
Open Access, Volume 11
Comparative analysis of full arch implant impressions using photogrammetry vs conventional approaches
Tom Murphy1; Waqar Ahmed2; Fadi Barrak1,3*
1School of Medicine and Dentistry, University of Central Lancashire, UK.
2School of Mathematics and Physics, University of Lincoln, UK.
3VSS Ltd, UK
Fadi Barrak
School of Medicine and Dentistry, University of Central Lancashire, & VSS Ltd, UK.
Email: fnbarrak@uclan.ac.uk
Received : December 11, 2024,
Accepted : January 13, 2025
Published : January 15, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: For older patients’ full arch dental implant rehabilitation is a viable solution, eliminating the need for removable of dentures. The registration of implant positions relies on conventional impression materials, involving implant impression posts, open trays, and dental stone models. The restoration of full arch implant-supported prostheses is costly, time-intensive, and inaccurate. Inaccuracies compromise prosthesis passivity, potentially leading to crestal bone loss, and prosthesis or implant failures. This is relevant following full arch dental implant surgery, due to significantly reduced bone volume following vertical alveoloplasty, meaning further revision surgery may not be possible.
Aims and objectives: This review compares the accuracy of conventional polyether or polyvinyl siloxane dental implant impressions with commercially available photogrammetry units. It also investigates potential differences in patient or clinician satisfaction.
Materials and methods: Three major databases (DoSS, MEDLINE, and EMBASE) were searched through electronically and manually, retrieving articles up to June 6, 2023. MeSH terms and keywords with Boolean connectors were employed, supplemented by a grey literature exploration using Google Scholar. The identified studies underwent screening via abstracts, or full texts when necessary, and final data extraction followed.
Results and discussion: Five articles meeting inclusion and exclusion criteria were retrieved, with two in vivo studies and three in vitro studies. These comprised three case-control trials, one controlled clinical trial, and one randomized controlled trial. Concerning the accuracy of photogrammetry, two studies highlighted comparable or superior accuracy compared to conventional impressions. Two studies concluded that photogrammetry displayed lower accuracy than conventional impressions. One study found no clinically significant deviations between the two methods in terms of implant success or marginal bone loss but did note a significant improvement in patient and clinician outcomes.
Conclusion: Photogrammetry impressions is a promising alternative to conventional impressions, showing improved patient and clinician satisfaction while exhibiting comparable or enhanced accuracy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Barrak F (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Murphy T, Ahmed W, Barrak F. Comparative analysis of full arch implant impressions using photogrammetry vs conventional approaches. Open J Clin Med Case Rep. 2025; 2318.
Introduction
With a steadily aging population, it’s not surprising that 69% of individuals are missing at least one tooth, and 2.6% are completely edentulous, experiencing further tooth loss as they age [1]. Advances in medicine, leading to increased life expectancy, contribute to a growing number of people grappling with varying degrees of edentulism. Consequently, many are turning to dental implants as a preferred alternative to partial or complete dentures.
The historical pursuit of replacing teeth dates back to 2500 BC, where golden wire was used to splint teeth, followed by the first recorded “dental implant” in 600 AD when the Mayan population implanted shells into the dental alveolar bone to mimic teeth [2]. As human civilization has progressed, so too have dental implants, with root form dental implants emerging as a well-established treatment for over 50 years, boasting a commendable survival rate of 95.6% at 5 years [3,4].
Essentially, a dental implant is a structure implanted under the gingiva and into the alveolar bone, providing support for a dental prosthesis. The process of placing multiple dental implants in an edentulous arch and connecting them with an implant-retained bridge is known as full arch dental implant treatment (Figure 1). Traditionally, to capture the 3D relationship of multiple dental implants across a patient’s dental arch, dentists would employ elastomeric materials (PVS/Polyether) to take impressions of implant impression posts—metal posts screwed into the implants to record their position [5]. Following the impression, a stone model is crafted, incorporating implant analogues (extra-oral copies of the implants placed in the stone model) and a confirmation jig (a multi-piece tool verifying the accuracy of the master model before framework manufacture). This meticulous process ensures passivity [7]. As we explore the evolution of dental implant techniques, it becomes evident that the journey from ancient practices to contemporary methods has significantly improved the options available for individuals seeking effective tooth replacement solutions.
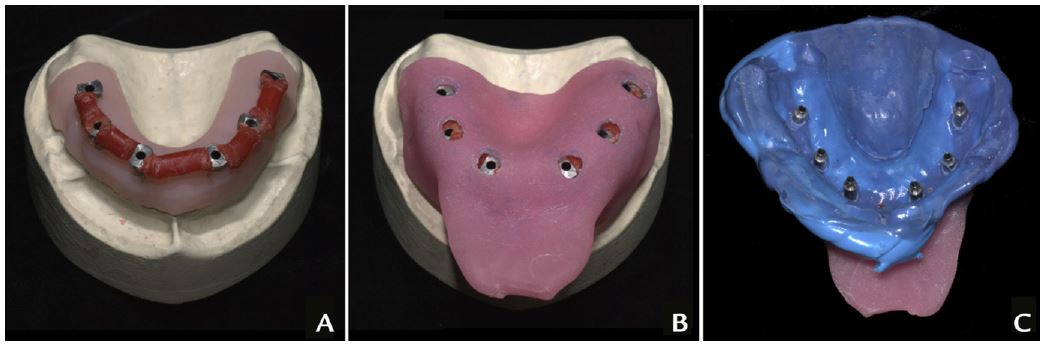
Figure 1: Conventional Full Arch Implant Impressions: A) Implant impression posts splinted together with pattern resin, B) A customised open tray impression is taken, C) The intaglio surface of the impression with impression posts visible Image courtesy of Knechtle et al., [6].
Considering the crucial aspect of prosthesis (bridge) passivity—how well the bridge fits against its opposing components, specifically multi-unit abutments—it becomes evident that optimal passivity involves the bridge fully seating across the entire arch without any gaps or tension. In contrast, poor passivity manifests when the prosthesis doesn’t fully seat at the abutment interface or experiences tension during torquing down.
The significance of prosthesis passivity lies in its impact on the proper fit of the bridge against opposing components. A bridge with good passivity ensures a seamless fit, eliminating any potential gaps and tension. Conversely, bridges with poor passivity may result in improper seating and lateral torquing forces on the implants and components during the torquing down process. This aspect underscores the importance of meticulous attention to detail during the fitting of bridges, as poor passivity can lead to adverse consequences. Figure 2 shows the implant superstructure with poor passivity and gaps at abutment interface and implant superstructure with good passivity at abutment interface.
Understanding the critical role of prosthesis passivity is essential, given that bridges with inadequate passivity can induce pain, contribute to bone loss at the crestal margin, and even jeopardize osseointegration, ultimately leading to implant loss [8]. Therefore, emphasizing and ensuring prosthesis passivity in the bridge superstructure is not only a matter of precision but also a safeguard against potential complications that could compromise the overall success of the implant treatment.
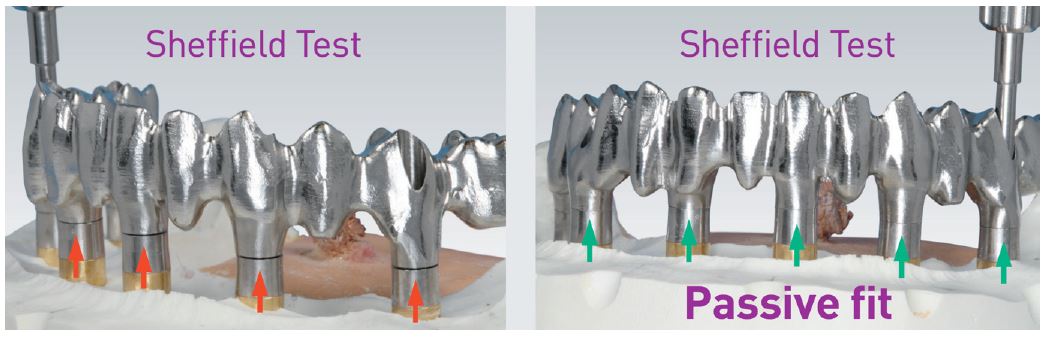
Figure 2: Implant superstructure with poor passivity and gaps at abutment interface (Left) and implant superstructure with good passivity at abutment interface (Right) (Image courtesy of Mueller, 2023).
Understanding the critical nature of prosthesis passivity in full arch dental implant patients is essential, particularly considering the limited alternative options available in the event of implant bridge failure. During full arch surgery, vertical alveoloplasty is often necessary, involving the removal or profiling of alveolar bone to enhance implant placement [11]. However, this procedure may leave limited or no remaining bone suitable for replacing a failed dental implant. Consequently, poor implant bridge passivity, stemming from inaccurate impressions, could potentially lead a patient to rely on a denture if implant failure occurs. To advance dental implant treatment, exploring novel technologies that enhance precision, accuracy, and efficiency in implant registration becomes imperative.
Conventional restoration of full arch dental prostheses presents its own challenges - being expensive, time-consuming, and prone to inherent inaccuracies. Issues such as high material and lab fees, extensive chairside and lab time, and inaccuracies during impression-taking and model-making due to errors or shrinkage collectively introduce inaccuracies into the prosthesis, impacting implant prosthesis passivity [8].
With a global placement of up to 300,000 implants annually [9], poor prosthesis passivity poses a widespread problem for both patients and clinicians, necessitating the exploration of methods to address this issue.
An innovative approach to the impression and registration stage is photogrammetry, a well-known process in medicine and radiology, now making strides in dentistry. In dental photogrammetry, a calibrated stereoscopic camera, paired with geometric/topographic implant scan markers, determines the 3D spatial arrangement of dental implants. This process is reported to be highly precise, reproducible, and significantly more time and labor-efficient than conventional impressions [12]. Following this, an impression of the peri-implant soft tissues, using either analog or digital techniques, forms the basis for fabricating the implant bridge.
As early as 1999, Jemt showcased the use of photogrammetry to capture implant positions in the edentulous jaw, demonstrating its accuracy on par with conventional techniques [13]. Recent works, such as Hussein [14], affirm the ongoing validity of photogrammetry in dentistry.
Early methods of dental photogrammetry involved DSLR cameras with wide-angle lenses capturing images reflected in parallel mirrors. However, issues such as time consumption, data standardization, image quality, and reproducibility in a clinical setting led to advancements. Notably, purpose-built photogrammetry units like the iCam4D (Imetric 4D) and the PIC camera (PIC) have gained prominence (Figure 3). Both units, designed for intra-oral implant 3D positioning, utilize sophisticated technology—iCam4D employs four cameras, a photo projector, and calibrated scan bodies, while the PIC camera is a commercially available photogrammetry unit using structured light to determine implant position. In the modern review of photogrammetry, only purpose-built units will be considered, as technology has evolved significantly beyond the limitations of early DSLR-based methods [15].

Figure 3: iCamBody scan markers (Left) and an iCam4D photogrammetric device (Right) [16].
The PIC camera employs two charged coupled devices along with a paired infrared flash, mirroring the setup of the iCam4D. Like its counterpart, the PIC camera is equipped with paired scan bodies, known as PIC transfers (Figure 4). Impressively, the PIC camera can capture 150 frames per minute, pinpointing the positions of PIC transfers with an error margin of less than 10 μm. However, a notable distinction arises as the PIC transfers lack metallic properties, making it more challenging to confirm their proper seating radiographically.

Figure 4: PIC transfers (Left) and PIC Camera photogrammetric device (Right) [17].
When assessing the utility of photogrammetry as a tool in implant dentistry, it’s essential to juxtapose it against the limitations of conventional methods. The evaluation of accuracy in both trueness and precision is paramount, aligning with the International Organization for Standardization - ISO 5725 guidelines (ISO, 2020). Trueness signifies the ability to replicate implant positions in their true 3D orientation without alterations, while precision measures how closely the impression can capture and reproduce these positions across multiple scans without deviation in 3D orientation. Additionally, considering both patient and dentist satisfaction with photogrammetry versus conventional methods, along with the time taken to produce finalized digital impressions, is crucial for a comprehensive comparison.
The literature review underscores the evident repercussions of impression inaccuracies on the final prosthesis. Such inaccuracies can compromise prosthesis passivity, diminishing the long-term prognosis of the supporting dental implants [8].
This review aims to scrutinize conventional full arch implant impressions against those taken with a photogrammetry device. Specifically, the study seeks to unveil any significant differences in terms of accuracy (precision and trueness) between conventional and photogrammetric impressions, directly impacting the fit and passivity of the final prosthesis. Additionally, the study endeavours to discern potential variations in patient and clinician satisfaction associated with the two impression types.
The aspiration is that by gathering this knowledge, clinicians can enhance their standard operating procedures, ultimately leading to improved patient outcomes and heightened satisfaction for both clinicians and patients alike.
Methods
The study was registered in the International Prospective Register of Ongoing Systematic Reviews (PROSPERO), adhering to the guidelines outlined by the preferred reporting items for systematic reviews and meta-analysis (PRISMA) with the registration number CRD42023447558.
This systematic review aims to evaluate the accuracy of photogrammetry digital impressions for full arch dental implant positions in comparison to conventional methods. The focus will be on deviations related to implant angulation, spatial distances, and feedback from both clinicians and patients.
The inclusion criteria, shaped by the PICO framework, specify that Participants (P) must be undergoing full arch implant treatment or be fabricated models of edentulous dental arches. The intervention (I) under consideration is the use of photogrammetry as an alternative to the Comparator (C), specifically PVS/Polyether (PE) impressions concerning the implants or implant analogues. The measured Outcome (O) encompasses the accuracy of the implant impression, as well as clinician and patient satisfaction.
Articles considered for inclusion were those published after 2010 and in English, falling into the categories of Randomised Controlled Trials (RCTs), Systematic Reviews, Case Studies, or Case Series. Exclusion criteria were applied to articles not meeting eligibility standards, including those published before 2010, letters to the editor, textbooks, or online articles. Additionally, publications lacking full mouth implants (single or partial jaw) or utilizing an incorrect comparator (e.g., plaster) were excluded. The alignment of inclusion and exclusion criteria with the PICO framework and the overarching research question ensures a targeted and comprehensive approach to assessing the accuracy and satisfaction aspects of photogrammetry in full arch dental implant impressions (Table 1).
Table 1: PICO Framework with inclusion and exclusion criteria.
| Inclusion criteria (basedon PICO framework) | Exclusion criteria (basedon PICO framework) | |
|---|---|---|
| Population | Patients thatare receiving fullarch implants | Patients that are not receiving full arch implants (single implants/ conventional dental restorations. |
| Studies usingmodels/analogues of fullarch implants | Studies usingmodels/analogues of single/partial arch implants | |
| Intervention | Full ArchPhotogrammetry Scanning | Intraoral Scanning/DSLR Photogrammetry/Partial arch photogrammetry scanning |
| Comparison | PVS/PE Impressions | Non PVS/PEImpressions (e.g. plaster/alginate/wax/compound/ZOE) |
| Outcome | Precision of implant positioning | Studies notmeasuring precision of implant positioning |
| Language | Studies published in English | Studies thatare not inEnglish |
| Publication Timing | Studies published after 2010 | Studies published before 2010 |
| Publication Type | RCTs, Systematic Reviews, Case Studies, Case Series | Letters to the editor, textbooks online articles. |
The search strategy was executed through UCL an Libraries, utilizing online resources. The databases selected for exploration were MEDLINE, DoSS, and EMBASE. MeSH terms, keywords, and Boolean connectors were employed, along with synonyms of common search terms. A restriction to the English language was applied, and the study timeframe extended from 2010 to June 6th, 2023, excluding potentially outdated technologies. After collating studies, duplicates were meticulously removed within RefWorks, supplemented by manual de-selection. Studies falling outside the specified timeframe or failing to meet inclusion criteria were excluded.
A supplementary manual search was conducted on Google Scholar for grey literature, employing the search terms “Dental Implants” and “Photogrammetry.” Reference chaining from sourced publications further enriched the search. All searches were performed by a single operator over a 10-week period, ensuring consistency
Titles and abstracts of studies were scrutinized, and studies meeting inclusion criteria or requiring further clarification underwent a full-text assessment. Studies that clearly did not meet eligibility criteria were categorized as “unsuitable” within RefWorks. All studies were diligently backed up on an external hard drive.
The Effective Public Health Practice Project (EPHPP) quality assessment tool for quantitative studies was employed to evaluate the risk of bias and study quality. This tool generates a global rating (1 = Strong, 2 = Moderate, 3 = Weak) based on component ratings for Selection Bias, Study Design, Confounders, Blinding, Data Collection Method, and Withdrawals and Dropouts. Given the nature of the review focusing on different types of dental implant impressions, blinding posed challenges in most studies. Despite the inability to fully blind operators and participants, consistency in data collection was observed across studies, while the interpretation of results varied.
Relevant data from selected papers were meticulously recorded in a Microsoft Excel spreadsheet, encompassing details such as Author, Year of Publication, Title of Study, Journal, Aims, Study Design, Location, Archforms Included, Implants per Arch, Captures per Method, Patient/Model/Both, Inclusion and Exclusion Criteria, Ethical Approval, Consent, Null Hypothesis, Recording Method, Comparator, Baseline Comparison, Distance and Angular Deviations, Power Analysis, Accuracy, Precision, and Conclusion. Due to heterogeneity in data recording across studies, not all studies fulfilled the desired complete data sets.
This comprehensive approach ensures a systematic and thorough evaluation of the literature, considering various sources and employing robust quality assessment tools for a nuanced understanding of the topic.
Results
Figure 5 shows the PRISMA Flow Diagram highlighting the literature searches and paper screening strategy employed in this study. A total of 131 papers were sourced from three databases, coupled with grey literature searches via reference chaining and manual exploration of Google Scholar. The distribution of these papers included 26 from Dentistry and Oral Sciences Source, 37 from EMBASE, 48 from Medline, and an additional 20 from manual searches and reference chaining. To ensure data accuracy, the individual literature searches were meticulously extracted from their respective databases and imported into RefWorks. Subsequently, 45 duplicated papers were identified, thoroughly reviewed with RefWorks’ duplication software, and manually revised before removal.
The remaining set of 86 articles underwent scrutiny during the titles and abstracts screening phase. Out of these, 78 articles were found to clearly not align with the inclusion and exclusion criteria and were consequently removed. The remaining 8 articles were pursued for retrieval, and all 8 were successfully obtained. During the subsequent full-text screening phase, 5 papers fully met the inclusion and exclusion criteria.
Among the 3 papers that did not satisfy the criteria, 1 was excluded due to the use of plaster as a comparator instead of PVS or Polyether impression materials. The other 2 employed DSLR Photogrammetry as the method for recording photogrammetric impressions (Table 2).
Of the 5 accepted studies, 3 were conducted in 2021, 1 in 2023, and 1 in 2017. This meticulous screening and retrieval process ensures that the studies included in the review align with the predefined criteria, providing a robust foundation for the systematic analysis (Tables 2, 3 & 4).
Table 2: Study designs of included studies and photographic method used.
| Study design | Number of studies |
|---|---|
| Randomised controlled trial | 1 |
| Controlled clinical trial | 1 |
| Case – control trial | 3 |
| Photogrammetry device | |
| iCam 4D (iMetric) | 3 |
| PIC camera | 2 |
Table 3: Summary of implant systems used, and implants placed.
| Implant system | Number of studies | No of implants placed |
|---|---|---|
| Straumann | 3 | 18 |
| Nobel | 1 | 78 |
| TiCare | 1 | 131 |
Table 4: Summary of study settings and archforms included.
| Study setting | Number of archforms included |
|---|---|
| In Vivo | 35 |
| In Vitro | 3 |
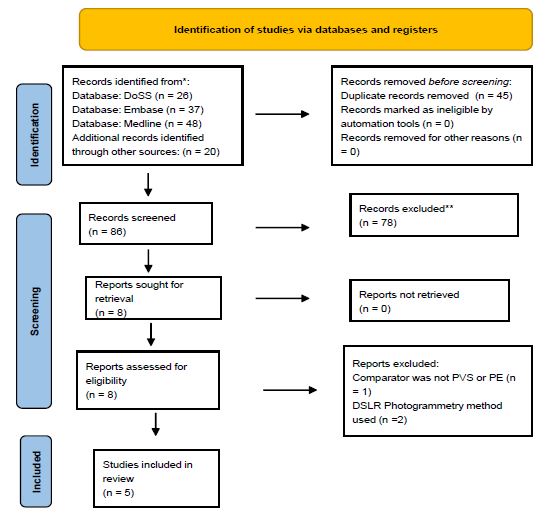
Figure 5: PRISMA Flow Diagram – Highlighting the literature searches and paper screening.
The diverse array of studies included in this systematic review spanned locations in Shanghai, China, the United States of America, and Spain. Among the selected studies, there was a balanced representation of one randomized control trial, one controlled clinical trial, and three case-control trials. Additionally, the studies encompassed both In Vivo and In Vitro settings, with 2 studies falling into the In Vivo category and 3 into the In Vitro category.
In the context of In Vivo studies, full arch dental implants were executed on 20 maxillae and 15 mandibles, each featuring a minimum of 4 and a maximum of 7 dental implants per arch. The capture of dental implant positions occurred once per dental arch across both In Vivo studies. Ethical approval and clear inclusion/exclusion criteria were explicitly stated in both In Vivo studies. Notably, two different implant systems, Nobel and TiCare, were utilized in these studies, with 78 Nobel implants in one study and 131 TiCare implants in the other.
Shifting to In Vitro studies, edentulous dental arch models with implant analogues were employed. These studies used a consistent edentulous model with 6 implants placed. The dental implant positions were captured between 10-15 times in the In Vitro studies, compensating for the reduced number of dental arches included. Notably, none of the In Vitro studies explicitly addressed ethical approval or outlined inclusion/exclusion criteria. Across all four In Vitro studies, the exclusive use of Straumann implants was a common feature, with a total of 18 Straumann implants being utilized.
Two commercially available photogrammetry units, namely the iCam4D and the PIC Camera, were employed across all 5 studies. The iCam4D featured in three studies, while the PIC Camera was used in two studies. Significantly, each photogrammetry unit was utilized in 1 In Vivo study, ensuring a relatively even distribution of implants scanned in both patients and edentulous models across both photogrammetry systems.
A comprehensive risk of bias study was conducted for all included studies. Four studies earned high global ratings, indicating a low risk of bias and were thus included in this review. One study received a low global rating and a high risk of bias due to moderate component ratings linked to selection bias/study design and weak component ratings tied to confounders and blinding. Despite this, the study was included as selection bias was challenging given a small subset of potential participants, and blinding was intricate due to the distinct nature of the variable/control that couldn’t be easily blinded to the operators.
In total, five studies were incorporated into this systematic review, with two being written by the same author. The findings from these studies presented varied perspectives. Two studies highlighted that photogrammetry exhibited comparable or higher accuracy (precision and trueness) when compared to conventional impressions. Conversely, two studies by Revilla-León et al. underscored reduced accuracy (precision and trueness) when compared to photogrammetry. Lastly, one study emphasized the reduced time and increased clinician/patient satisfaction of photogrammetry compared to conventional impressions. This amalgamation of results provides a comprehensive overview of the current landscape of research in this domain.
Summary of studies included
Zhang et al (2021) conducted an in vivo comparative controlled clinical trial to evaluate photogrammetry’s accuracy in recording implant positions for complete mouth implant prostheses. Patients meeting specific criteria underwent the procedure using the iCam4D system for photogrammetry and conventional impressions. The study revealed a mean standard deviation of 70±57 μm for distance deviations, significantly below the 150 μm clinically acceptable limit. Angular deviations were 0.432±0.348 degrees, with 90.8% of implant deviations below 150 μm. While the study had a limited sample size, it provided valuable insights into photogrammetry’s efficacy, despite a high risk of bias.
Ma et al (2021) conducted an in vitro case control study comparing photogrammetry, Iintraoral Scanning (IOS), and conventional impressions for complete arch implant rehabilitation. The photogrammetry group, employing the iCam4D system, exhibited superior trueness and precision compared to conventional and IOS methods. While the study highlighted time considerations, satisfaction, and reduced error with photogrammetry, limitations included the lack of blinding and a relatively small sample size.
Revilla-León et al (2021) explored the accuracy and precision of conventional impressions, photogrammetric impressions, and intra-oral scanners for full-mouth implant impressions in an in vitro case control study. Photogrammetry exhibited higher discrepancies along the y-axis but demonstrated 3D discrepancies of 77.6 μm, prompting a low risk of bias classification with strong ratings in study design and blinding.
In a subsequent in vitro case control study, Revilla-León et al (2023) compared the accuracy, trueness, and precision of full arch dental implant impressions using conventional and photogrammetric methods. The study highlighted a statistically significant discrepancy between the two methods, with the conventional group showing greater accuracy. The study was rated with low risk of bias, considering factors such as study design, blinding, and selection bias.
Peñarrocha-Diago et al (2017) conducted an in vivo randomized controlled pilot clinical trial, comparing patient and dentist satisfaction, working times, and outcomes between photogrammetric and conventional full arch dental impressions. The photogrammetry group demonstrated significantly reduced impression time and higher satisfaction scores. The study exhibited a low risk of bias, offering valuable insights into the clinical benefits of photogrammetry despite potential limitations in accuracy measurement.
In summary, while each study contributes unique insights into photogrammetry’s application in dental impressions, limitations such as sample size, lack of blinding, and potential biases should be considered when interpreting the results. Further research with larger sample sizes and standardized methodologies could enhance the evidence base for the efficacy of photogrammetry in dental implant impressions.
Discussion
The accumulated evidence reveals a consistent pattern indicating that while photogrammetry units effectively capture the 3D positions of dental implants, there is a current limitation in reproducing the soft tissue profile of an edentulous dental arch. This necessitates additional soft tissue impressions, either through an intra-oral scanner or conventional dental impression material, to capture relevant peri-implant soft tissues [19]. Introducing additional impressions may theoretically introduce errors in the final merged file. Conventional impressions may deform, and intra-oral scanners are influenced by factors such as lighting conditions, moisture, color, and scanning distance, potentially introducing errors. The digitization and merging process with photogrammetry data can also introduce inaccuracies [20]. A recent study [21] comparing full arch dental implant impressions found higher accuracy with conventional impressions than intra-oral scanning impressions. However, the impact of these transferred errors on the final full arch prosthesis remains unclear. Notably, the two in vivo studies included in this review found no statistically significant differences in final accuracy, implant success rates, marginal bone loss, or prosthesis survival.
When comparing the accuracy of photogrammetric impressions to conventional impressions, the results from the studies present varying outcomes. Revilla-León et al., two in vitro studies concluded that conventionally splinted impressions had the lowest 3D discrepancies and a statistically significant difference in impression accuracy compared to photogrammetric impressions. In contrast, Ma et al., in vitro study concluded that photogrammetric impressions demonstrated statistically significant improvements in accuracy compared to conventional impressions. Revilla-León et al (2021) highlighted low precision for all impression techniques (PG/CNV/IOS), contrasting with Ma et al’s results that emphasized high precision in the photogrammetry group compared to conventional and intra-oral scanning groups.
In critically evaluating the study results, consideration of the measurement tools is crucial. Revilla-León et al (2021 and 2023) used a coordinate measuring machine, while Zhang et al and Ma et al used laboratory reference scanners to measure accuracy. Differences in accuracy measurement tools, such as the limitations of coordinate measuring machines in detecting complex topography, may have influenced the varying outcomes.
The randomized control trial by Peñarrocha-Diago et al stands out in highlighting the benefits of photogrammetry. Despite additional soft tissue impressions, the overall working time for photogrammetric impressions was less than conventionally splinted impressions. Reduced working time, coupled with increased patient and clinician satisfaction, underscores the positive impact of photogrammetry. This aligns with broader literature, including a meta-analysis [23], showing increased patient satisfaction with digital impressions over conventional impressions. While the high entry cost of digital impressions may be a limiting factor, technological advancements are gradually reducing these costs [24], making digital options more accessible.
Conclusions
Most studies consistently suggest comparable or increased accuracy when comparing photogrammetric impressions to conventional impressions. Notably, there is evidence indicating that an increase in inter-implant distances may impact the accuracy of photogrammetric impressions. Beyond accuracy, photogrammetry demonstrates a notable enhancement in both patient and professional satisfaction compared to conventional impressions. However, it is crucial to acknowledge that photogrammetric impressions alone are unable to capture peri-implant soft tissues. The incorporation of complementary soft tissue scanning could potentially reduce working time and streamline clinical steps. To bolster the findings of this study, there is a clear need for additional research, particularly in vitro studies with larger sample sizes. This will contribute to a more comprehensive understanding and robust support for the assertions made in this study.
Declarations
The manuscript has been submitted solely to this journal and is not published, in press, or submitted elsewhere.
All authors do not have any potential sources of conflict of interest in the manuscript. – see COI forms form each author uploaded.
I confirm that the study has been approved by relevant committee. No human participants were involved in the study. No funding was obtained for the project.
The manuscript has been prepared according to journal’s Author Guidelines.
All the authors have contributed significantly to the manuscript.
References
- Almusallam SM. “The prevalence of partial edentulism and complete edentulism among adults and above population of Riyadh City in Saudi Arabia”. Journal of Family Medicine and Primary Care. 2020; 9: 1868.
- Abraham CM. ‘A brief historical perspective on dental implants, their surface coatings and treatments’, The Open Dentistry Journal. 2014; 8: 50–55.
- Buser D, Sennerby L, De Bruyn H. ‘Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions’. Periodontology. 2000; 73: 7–21.
- Pjetursson BE, et al. ‘A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (fdps) after a mean observation period of at least 5 years’. Clinical Oral Implants Research. 2012; 23: 22–38.
- Baldissara P, et al. ‘Assessment of impression material accuracy in complete-arch restorations on four implants’. The Journal of Prosthetic Dentistry. 2021; 126: 763–771.
- Knechtle N, et al. ‘Accuracy of digital complete-arch, multi-implant scans made in the edentulous jaw with Gingival movement simulation: An in vitro study’. The Journal of Prosthetic Dentistry. 2022; 128: 468–478.
- Ercoli C, et al. ‘The influence of verification jig on framework fit for nonsegmented fixed implant-supported complete denture’, Clinical Implant Dentistry and Related Research. 2011: 14.
- Buzayan MM, Yunus NB. ‘Passive fit in screw retained multi-unit implant prosthesis understanding and achieving: A review of the literature’, The Journal of Indian Prosthodontic Society. 2013; 14: 16–23.
- Gaviria L, et al. ‘Current trends in dental implants’, Journal of the Korean Association of Oral and Maxillofacial Surgeons. 2014; 40: 50.
- Mueller WD. Recognised proof of passive fit - The Sheffield test, Sheffield Test - SAE DENTAL VERTRIEBS GMBH. 2023.
- Misch CE. Prosthetic options in implant dentistry. Int J Oral Implantol. 1991; 7: 17-21.
- Mühlemann S, et al. ‘Is the use of digital technologies for the fabrication of implant-supported reconstructions more efficient and/or more effective than conventional techniques: A systematic review’. Clinical Oral Implants Research. 2018; 29: 184–195.
- Jemt T, Bäck T, Petersson A. ‘Photogrammetry--an alternative to conventional impressions in implant dentistry? A clinical pilot study’. Int J Prosthodont. 1999; 12: 363–368.
- Hussein MO. ‘Photogrammetry Technology in Implant Dentistry: A systematic review’. The Journal of Prosthetic Dentistry. 2021.
- Haines J. Photogrammetry workflow using a DSLR camera, Scholars’ Lab. 2019.
- iMetric4D. iCam4D, Imetric 4D. 2023.
- PIC Dental. Pic Camera, PIC dental. 2023.
- International Organization for Standardization. 2020.
- Molinero-Mourelle P, et al. ‘Photogrammetric and intraoral digital impression technique for the rehabilitation of multiple unfavorably positioned dental implants: A clinical report’. Journal of Oral Implantology. 2019; 45: 398–402.
- Sánchez-Monescillo A, et al. ‘All-on-four rehabilitation using photogrammetric impression technique’. Quintessence Int. 2019; 50: 288–293.
- Husein HA, Morad Mhd L, Kanout S. ‘Accuracy of conventional and digital methods of obtaining full-arch dental impression (in vitro study)’. Cureus. 2022.
- Mizumoto RM, et al. ‘Accuracy of different digital scanning techniques and scan bodies for complete-arch implant-supported prostheses’. The Journal of Prosthetic Dentistry. 2020; 123: 96–104.
- Sivaramakrishnan G, Alsobaiei M, Sridharan K. ‘Patient preference and operating time for digital versus conventional impressions: A network meta‐analysis’. Australian Dental Journal. 2019; 65: 58–69.
- Cicciù M, et al. ‘3D digital impression systems compared with traditional techniques in dentistry: A recent data systematic review’. Materials. 1982: 13.
