
Open Access, Volume 10
Unraveling a complex case: Brucellosis manifesting as fever of unknown origin, septic ankle arthritis, and iliacus abscess
Aya Odeh*; Farah Al Khaled
Shatha Soudi, Internal Medicine Physician, Jordan.
Aya Odeh
Shatha Soudi, Internal Medicine Physician, Jordan.
Email: aya_odeh2@hotmail.com
Received : October 22, 2024,
Accepted : November 25, 2024
Published : November 29, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Brucellosis is an infectious disease caused by bacteria of the genus Brucella, predominantly affecting livestock and humans through contact or consumption (Department of Communication World Health Organization Media Center, 2011). It is a major public health challenge, particularly in the developing countries. Symptoms can be mild to severe, making diagnosis difficult and often resulting in more chronic problems if those issues are not addressed. Our case report is about a patient with brucellosis who ended up having multiple organ involvement and focusing on the benefits of early diagnosis and management.
Case presentation: A 61-year-old Jordanian male with significant medical history, including heart failure, diabetes, and hypertension, was admitted for left ankle pain, redness, and swelling after a recent travel to Italy. His symptoms began four months prior with abdominal pain, fever, and persistent gastrointestinal issues, worsening despite oral antibiotics. He developed progressive thigh pain and was ultimately diagnosed with septic arthritis, experiencing ongoing fever and new anemia. Blood tests indicated elevated ESR, CRP, and leukocytosis, while cultures were negative. Imaging revealed fluid collections around the right iliac and gluteus minimums muscles. A diagnosis of brucellosis was confirmed through lab tests. Management included intravenous teicoplanin, hydration support, pain relief, and imaging-guided drainage to address the infection and its complications.
Discussion: Brucellosis, a zoonotic infection from *Brucella*, poses a public health threat, particularly in developing countries. Its symptoms can mimic other conditions, complicating diagnosis. Effective treatment typically involves a combination of antibiotics, with early intervention critical for favorable outcomes. The case highlights the need for awareness of brucellosis in patients with fever of unknown origin, iliacus abscess and septic arthritis and emphasizes the importance of considering travel history and comorbidities in diagnosis and management.
Conclusion: In conclusion, this case highlights the diverse manifestations of brucellosis, including atypical symptoms such as fever of unknown origin, septic arthritis, and iliacus abscess. Studies underscore the need to consider brucellosis in the differential diagnosis of FUO, especially in endemic regions. A multidisciplinary management approach and a high level of clinical suspicion are crucial for achieving optimal outcomes in patients with this complex infection.
Keywords: Brucellosis; Fever of unknown origin; Septic arthritis; Hemolytic anemia; Iliacus Abscess; Infection.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Odeh A (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Odeh A, Al Khaled F. Unraveling a complex case: Brucellosis manifesting as fever of unknown origin, septic ankle arthritis, and iliacus abscess. Open J Clin Med Case Rep. 2024; 2304.
Introduction
Brucellosis: A global public health concern
Brucellosis is a worldwide zoonotic disease caused by intracellular Brucella bacteria, primarily affecting humans who come into contact with infected animals or consume unpasteurized dairy products. This illness remains a significant public health issue, especially in developing countries where livestock farming is common.
The clinical presentation of brucellosis varies widely, ranging from mild flu-like symptoms to severe systemic complications, which complicates diagnosis. If left untreated, chronic complications may develop, resulting in long-term health issues. The disease can impact various organs, with the skeletal system being the most frequently affected, seen in 10% to 85% of patients. Spinal involvement is widespread, occurring in 54% of cases. Due to the nonspecific symptoms associated with Brucella Spondylitis (BS), misdiagnosis and improper treatment are common challenges [1].
This case report details the clinical course, diagnostic difficulties, and treatment outcomes for a patient diagnosed with brucellosis. By highlighting this case, we aim to raise awareness among healthcare professionals about the disease and emphasize the critical importance of early recognition and management to prevent severe complications.
Case Presentation
A 61-year-old Jordanian male with No Known Drug Allergies (NKDA), a history of smoking (35 pack-years), and significant past medical history, including heart failure with an Ejection Fraction (EF) of 35%, Diabetes Mellitus (DM), Hypertension (HTN), dyslipidemia, and glaucoma. His past surgical history includes a catheterization, which was without complications.
A patient was admitted to the hospital with left ankle pain, redness, heat, and swelling. He reported traveling to Italy four months ago, where his symptoms began with abdominal pain, black stools, constipation, and a documented fever of 39°C. The fever persisted until diagnosis, with no improvement observed, and was associated with rigors, chills, tremors, and fatigue.
Before the fever began, he complained of anaemia, which developed prior to the onset of the fever. Despite being prescribed oral antibiotics, he experienced no improvement. He later developed progressive right anterior thigh pain and limping, treated with Relaxon and Panadol, but without relief. He now reports right ankle pain with similar symptoms, diagnosed as septic arthritis by MRI (Figure 1) and underwent drainage with persistent fever.
Blood tests revealed an ESR of 115, CRP of 255, WBC of 12.7, and Hb of 9. Urinalysis and urine culture were unremarkable, and both blood and swab cultures were negative.
Table 1: Lab Results.
The laboratory test results reveal several significant findings. The ESR is elevated at 115 mm/hr, indicating considerable inflammation, while the CRP level is also high at 255 mg/L, suggesting an acute inflammatory response or infection. A sodium spot urine test shows a normal level of 94.20 mmol/L, reflecting adequate renal sodium handling. Notably, synovial fluid analysis revealed no crystals, ruling out crystal-induced arthropathy. The creatinine level is slightly elevated at 1.41 mg/dL, which may indicate renal impairment or dehydration. CPK is within the normal range at 0.68 ukat/L, suggesting no significant muscle damage. The FIT test is positive, indicating gastrointestinal bleeding. The Hb A1c level of 7.50% points to poor glycemic control in diabetes management, and serum sodium is low at 129 mmol/L, suggesting hyponatremia. The blood film shows mild anisocytosis and minimal polychromasia in red blood cells, which may relate to anemia or chronic disease. White blood cell morphology reveals mild neutrophilia with variable cytoplasmic granulation and nuclear segmentation, indicating an ongoing inflammatory response or infection. Lastly, mild thrombocytopenia is noted, which may require further evaluation.
| LAB TEST | RESULT | COMMENT |
|---|---|---|
| HB | 78 gm/L | |
| ESR | 115 | |
| CRP | 255 | |
| Sodium spot urin | 94.20 mmol/L | |
| Synovial fluid crystals | No crystals seen | |
| Creatinine | 1.41 mg/dl | |
| Cpk | 0.68 ukat/L | |
| FIT | Positive | |
| Hb a1c | 7.50 | |
| Sodium serum | 129 mmol /L | |
| Blood film | RBCs morphology: Mild anisocytosis, minimal polychromasia,features of high ESR on bloodsmear. WBC morphology: mild neutrophilia, neutrophils shows variable cytoplasmic granulation and neuclear segmentation. PTLS: mildthrombocytopenia. |
X-rays of the chest, pelvis, and femur showed a normal chest X-ray, bilateral osteoarthritis changes in the pelvis, and soft tissue calcification around the right hip joint, with vascular calcification also noted. A chest, abdomen, and pelvis CT with IV contrast identified a 29 x 44 x 88 mm fluid collection with internal gas locules deep to the right iliac muscle and a 22 x 38 mm fluid collection deep to the right gluteus minimums muscle (Figure 2). We decided to perform a pelvic MRI with contrast and US drainage. The patient continues to have a Fever of Unknown Origin (FUO). Subsequently, lab tests for brucellosis showed a positive titer, confirming brucellosis as the cause of his symptoms for the past four months.

Figure 1: Left Ankle Septic Arthritis MRI.
- Evidence of Thick Peripherally Enhancing Effusion Involving the Talocrural and Subtalar Joint Spaces.
- Diffuse Subcutaneous Edema Seen Overlying the Lateral Malleolus Eith Extension into the Dorsal Aspect of the Hindfoot with No Well-Formed Collection Seen.
- Evidence of Thick Peripherally Enhancing Effusion Involving the Talocrural and Subtalar Joint Spaces.
- Diffuse Subcutaneous Edema Seen Overlying the Lateral Malleolus Eith Extension into the Dorsal Aspect of the Hindfoot with No Well-Formed Collection Seen.
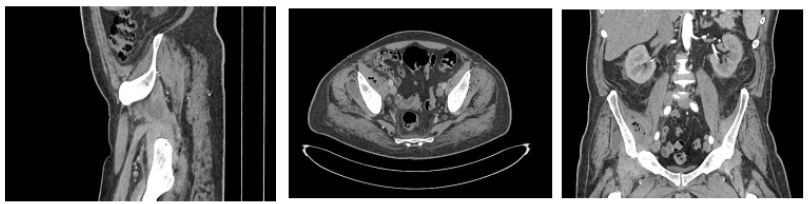
Figure 2: Abdomen and Pelvis Ct with IV Contrast.
- Identified a 29 x 44 x 88 mm fluid collection with internal gas locules deep to the right iliac muscle and a 22 x 38 mm fluid collection deep to the right gluteus minimums muscle.
- Identified a 29 x 44 x 88 mm fluid collection with internal gas locules deep to the right iliac muscle and a 22 x 38 mm fluid collection deep to the right gluteus minimums muscle.

Figure 3: Abdomen and Pelvis MRI with Contrast.
- 3*5.8*8.6 cm ring-enhancing collection seen in the right iliac muscle with multiple gas locules, associated with diffuse oedema within the muscle and minimal surrounding fat standing.
- There’s another similar ring-enhancing collection seen in the right gluteus minimums muscle measuring 4.8*3.8*3.3 cm with minimal oedema in the muscle and minimal.
- 3*5.8*8.6 cm ring-enhancing collection seen in the right iliac muscle with multiple gas locules, associated with diffuse oedema within the muscle and minimal surrounding fat standing.
- There’s another similar ring-enhancing collection seen in the right gluteus minimums muscle measuring 4.8*3.8*3.3 cm with minimal oedema in the muscle and minimal.
The management of the patient began with the initiation of teicoplanin, administering 400 mg intravenously twice for three doses, followed by a maintenance dose of 400 mg once daily. To support hydration and manage any potential renal implications, normal saline (0.9%) was infused at 60 ml/hr.
Symptomatic relief was provided with Perfalgan (1 g IV, four times daily) and pethidine (50 mg intramuscularly, three times), addressing the patient’s pain. Additionally, Prizma 4.5 IV was given four times daily, while Clexan (40 mg subcutaneously) and Lasix (20 mg were administered as part of the management strategy to prevent thromboembolic complications and manage fluid status. After identifying significant fluid collections via imaging, US was performed for drainage, followed by a pelvic MRI with contrast (Figure 3) for further investigations, which shows:
- 3*5.8*8.6 cm ring-enhancing collection seen in the right iliac muscle with multiple gas locules, associated with diffuse edema within the muscle and minimal surrounding fat standing.
- There’s another similar ring-enhancing collection seen in the right gluteus minimums muscle measuring 4.8*3.8*3.3 cm with minimal edema in the muscle and minimal surrounding fat standing.
- Diffuse oedema involving all right adductor muscle suggestion muscle strains.
- Bone marrow oedema was seen in the right iliac bone and acetabulum, likely reactive osteitis.
- Mildly distended right iliopsoas bursa with rim enhancement suggestion bursitis.
- Mild right hip joint fluid with synovial mild enhancement suggesting synovitis.
- Minimal free fluid was seen in the pelvis.
US guidance was on LA & septic technique. A 12 FR pigtail drainage catheter was inserted and fixed successfully to drain the iliacus muscle abscess (it was thick, infected, and yellowish) in addition to that, there was no immediate complication. Moreover, to rule out cancer due to having IDA (Iron Deficiency Anaemia), we performed upper and lower endoscopies, and it was clear except for haemorrhoids.
Upon confirming the diagnosis of brucellosis, specific treatment protocols were initiated, marking a crucial step in addressing the patient’s underlying infection and associated complications. The patient was on doxycycline 100 mg, 1*2, and rifampicin 600 mg, 1*1.
Discussion
Case report: A complex presentation of brucellosis
This case report focuses on a 61-year-old Jordanian male with multiple comorbidities, including heart failure (ejection fraction 35%), diabetes, hypertension, and a history of smoking. He presented with fever, abdominal pain, and joint symptoms following a trip to Italy. Initial symptoms began four months earlier, characterized by abdominal pain, melena, and persistent fever reaching up to 39°C, which did not improve with outpatient antibiotic treatment.
The patient subsequently developed left ankle pain accompanied by redness and swelling, along with progressive pain in the right thigh, leading to a diagnosis of septic arthritis.
Laboratory tests revealed elevated inflammatory markers (ESR 115 mm/h, CRP 255 mg/L), leukocytosis (WBC 12.7 × 109/L), and anemia (Hb 9 g/dL). Urinalysis was unremarkable, and cultures returned negative, complicating the diagnostic process.
Imaging studies, including X-rays of the chest, pelvis, and femur, indicated bilateral osteoarthritis and soft tissue calcifications. A CT scan identified significant fluid collections deep to the right iliac and gluteus minimus muscles. Despite the ongoing fever, serological tests for brucellosis eventually returned positive.
Management included initiating teicoplanin for potential co-infection, administering analgesics for pain relief, and providing intravenous fluids. Ultrasound-guided drainage of the fluid collections was performed, which proved crucial for symptom relief and microbiological assessment. Upon confirmation of brucellosis, teicoplanin was discontinued, and the patient was started on doxycycline (100 mg, twice daily) and rifampicin (600 mg, once daily).
This case underscores the importance of considering travel history in diagnosing infectious diseases and highlights the complexities involved in managing patients with multiple comorbidities, necessitating a multidisciplinary approach for optimal outcomes.
Moreover, this case illustrates a rare and complex manifestation of brucellosis, presenting as a Fever of Unknown Origin (FUO) alongside complications such as septic ankle arthritis, anemia and an iliacus abscess. These manifestations highlight the diagnostic challenges and the necessity of maintaining a high index of suspicion among clinicians, particularly in endemic regions.
Brucellosis Overview
Brucellosis is a zoonotic infection primarily caused by the Brucella genus, transmitted from animals to humans, typically through unpasteurized dairy products or direct contact with infected animals.
The global incidence of brucellosis varies significantly, with higher prevalence observed in regions such as the Mediterranean, the Middle East, and parts of South Asia and Africa. In contrast, human brucellosis is rare in the United States, with only a few hundred cases reported annually, primarily among high-risk occupational groups, such as veterinarians and farmworkers [2].
Brucella species invade the reticuloendothelial system, effectively evading the host’s immune response. Once in the bloodstream, these bacteria can disseminate to various organs, resulting in a wide range of clinical manifestations. Their ability to survive intracellularly contributes to both their pathogenicity and the chronic nature of the infection. Importantly, the presence of antibodies against Brucella does not always correlate with disease severity, complicating both diagnosis and treatment [3].
Brucellosis is characterized by a variety of symptoms, including fever, chills, malaise, and sweats, often leading to presentations of Fever of Unknown Origin (FUO). In our case, the patient exhibited FUO, septic ankle arthritis, and an iliacus abscess. These symptoms reflect the disease’s nature and its potential to mimic other conditions, emphasizing the need for heightened clinical awareness.
Additionally, hemolytic anemia may occur due to immune-mediated mechanisms or direct invasion of red blood cells [4]. Septic arthritis and abscess formation arise from hematogenous spread, underscoring the critical importance of early intervention in managing brucellosis.
Diagnostic Challenges
Diagnosing brucellosis is often challenging due to its nonspecific symptoms and variable presentations. Serological testing remains the cornerstone of diagnosis, with standard agglutination tests and Enzyme-Linked Immunosorbent Assays (ELISA) commonly employed. While culturing Brucella from blood or tissue samples is the definitive method, it can be time-consuming and may yield negative results, especially following prior antibiotic therapy. Imaging studies, such as ultrasound or MRI, may be necessary to identify abscesses or joint involvement.
The treatment of brucellosis typically involves a combination of antibiotics to enhance efficacy. The World Health Organization (WHO) recommends a regimen of doxycycline and rifampin for at least six weeks, with the addition of streptomycin or gentamicin for severe cases [6]. In this case, the early initiation of appropriate antibiotics was crucial in preventing complications. Surgical intervention may be required for abscess drainage or joint debridement in cases of septic arthritis.
Prognosis and Prevention
The prognosis for brucellosis varies depending on the severity of the infection and the timeliness of treatment. Most patients respond well to appropriate antibiotic therapy; however, relapses can occur, particularly in severe or chronic cases [7]. Long-term complications may include spondylitis, chronic arthritis, or reproductive health issues. Our patient’s prognosis improved significantly with prompt diagnosis and treatment, highlighting the critical importance of early recognition and intervention.
Preventive Measures
Preventive measures are essential for controlling the spread of brucellosis. Public health strategies should focus on livestock vaccination, pasteurization of dairy products, and educating high-risk populations about safe handling practices for animals and animal products. Implementing robust surveillance systems can help monitor and control outbreaks, particularly in endemic areas [8]. Moreover, enhanced awareness among healthcare providers regarding the diverse presentations of brucellosis is vital for early diagnosis and the prevention of complications.
Brucellosis and Fever of Unknown Origin
The initial presentation of Fever of Unknown Origin (FUO) poses a common challenge in clinical practice. Studies indicate that brucellosis can significantly contribute to FUO, with various reports demonstrating the prevalence of Brucella antibodies in affected patients. For instance, a study in Ethiopia found that 3.6% of patients with FUO tested positive for brucellosis, emphasizing the importance of including it in the differential diagnoses for FUO cases [9]. Similarly, research from China revealed that 54% of patients with confirmed brucellosis presented with FUO, particularly among individuals exposed to livestock [10].
These findings underscore the need to consider brucellosis when evaluating patients with unexplained fevers, especially in regions with known zoonotic transmission. In children, brucellosis has also emerged as a leading cause of FUO. A Turkish study demonstrated that 15.2% of children with FUO were diagnosed with brucellosis, advocating for increased awareness and prompt serological testing in pediatric populations presenting with FUO [11].
Septic Arthritis
The development of septic ankle arthritis in our case aligns with existing literature, which highlights brucellosis’s potential to cause significant joint involvement, including septic arthritis and osteoarthritis [12]. Early recognition and treatment are crucial to preventing joint damage and chronic complications. A report on septic arthritis caused by Brucella melitensis underscores the importance of maintaining a high suspicion for brucellosis in patients presenting with joint symptoms, particularly those with relevant exposure histories [13].
Timely identification of this condition can significantly improve patient outcomes, as demonstrated by successful interventions documented in similar cases.
Iliacus Abscess
The iliacus abscess observed in our patient represents a rare but serious complication of brucellosis. Abscess formation can occur due to hematogenous spread or direct extension from adjacent infected tissues. The importance of imaging studies in diagnosing such complications cannot be overstated, as they enable early surgical intervention when necessary. This case contributes to the growing body of literature on the diverse complications of brucellosis and reinforces the need for thorough evaluation in cases of Fever of Unknown Origin (FUO).
One of the rarest types of abscesses is this one, where the abscesses form near the iliac muscle. Muscle abscesses due to brucellosis usually appear in the psoas and paravertebral muscles. The physical examination findings were normal, except for hip joint pain and limited range of motion. Only one case of a psoas abscess linked to brucellosis in the literature did not require surgical drainage and was effectively treated with anti-Brucella drugs. Psoas abscesses require surgical drainage and antibiotic therapy. In the only previous case in the literature, the abscess could not be drained because of its location, and it was not possible to obtain a specimen for culture.
However, it was effectively treated with antimicrobials that are effective for brucellosis. MRI is an effective method for identifying spondylodiscitis, particularly in the initial phases, as well as paraspinal or epidural abscesses, and nerve or root compression related to brucellosis. The diagnosis of both the iliacus muscle abscess and olecranon bursitis was made using MRI [14].
The bacteria can damage intervertebral discs and vertebral bodies, leading to cervical instability.
Inflammatory granulation tissue and abscesses may compress the spinal cord, resulting in sensory and motor dysfunction in the limbs and potentially causing paraplegia. Pain is the most prevalent symptom among patients with brucellosis. While brucellosis- related spondylitis is uncommon, cervical spondylitis is particularly rare. This serious complication can lead to chronic pain, neurological issues, and paralysis if not accurately diagnosed and treated. Furthermore, the overuse of Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) and antibiotics in China has made the typical fever pattern observed in brucellosis spondylitis patients less common, further complicating the diagnostic process [15].
Epidural abscesses most frequently occur in the lumbar vertebrae, while cervical spine involvement is relatively uncommon. The management of spinal epidural abscesses remains a topic of ongoing debate within the medical community. In certain cases, particularly among patients with stable neurological status, effective treatment has been achieved using antibiotics alone. However, when signs of spinal cord compression are present, the situation becomes a neurosurgical emergency due to the risk of rapid and progressive paralysis. This underscores the critical need for timely diagnosis and intervention to prevent severe neurological outcomes in patients affected by brucellosis-related complications.
Brucellosis can progress to systemic involvement, with the musculoskeletal system being especially susceptible to complications such as arthritis, bursitis, sacroiliitis, spondylitis, and osteomyelitis. Notably, a spinal epidural abscess is a rare but serious complication that may arise during spondylitis caused by Brucella species. While spine brucellosis is uncommon, it can be a debilitating manifestation of the disease [16].
On the other hand, the presence of abscesses was revealed following the diagnosis of brucellosis in various internal organs, including the spleen, renal tubules, para-aortic area, and even in testicular and tubo-ovarian regions. Brucellosis is associated with a range of genitourinary infections in males, such as Brucella Epididymal-Orchitis (BEO), cystitis, prostatitis, interstitial nephritis, pyelonephritis, exudative glomerulonephritis, and the formation of renal and testicular abscesses, as well as seminal vesiculitis.
BEO, while an infrequent complication of brucellosis, occurs in approximately 5.7% of cases and is commonly unilateral. The prevailing symptoms of BEO include fever, scrotal pain and swelling, chills or rigors, malaise, generalized discomfort, fatigue, and headache. The incidence and nature of complications can vary based on the specific strain of the infecting Brucella, the patient’s age, and the duration of the illness [16].
Conclusion
This case study emphasizes the challenges of diagnosing and treating brucellosis, especially in patients with multiple underlying health conditions. A 61-year-old man from Jordan exhibited unusual symptoms, such as septic arthritis in the ankle and an abscess in the iliacus, which complicated the diagnosis and postponed the start of proper treatment.
Extensive investigations, such as imaging and serological tests, were necessary to confirm the diagnosis of brucellosis, highlighting the potential for the disease to manifest as a fever of unknown origin. This case demonstrates the importance of increased clinical awareness, especially in endemic areas or among individuals with recent travel history, in order to promote early detection and intervention.
The effective treatment of the patient, involving the use of antibiotics and the surgical removal of abscesses, led to notable progress, highlighting the crucial need for timely intervention to avoid serious complications. Additionally, this instance adds to the increasing pool of research on brucellosis, underscoring the vital importance of comprehensive assessment for patients with unexplained symptoms and the essential consideration of brucellosis in the range of potential diagnoses.
In general, this instance acts as a prompt regarding the persistent public health issue presented by brucellosis and the necessity for ongoing training among healthcare professionals to identify and manage this zoonotic illness efficiently.
Declarations
Conflict of interest: The authors declare that they have no conflicts of interest. They take full responsibility for the content and writing of this paper. No editorial assistance or support was provided in the preparation of the article. Additionally, no funding or support from any organization or company was received during the study.
Consent: Written informed consent was obtained for the publication of this case and accompanying images.
References
- Gou L, Yang Y, Li J, et al. MRI findings and classification of brucella spondylitis: A China multicenter study. Eur J Med Res. 2024; 29: 469.
- Pappas G, Papadimitriou P, Akritidis N, Christou L, Tsianos EV. The role of Brucella spp. in human disease. Clinical Microbiology Reviews. 2006; 19(3): 429-438.
- Garin-Bastuji B, et al. Brucellosis: A review of the current state of the disease. Infectious Disease Clinics of North America. 2017; 31(3): 531-552.
- Montenegro A, et al. Hemolytic anemia associated with brucellosis. The Journal of Infection in Developing Countries. 2021; 15(4): 564-568.
- Burgdorfer W, et al. Diagnosis and treatment of brucellosis. The American Journal of Medicine. 1996; 101(3): 304-313.
- Bouguila J, et al. Antimicrobial therapy for brucellosis: A review. Expert Review of Anti-infective Therapy. 2018; 16(2): 115-124.
- López-Gatell H, et al. Long-term sequelae of brucellosis: A follow-up study. Tropical Medicine and International Health. 2019; 24(9): 1054-1061. DOI: 10.1111/tmi.13236
- OIE. Brucellosis. World Organisation for Animal Health. Retrieved from OIE website. 2019.
- Tolosa TG, Tadele Regassa, Fekadu Belihu, Kelay. Brucellosis among patients with fever of unknown origin in Jimma University Hospital, southwestern Ethiopia. Ethiopian journal of health sciences. 2007; 17.
- Wu ZG, Song ZY, Wang WX, et al. Human brucellosis and fever of unknown origin. BMC Infect Dis 22, 868 (2022). https://doi.org/10.1186/s12879-022-07872-8. DOI: https://doi.org/10.1186/s12879-022-07872-8.
- Çiftdoğan DY, Bayram N, Vardar F. Brucellosis as a Cause of Fever of Unknown Origin in Children Admitted to a Tertiary Hospital in the Aegean Region of Turkey. Vector-Borne Zoonotic Dis. 2011; 11(8): 1037-40.
- Hassan MA, Noor F, Salehi A, Al Hariri B. Brucellosis an Unusual presentation as isolated septic mono-arthritis of the knee joint: A case report. Heliyon. 2024; 10(4).
- Chernchujit B, Srimongkolpitak S, Kintarak J, Pornmeechai Y. The role of shoulder arthroplasty after chronic brucellosis of glenohumeral joint septic arthritis. A case report and literature reviews. Int J Surg Case Rep. 2022; 97: 107467.
- Wang J, Zhang Q. Early diagnosis and treatment of acute brucellosis knee arthritis complicated by acute osteomyelitis: Two cases report. BMC Infect Dis. 2022; 22: 430.
- Bapir R, Abdalqadir AM, Aghaways E, Bayz HH, Abdullah HO, et al. Brucella epididymo- orchitis: A single-center experience with a review of the literature. Arch Ital Urol Androl. 2023; 95(4): 11978.
Full article: Cervical Brucella Spondylitis: A Case Report on Diagnosis and Surgical Management (tandfonline.com) - Abu Nowar H, Al Dalahmeh A, Alrabadi M, et al. Exploring the Complex Landscape of Spine Brucellosis. Cureus. 2024; 16(1): e51761.
