
Open Access, Volume 10
Capsule endoscopic features in a severe patient with eosinophilic gastroenteritis: A case report
Phu Pham Quang1,2; Thuan Nghiem Duc2*; Nhuong Duong Xuan1,2; Thuong Nguyen Hoai1; Yen Tran Hai1,2; Hoa Vu Thi2
1Military Hospital 103, Hanoi, Vietnam.
2Vietnam Military Medical University, Hanoi, Vietnam.
Thuan Nghiem Duc
Vietnam Military Medical University, 160 Phung Hung, Ha Dong, Ha Noi, Vietnam.
Email: Thuanbm6@gmail.com
Received : November 05, 2024,
Accepted : December 06, 2024
Published : December 16, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Background: Eosinophilic Gastroenteritis (EGE) is a rare digestive disorder characterized by eosinophilic infiltration of the gastrointestinal tract. In the diagnosis of EGE, it is extremely important to recognize characteristic endoscopic findings and eosinophilia in gastrointestinal tissues. Capsule endoscopy can reveal lesions in the gastrointestinal tract, especially small bowel lesions, which are difficult to access for evaluation. However, the endoscopic findings of EGE in the small intestine are still not well understood.
Case presentation: A 20-year-old Asian man presented with abdominal pain in the right lower quadrant for 1 month, nausea, vomiting, and diarrhea 1-2 times per day. Laboratory studies revealed increased peripheral blood eosinophilia (665/μL; normal range 20-400) and high C-reactive protein (28.8 mg/L). The abdominal CT findings revealed uneven thickening of the ileum and ileocecal angle wall. Multiple areas of erythema, villous atrophy, erosion, ulceration, and edema were detected throughout the small bowel by a capsule endoscopy (MC 2000, Intromedic, South Korea). Anatomopathological examination of the biopsy sample revealed mucosal infiltration of >50 eosinophils per high-power field.
The patient was diagnosed with EGE. We initiated treatment with an infusion of methylprednisolone at a dosage of 40 mg/day. The patient experienced a significant reduction in symptoms after 2 weeks of treatment. The dosage of methylprednisolone was gradually decreased to 15 mg/day. A follow-up capsule endoscopy examination performed 2 months later revealed that there were no mucosal lesions present in the small intestine.
Conclusion: The most common capsule endoscopic findings in our EGE patient were multiple areas of erythema, villous atrophy, erosion, ulceration, and edema throughout the small bowel.
Keywords: Eosinophilic gastroenteritis; Capsule endoscopy; Multiple erythema; Case report.
Abbreviations: EGE: Eosinophilic Gastroenteritis; Eoe: Eosinophilic Esophagitis; HPF: High Power Field.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Nghiem Duc T (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Pham Quang P, Nghiem Duc T, Duong Xuan N, Nguyen Hoai T, Y Tran Hai Y, Vu Thi H. Capsule endoscopic features in a severe patient with eosinophilic gastroenteritis: A case report. Open J Clin Med Case Rep. 2024; 2307.
Introduction
Eosinophilic Gastroenteritis (EGE) is a rare disorder characterized by an abnormal increase in eosinophils in the gastrointestinal tract in the absence of secondary causes of eosinophilia, resulting in gastroenteritis damage and dysfunction [1,2].
The clinical characteristics of Vietnamese patients with EGE have not been fully clarified. Precise knowledge about the clinical features and endoscopic findings of these disorders is crucial for both understanding the pathophysiology and supporting an accurate diagnosis. Compared with other eosinophilic gastrointestinal diseases, EGE is the most challenging to diagnose because of its small intestinal location, which poses a challenge for traditional endoscopy [2].
Capsule endoscopy enables the visualization of lesions in the entire small intestine, suggesting its value in the detection of EGE lesions. However, the capsule endoscopic findings of EGE have been described in only a few reports [3-5]. Therefore, we report a clinical case of eosinophilic enteritis with capsule endoscopy findings and histopathology.
Case Presentation
A 20-year-old male Asian patient without a medical history was admitted to our hospital with abdominal pain in the right lower quadrant for 1 month. He also presented with nausea, vomiting and diarrhea 1-2 times per day. He had no notable family history, including no prior diagnosis of allergic diseases.
Laboratory studies revealed increased peripheral blood eosinophilia (665/μL; normal range 20-400) and high C-reactive protein (28.8 mg/L). Stool examinations were negative for parasites. The abdominal CT findings revealed uneven thickening of the ileum and ileocecal angle wall.
Esophagogastroduodenoscopy and colonoscopy were unremarkable. However, a capsule endoscopy examination (MC 2000, Intromedic, South Korea) revealed multiple erythematous mucosal lesions and villous atrophy, erosion, ulceration, and edema throughout the small bowel. The images of the lesion detected through capsule endoscopy continued continuously from the capsule location at 3 hours 35 minutes to the end of the ileum at 9 hours 4 minutes. Specifically, multiple areas of erythema, villous atrophy, erosion, ulceration, and edema were the most common endoscopic findings in the small bowel (Figure 1). Other findings included mucosal congestion, whitish exudate and short-rounded edematous villi (Figure 1).
Inflammation, erosion, and ulceration were detected by inserting the endoscope through the Bauhin valve and into the ileum. A lesion biopsy was taken for histopathological analysis. Anatomopathological examination of the biopsy sample showed mucosal infiltration of >50 eosinophils per High-Power Field (HPF) (Figure 2). During pathological specimen analysis, the lesion location was determined by looking for eosinophilic infiltration with at least 20 cells per HPF [6]. These findings were consistent with a diagnosis of predominantly mucosal EGE.
Treatment with infusion methylprednisolone at a dosage of 40 mg/day was initiated. The patient experienced a significant reduction in symptoms after 2 weeks of treatment. The dosage of methylprednisolone was gradually decreased to 15 mg/day. The patient’s symptoms improved dramatically, and the eosinophil count returned to normal after treatment for 4 weeks. A follow-up capsule endoscopy examination performed 2 months later revealed that there were no mucosal lesions present in the small intestine (Figure 3).

Figure 1: Representative images of our EGE Redness, erythema, villous atrophy, erosion, ulceration, and edema.
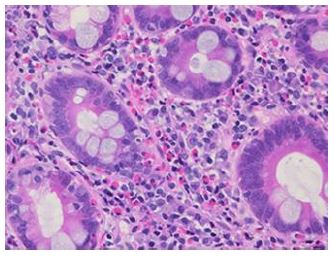
Figure 2: Histological images of the biopsy from the ileum showed eosinophilic infiltration.
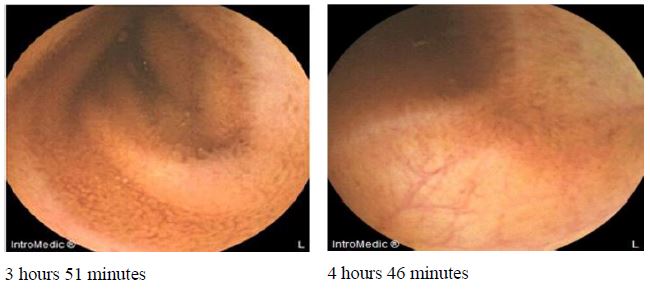
Figure 3: Capsule endoscopy post treatment showing a significant improvement of the mucosal lesions.
Discussion
EGE is an eosinophilic gastrointestinal disease characterized by infiltration of eosinophils into different layers of the gastrointestinal tract in the absence of secondary causes. A population-based study in the America from 2012-2017 reported that the overall prevalence of EGE was 5.1/100,000 persons [7]. In Japan, EGE is reported more prevalent than Eosinophilic Esophagitis (EoE) [8]. EGE occurs more frequently in Asian patients than Caucasian patients [9]. To our knowledge, no studies on the prevalence of EGE have been reported in Vietnam. The present report showed capsule endoscopy images of EGE before and after treatment for the first time in Vietnam.
EGE is an uncommon disorder that is often overlooked [10]. The clinical symptoms of EGE depend on the location and depth of the eosinophilic infiltrate. Abdominal pain, nausea, vomiting, diarrhea, weight loss, abdominal distention, and dysphagia, similar to other digestive diseases, are the most common clinical manifestations [10]. Our patient had atypical symptoms, including abdominal pain, nausea, vomiting, diarrhea, and normal endoscopic findings, which might have resulted in a clinical misdiagnosis. In this case, we found that the level of peripheral eosinophils increased, which is an important factor in the diagnosis of EGE [10]. However, high peripheral eosinophil levels have been reported in approximately 70-90% of EGE patients [10,11]. Mizumoto et al. (2021) reported three cases of EGE without high peripheral eosinophil levels [12]. Therefore, a high level of peripheral eosinophils might be a suggestion for the diagnosis of EGE, but it is not required.
Owing to its ability to view the whole small bowel, capsule endoscopy is helpful in the diagnosis of EGE. In the present study, we used MicroCam capsule MC2000, which is a double tip capsule with a constant frame rate of 3 FPS on each side. More coverage and crystal clear images of the small bowel are offered by MC2000, improving diagnostic performance. According to Yu et al. (2022), redness or erythema is the most common endoscopic finding of EGE, followed by villous atrophy, erosion, ulceration, and edema [2]. The small bowel lesions of the present patient, whose multiple erythema mucosal lesions, villous atrophy, erosion, ulceration, and edema throughout the small bowel, were more severe than some recently reported cases [3,5,12]. These findings suggested a treatment plan for the patient. The diagnosis of EGE is based on symptoms and eosinophilic infiltration of tissues; however, capsule endoscopy might be useful for determining the presence and extent of small intestinal lesions of EGE and monitoring the outcome of the lesions.
Corticosteroids are the main treatment method for patients with EGE [6,10]. Oral steroids (prednisolone 0.5 to 1.0 mg/kg/day) are the conventional treatment for EGE; the dosage is gradually reduced every one to two weeks, depending on the inflammatory bowel disease treatment plan [6]. The starting dosage for prednisone is 15-40 mg/day or 40 mg/day infusion methylprednisolone in more severe situations [10]. Our patient was treated with 40 mg/day of methylprednisolone infusion. After 2 weeks of treatment, the patient experienced a significant reduction in symptoms. The dosage was gradually decreased to 15 mg/day. The patient had a favorable response with corticoid; no mucosal lesions in his small intestine were confirmed by capsule endoscopy after 2 months.
Conclusion
We described the capsule endoscopy findings of a severe patient with EGE before and after treatment for the first time in Vietnam. The most common capsule endoscopic findings in this case were multiple areas of erythema, villous atrophy, erosion, ulceration, and edema throughout the small bowel.
Declarations
Acknowledgments: The authors acknowledge the support of the Vietnam Ministry of Science and Technology under Grant No. ĐTĐL.CN.49/19.
Author Contributions: P.P.Q.: writing – original draft preparation, conceptualization, data curation; T.N.D.: writing – review & editing, conceptualization, supervision; N.D.X.: writing and editing, investigation; T.N.H: investigation; Y.T.H.: investigation; H.V.T.: writing – review & editing. All the authors have read and agreed to the published version of the manuscript.
Ethics approval and consent to participate: This study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of Military Hospital 103 and Vietnam Military Medical University (38/2023/CNChT- HĐĐĐĐ). Informed consent was obtained for this case report.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report.
Funding: This research was funded by the Vietnam Ministry of Science and Technology, No. ĐTĐL.CN.49/19.
Declaration of conflicting interests: The authors declare that they have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Kinoshita Y, Oouchi S, Fujisawa T. Eosinophilic gastrointestinal diseases-Pathogenesis, diagnosis, and treatment. Allergology International. 2019; 68: 420-429. doi: https://doi.org/10.1016/j.alit.2019.03.003.
- Sasaki Y, Abe Y, Mizumoto N, Nomura E, Ueno Y. Small Bowel Endoscopic Features of Eosinophilic Gastroenteritis. Diagnostics (Basel, Switzerland). 2022; 13: doi: 10.3390/diagnostics13010113.
- Munjal A, Al-Sabban A, Bull-Henry K. Eosinophilic Enteritis: A Delayed Diagnosis. Journal of investigative medicine high impact case reports. 2017; 5: 2324709617734246. doi:10.1177/2324709617734246.
- Herrera Quiñones G, Scharrer SI, Jiménez Rodríguez AR, García Compean D, Borjas Almaguer OD, et al. Diagnosis of Eosinophilic Enteritis with Video Capsule Endoscopy and Double Balloon Enteroscopy with Favorable Response to Corticosteroids. ACG case reports journal. 2019; 6: e00127. doi:10.14309/crj.0000000000000127.
- Sousa M, Pinho R, Proença L. Capsule Endoscopy in the Diagnosis of Eosinophilic Enteritis. GE Portuguese journal of gastroenterology. 2019; 26: 381-382. doi:10.1159/000494095.
- Ashitani K, Tsuzuki Y, Yamaoka M, Ohgo H, Ichimura T, et al. Endoscopic Features and Diagnostic Procedures of Eosinophilic Gastroenteritis. Internal medicine (Tokyo, Japan). 2019; 58: 2167-2171. doi:10.2169/internalmedicine.2298-18.
- Mansoor E, Saleh MA, Cooper GS. Prevalence of Eosinophilic Gastroenteritis and Colitis in a Population-Based Study, From 2012 to 2017. Clinical gastroenterology and hepatology: The official clinical practice journal of the American Gastroenterological Association. 2017; 15: 1733-1741. doi: 10.1016/j.cgh.2017.05.050.
- Kinoshita Y, Furuta K, Ishimaura N, Ishihara S, Sato S, et al. Clinical characteristics of Japanese patients with eosinophilic esophagitis and eosinophilic gastroenteritis. Journal of gastroenterology. 2013; 48: 333-339. doi:10.1007/s00535-012-0640-x.
- Ito J, Fujiwara T, Kojima R, Nomura I. Racial differences in eosinophilic gastrointestinal disorders among Caucasian and Asian. Allergology International. 2015; 64: 253-259.
- Abassa KK, Lin XY, Xuan JY, Zhou HX, Guo YW. Diagnosis of eosinophilic gastroenteritis is easily missed. World journal of gastroenterology. 2017; 23: 3556-3564. doi:10.3748/wjg. v23.i19.3556.
- Hurrell JM, Genta RM, Melton SD. Histopathologic diagnosis of eosinophilic conditions in the gastrointestinal tract. Advances in anatomic pathology. 2011; 18: 335-348.
- Mizumoto N, Sasaki Y, Abe Y, Yagi M, Kon T, et al. Small-bowel Capsule Endoscopic Features in Patients with Eosinophilic Gastroenteritis: Three Case Reports. Internal medicine (Tokyo, Japan). 2021; 60: 2961-2965. doi:10.2169/internalmedicine.6935-20.
