AlKheder MA, Al Hammad MF. Steroids for symptom control in infectious mononucleosis. Cochrane Database Syst Rev. 2015; 2015: CD004402.
- Usami O, Saitoh H, Ashino Y, Hattori T. Acyclovir reduces the duration of fever in patients with infectious mononucleosis-like illness. Tohoku J Exp Med. 2013; 229: 137-42.
- Hu H, Deng H, Bi J, Xu Y, Li S, Xie Y, et al. Clinical characteristics and effectiveness of antiviral agents in hospitalized children with infectious mononucleosis in China: A multicenter retrospective study. Pediatr Investig. 2021; 5: 188-194.
- Andrei G, Trompet E, Snoeck R. Novel Therapeutics for Epstein⁻Barr Virus. Molecules. 2019; 24: 997.
- Feinstein J, Benson D, Dubin A. et al. Hypoplastic Left Heart Syndrome: Current Considerations and Expectations. JACC. 2012; 59: S1–S42.
- Anderson BR, Ciarleglio AJ, Krishnamurthy G, Glied SA, Bacha EA. Neonatal hypoplastic left heart syndrome: Effects of bloodstream infections on outcomes and costs. The Annals of Thoracic Surgery. 2015; 99: 1648–1654.
