
Open Access, Volume 10
Giant renal angiomyolipoma: Challenge treatment
Elia Expósito Ibáñez1,*; Mario Domínguez Esteban1,3; Félix Campos Juanatey1,3,4; Adriana Katherine Calapaqui Terán2; Jaime García Herrero1; Marina Sánchez Gil1; Gonzalo Azcárraga Aranegui1; Miguel Ángel Latatu Córdoba1; Félix Arnáiz Jiménez1; Jorge Crespo Bañón1; Beltrán Fernández López1; José Luis Gutiérrez Baños1,3,4
1Urology Department, Marqués de Valdecilla University Hospital, Santander, Spain.
2Pathological Anatomy Department, Marqués de Valdecilla University Hospital, Santander, Spain.
3Urology Department, Marqués de Valdecilla Research Instiute (IDIVAL), Santander, Spain.
4Faculty of Medicine, University of Cantabria, Santander, Spain.
Elia Expósito Ibáñez
Urology Department, Marqués de Valdecilla University Hospital, Santander, Spain. Email: eliaex97@gmail.com
Received : November 03, 2024,
Accepted : December 04, 2024
Published : December 16, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Giant renal Angiomyolipomas (AML) are benign renal tumors larger than 10 cm. Most are sporadic and asymptomatic. The lack of prospective trials and a limited number of large retrospective case series in this field has made it difficult for urologists to choose the best approach for their patients. Our aim is to demonstrate the different treatment options available through several cases treated at our centre.
Keywords: Giant renal angiomyolipoma; Asymptomatic; Active treatment; Case Series.
Abbreviations: AML: Angiomyolipoma; CT: Computed Tomography.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Expósito Ibáñez E (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Expósito Ibáñez E, Domínguez Esteban M, Campos Juanatey F, Calapaqui Terán AK, García Herrero J, Sánchez Gil M, Azcárraga Aranegui G, et al. Giant renal angiomyolipoma: Challenge treatment. Open J Clin Med Case Rep. 2024; 2306.
Introduction
Renal Angiomyolipoma (AML) is a benign renal entity consisting of dysmorphic blood vessels, smooth muscle and fatty tissue [1]. AML is the most frequently diagnosed benign renal tumor in clinical practice. The overall prevalence is 0.44%. Sporadic angiomyolipomas typically manifest between the ages of 50 and 60, with a higher prevalence in women. Such lesions frequently manifest as a unilateral mass and exhibit a slow growth rate. In 20% of cases, there is an association with tuberous sclerosis complex. AMLs in tuberous sclerosis appear at a younger age, grow rapidly and are often bilateral and multilocular. Tuberous sclerosis typically results from mutation in either TSC1 (which encodes hamartin) or TSC2 (which encodes tuberin). These proteins are involved in the mammalian Target Of Rapamycin (mTOR) pathway. In addition to AMLs, theses genetic alterations lead to different manifestations such as epilepsy, neurocognitive impairment, autism, astrocytomas, cardiac rhabdomyomas, retinal hamartomas, hypomelanotic macules and facial/ungual angiofibromas [2]. AMLs are often diagnosed incidentally.
Although often asymptomatic, up to 15% of patients may present with Wunderlich syndrome. AML represents the most common underlying cause of this syndrome. The term ‘giant renal AMLs’ is used to describe those than exceed 10 cm in size, although they are relatively uncommon [3]. The lack of clinical trials makes it difficult to choose the best approach for these patients. The size of these tumors requires active management due to the high risk of bleeding. Given their benign nature, kidney-sparing treatments are preferred [4]. We reported three cases of giant renal AML successfully treated in our centre.
Case Presentation
Between January 2023 and May 2024, 3 patients, aged 50 (patient A), 75 (patient B), and 76 (patient C), were diagnosed with giant renal AML. No relevant previous diseases or associated genetic syndromes were identified. On our initial evaluation, detailed medical history revealed non-specific symptoms, including abdominal pain, urinary incontinence, general syndrome. In the cases where the size was larger, physical examination revealed a palpable abdominal mass. Laboratory tests showed no remarkable findings. An abdominal ultrasound scan revealed these lesions as an incidental finding. A contrast-enhanced Computed Tomography (CT) scan was subsequently performed, which demonstrated a mass compatible with AML, with sizes ranging from 13 to 24 cm. Given the high prevalence of these tumors in tuberous sclerosis, all patients were referred to Oncology department. An exhaustive physical examination, a complete blood test, and an ophthalmological examination were conducted, which revealed nothing of interest. Furthermore, a transthoracic echocardiogram and a brain MRI was conducted. A genetic study was also conducted which excluded the presence of mutation in TSC1 and TSC2 genes. After diagnosis, active treatment was chosen with approaches in each case.
Patient A presented to the Emergency department with two episodes of presyncope, which were subsequently associated with intense abdominal pain. An abdominal tumor was palpated. The abdominal x-ray showed a large mass that had displaced the bowel (Figure 1). CT findings compatible with Wunderlich syndrome were additionally observed in patient A, although there was no evidence of active bleeding (Figure 2). Given the size of the lesion and the high risk of bleeding in this patient, an open partial nephrectomy was performed. A midline laparotomy revealed a large mass that was excised under arterial clamping with a total ischemia time of eight minutes (Figure 3). The weight of the surgical specimen was 2480 grams (Figure 4). The surgical procedure lasted 3 hours and we transferred and two units of red blood cells were subsequently transfused. On the 8th day, peritoneal drainage was removed, and patient was discharged.
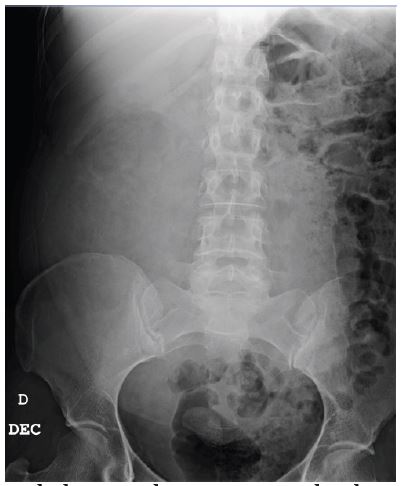
Figure 1: The abdominal x-ray reveals the displacement of the bowel loops into the left hemiabdomen.

Figure 2: CT scan of patient A shows an AML with a maximum diameter of 24,5cm.
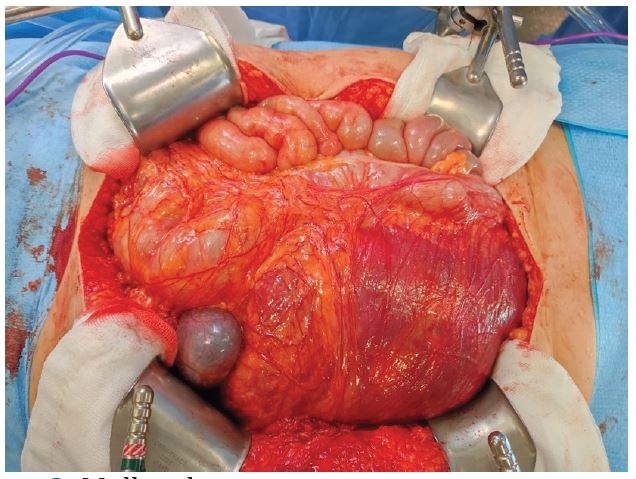
Figure 3: Midline laparotomy.
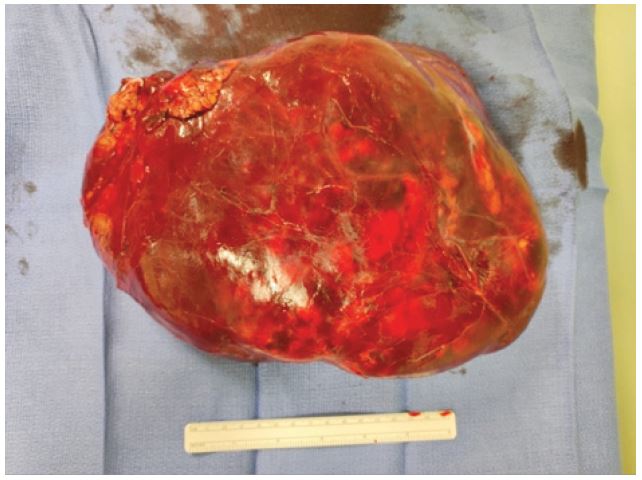
Figure 4: Surgical specimen.
In patient B, the risk of surgical resection was found to be higher due to patient’s age and comorbidities. Selective embolization of tumor branches was successfully performed in order to minimize the risk of bleeding (Figure 5). No adverse effects were observed. After four months, the lesion had decreased in size, so we performed an open partial nephrectomy due to the patient’s favorable general condition.
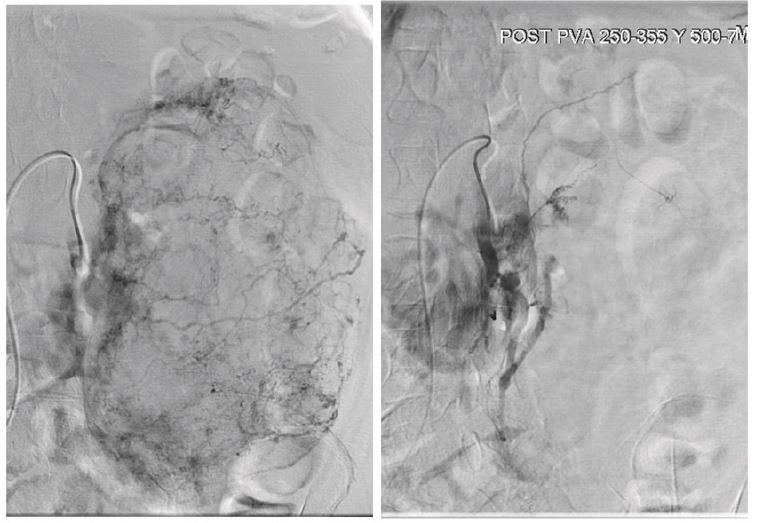
Figure 5: Before and after selective renal embolization.
The lesion on patient C was of a slightly smaller size, so we decided to underwent a robotic partial nephrectomy. The aforementioned procedure was made feasible thanks to the assistance of a three-dimensional model, which was employed during surgical procedure. This model was created beforehand on the basis of the imaging tests performed. The neovascularization present in the lesion was optimally identified and controlled (Figure 6). No complications were observed during surgical procedure and the patient was discharged on the third postoperative day.
In all cases, the immediate and late postoperative period was uneventful. The microscopic and immunohistochemical studies of the pathological anatomy in these lesions demonstrated the presence of an AML (Figure 7). Serial sections revealed a proliferation of adipose tissue, smooth muscle and blood vessels, exhibiting positive staining for actin positive and negative for cytokeratin.
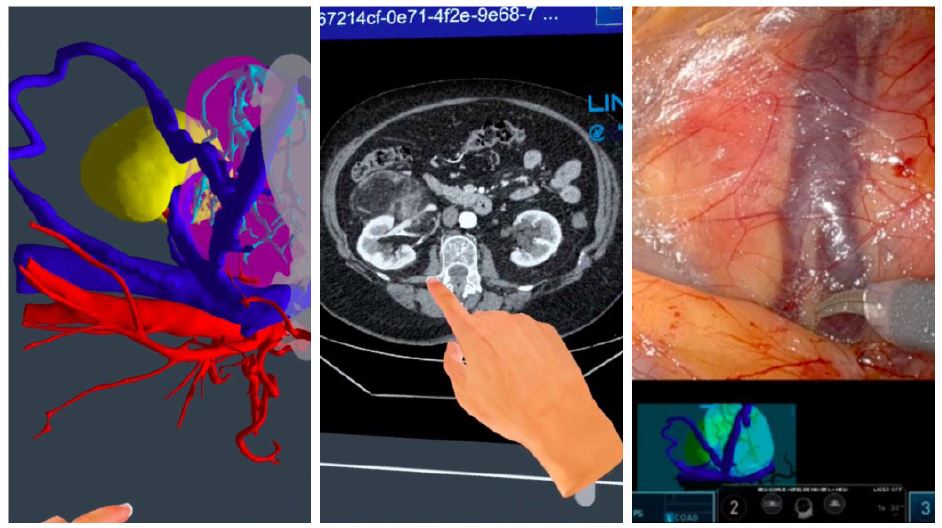
Figure 6: Correlation between preoperative 3D reconstruction and CT scan with intraoperative findings.
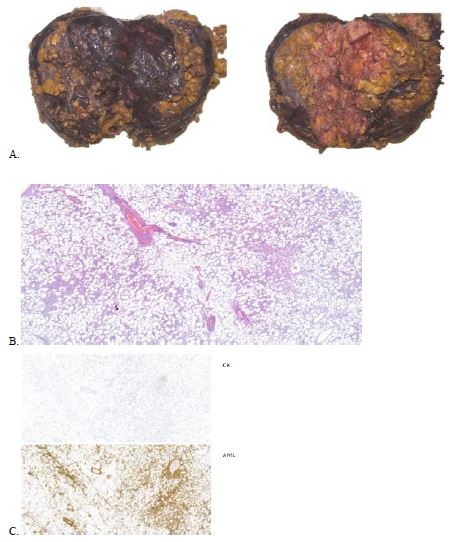
Figure 7: Main pathological anatomy findings.
(A. Macroscopic study, B. Microscopic study, C. Immunohistochemical studies -actin and cytokeratin)
(A. Macroscopic study, B. Microscopic study, C. Immunohistochemical studies -actin and cytokeratin)
Discussion
Most of renal masses are asymptomatic and are incidentally identified by non-invasive imaging techniques. Some patients present with symptoms caused by active bleeding. In most cases, ultrasound can provide a preliminary diagnosis, but a CT scan is required to confirm the diagnosis. The definitive diagnosis depends on the detection of fat within the lesion and a renal biopsy is not required for confirmation.
In large AMLs, active treatment should be considered due to the high risk of bleeding. The decision to offer active treatment may be influenced by patient characteristics such as age and comorbidities. This report presents three different approaches to achieve kidney-sparing treatment despite the large size of these lesions. We demonstrated that renal embolization represents a less invasive approach in the initial stage of treatment, with the objective of enabling surgical intervention at a later stage. Main disadvantages of less invasive selective arterial embolization are more recurrences and a need for a secondary treatment [4].
Surgery is not the first treatment for AML associated with tuberous sclerosis due to its bilateral and multifocal nature. For this reason, we carry out a genetic study in all cases. The use of drugs such as Everolimus, an inhibitor of the mTOR pathway, has been studied. A number of clinical trials have demonstrated that patients with tuberous sclerosis who have been treated with Everolimus have experienced a reduction in the volume of AML. The question remains whether Everolimus could prove an effective treatment for sporadic AML. However, the number of studies conducted is insufficient to provide a definitive answer [5].
Conclusion
AML is a common renal tumor although it rarely reaches sizes larger than 10 cm. When it does, it presents a challenge to daily urological practice. This case series, based on current scientific evidence, attempts to demonstrate effective ways of managing them. Further research is needed to assess whether they could benefit from medical treatment before or after surgery.
References
- Tsai HY, et al. Clinicopathologic analysis of renal epithelioid angiomyolipoma: Consecutively excised 23 cases. Kaohsiung J Med Sci. 2019; 35: 33.
- Alan W Parin, Roger R Dmochowski, Louis R Kavoussi, Craig A Peters, Alan Wein. Campbell Walsh Wein Urology: 12th Edition. Elselvier. 2020; 96: 2121-2132.e5.
- Ljungberg B, Bex A, et al. EAU guidelines on renal cell carcinoma. Edn presented at the EAU Annual Congress Milan. 2023; ISBN 978-94-92671-19-6.
- Fernández-Pello S, et al. Management of Sporadic Renal Angiomyolipomas: A Systematic Review of Available Evidence to Guide Recommendations from the European Association of Urology Renal Cell Carcinoma Guidelines Panel. Eur Urol Oncol. 2020; 3: 57.
- Bissler JJ, et al. Everolimus for renal angiomyolipoma in patients with tuberous sclerosis complex or sporadic lymphangioleiomyomatosis: Extension of a randomized controlled trial. Nephrol Dial Transplant. 2016; 31: 111.
