
Open Access, Volume 10
Fatal masquerade: A case of calciphylaxis concealed as cellulitis
Rocio Rimachi1*;Anke Van Mellaert2; Fabrice Kanyanzira3; Hussein Rahal2; Charlotte Van Noten2
1Department of Intensive Care, Delta Chirec Hospital, Brussels, Belgium.
2Department of Internal Medicine, Division of Nephrology, Delta Chirec Hospital, Belgium.
3Department of Emergency, Delta Chirec Hospital, Brussels, Belgium.
Rocio Rimachi
Department of Intensive Care, Delta Chirec Hospital, Brussels, Belgium.
Email: rocio.rimachi@gmail.com
Received : October 28, 2024,
Accepted : November 20, 2024
Published : November 29, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Calciphylaxis is a rare but potentially life-threatening condition. The clinical diversity of presentation contributes to diagnosis delays. We report a case of a woman with end-stage chronic kidney disease under dialysis, who complained of lower abdominal pain and exhibited subcutaneous infiltration with erythematous painful skin lesions in the hypogastric region, erysipelas was suspected, and antibiotic treatment initiated. Urgent extensive surgical debridement of necrotic tissue was performed. Histopathological examination revealed calcifications in the wall of small vessels. The patient’s condition progressed within 24 hours to refractory shock ultimately leading to death from circulatory shock.
Keywords:Calciphylaxis; Chronic kidney disease; Thiosulfate; Warfarin.
Abbreviations: CUA: Calcific Uremic Arteriolopathy; CKD: Chronic Kidney Disease.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Rimachi R (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Rimachi R, Van Mellaert A, Kanyanzira F, Rahal H, Van Noten C. Fatal masquerade: A case of calciphylaxis concealed as cellulitis. Open J Clin Med Case Rep. 2024; 2303.
Introduction
Calciphylaxis or Calcific Uremic Arteriolopathy (CUA) is a rare but potentially fatal condition characterized by calcification in subcutaneous arteries, thrombosis, and tissue ischemia. Late recognition due to the diversity in clinical presentation, is associated with an increased risk of life-threatening complications. Patients with CUA have a poor outcome, with a long-term mortality rate exceeding 50% [1]. It is most often observed in patients with advanced Chronic Kidney Disease (CKD), frequently affecting the lower extremities. The clinical diversity of presentation contributes to diagnostic delays, with skin biopsy currently regarded as the gold standard for confirmation.
Reported herein is an atypical manifestation of progressive and severe calciphylaxis in a patient with CKD undergoing dialysis, ultimately leading to death from circulatory shock.
Case Description
A 70A 73-year-old woman presented lower abdominal pain 2 weeks before hospital admission. Upon examination, she exhibited subcutaneous infiltration with erythematous painful skin lesions limited to the hypogastric region. Abdominal Computed Tomography (CT) revealed hepatic steato-cirrhosis, along with edematous infiltration of subcutaneous fat. Laboratory investigation showed elevated plasma levels of C reactive protein 50 mg/L, white blood cell counts 8.800/mm3, proteins 61.7 g/L, serum calcium 2.27 mmol/L, serum phosphate 2.35 mmol/L and parathormone 2.048,9 ng/L (normal: 18,5-88,0 ng/L). She had a history of renal cell carcinoma with pulmonary and bone metastasis, treated by nephrectomy six years previously and immunotherapy, and was in complete remission.
Additionally, she had been undergoing dialysis for chronic renal failure for five years, had diabetes, and was obese. She also had severe secondary hyperparathyroidism, which was being treated with etelcalcetide. Furthermore, she was on anticoagulation therapy with fenprocoumon, initiated two months prior to admission, due to refractory dysfunction of the hemodialysis catheter and paroxysmal atrial fibrillation.
A diagnosis of erysipelas was initially suspected, and treatment with amoxicillin-clavulanate was started. Five days later vancomycin was added because of lack of improvement. During the following five days abdominal pain increased, and she presented to the emergency department with hypotension, rapid atrial fibrillation, and elevated lactate levels 6 mmol/L (normal: 0,5-1,5 mmol/L). Upon physical examination, an erythematous, painful subcutaneous infiltration with extensive purpuric lesions was observed in the hypogastric region (Figure 1).
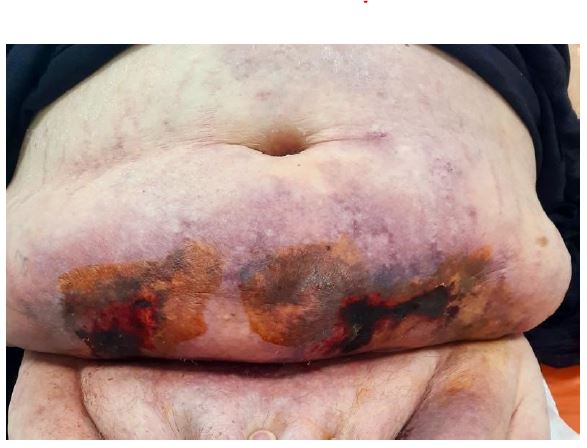
Figure 1: Ulcer with black eschar, irregular violaceous boundaries, surrounding erythema and retiform purpura.
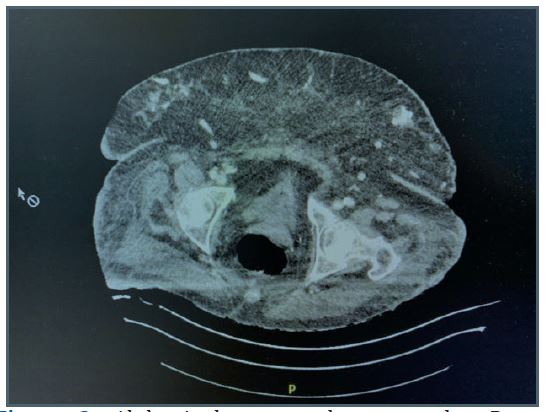
Figure 2: Abdominal computed tomography: Deep collection in subcutaneous fat corresponding to area of necrosis.
The patient’s medication regimen included Simvastatin®, L-thyroxin®, Pantomed®, etercalcetide, calcitriol and enoxaparin. A subsequent abdominal CT revealed a deep collection within the subcutaneous fat in contact with the muscular wall with high density, corresponding to an area of necrosis (Figure 2).
Laboratory tests revealed elevated CRP 290 mg/L, white blood cell count 14,600/mm3, calcium 2.82 mmol/L, urea 54 mg/dL, creatinine 3.37 mg/dL, albumin 29,1 g/L and alkaline phosphatase 146 U/L (normal: 35-104 U/L). Urgent extensive surgical debridement of necrotic tissue was performed, and the antibiotic regimen was modified to piperacillin-tazobactam, clindamycin and vancomycin.
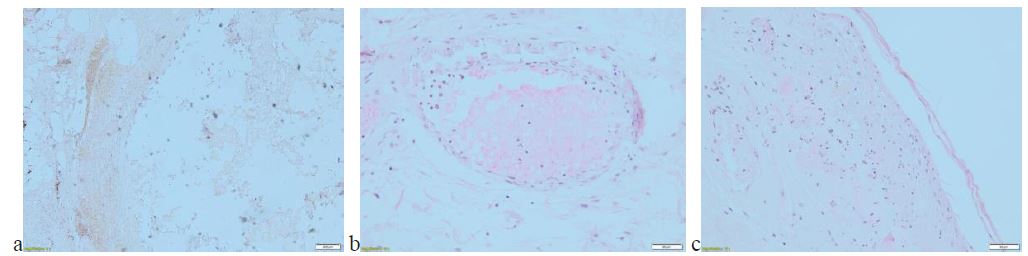
Figure 3: Histological features: (a) Calcification within adipose tissue and necrosis, (b) Circumferential calcification, (c) Necrosis of the epidermis and microcalcification.
Histopathological examination revealed interstitial calcification, vascular ectasia in the middle dermis and calcifications in the wall of small vessels, without evidence for gangrenous pyoderma. Von Kossa staining provided further evidence in favor of CUA (Figure 3).
The patient’s condition progressed within 24 hours to refractory circulatory shock and multiorgan failure. Following discussion with the family regarding goals of care and prognosis, they opted for palliative and comfort measures without further medical treatment. Sodium thiosulfate was not prescribed.
Discussion
Calciphylaxis or CUA is a rare and aggressive vascular occlusive disease. Calcification within small caliber vessels leads to progressive narrowing of their lumens and subsequent tissue ischemia due to thrombosis.
Seyle [2], first described CUA in rodents by inducing subcutaneous calcification through “sensitization” with parathyroid extracts, hypervitaminosis and high phosphorus diet followed by application of a “challenging” agent such as local trauma, egg albumin or metallic salts. Moe et al. demonstrated that in response to hyperphosphatemia, hypercalcemia and hyperglycemia, vascular smooth muscle cells transform into osteoblast-like cells able to produce and deposit hydroxyapatite crystals [3]. However, calciphylaxis has been described with normal or minimally elevated calcium and phosphate levels.
Other factors contributing to the development of CUA include deficiencies in vascular calcification inhibitors such as fetuin-A, osteoprotegerin, and Matrix G1a Protein (MGP) [4]. Fetuin-A is a glycoprotein that binds calcium and phosphorus, potentially preventing calcification of vessels and soft tissues. MGP inhibits calcification but requires vitamin K activity [5]. In addition, aberrant adipocytes, proinflammatory cytokines and recurrent vascular endothelial injury may also play role [6]. Physical trauma may lead to endothelial damage and subsequent activation of the coagulation cascade resulting in thrombosis, a phenomenon known as Koebner phenomenon. The largest study from Fresenius Medical Care North America (FMCNA) reports an incidence rate of CUA was 3.4/1,000 patients among patients receiving maintenance hemodialysis [7]. CUA in patients with normal renal function, known as nonuremic or non-nephrogenic CUA carries a lower incidence [8].
Additional risk factors for CUA include diabetes, obesity, female sex, protein C or S deficiency, iron infusions, corticosteroid use, immunosuppressive drugs, and warfarin use, as well as hypoalbuminemia and autoimmune processes.
Typically, lesions associated with CUA are extremely painful, and livedo reticularis may also develop due to ischemia. Subsequently, the lesions progress to ulceration with the development of necrosis and eschar. CUA ulcerations can be mistaken for pyoderma gangrenosum or warfarin and heparin-induced necrosis, antiphospholipid syndrome or infected diabetic ulcers [4]. Additionally, plaques may be mistaken for cellulitis, as they both present with redness, warmth, and tenderness. The rapid progression to ulcers with black eschar is the hallmark of CUA presentation.
Patients present mostly with lesions on the lower extremities and upper extremity involvement is less common. Distal lesions generally have a better prognosis compared to proximal lesions, which may appear on the thighs, buttocks, and abdomen [1]. CUA is a clinical diagnosis, but definitive diagnosis relies on biopsy findings. However, the association between the Koebner phenomenon and calciphylaxis has led to debate regarding the hazards of biopsy, including the potential risk of new ulceration, bleeding, and infection. Biopsy can demonstrate medial calcification and intimal proliferation of small arteries, leading to ischemic epidermal necrosis [9]. Sensitivity is improved using special stains such as von Kossa or Alizarin red, for the detection of microcalcification. In the differential diagnosis, warfarin-induced skin necrosis is particularly important and typically responds to warfarin withdrawal. However, surgical debridement may be necessary in some cases.
Patients should discontinue all medications that possibly contribute to CUA, including warfarin, iron, calcium, and vitamin D supplements. Treatment of hypercalcemia and hyperphosphatemia can be achieved with an intensified dialysis regimen and low-calcium dialysate. Severe hyperparathyroidism should be treated with calcimimetics. Sodium thiosulfate, known for its vasodilatory and antioxidant properties, increases calcium solubility to form a dialyzable salt.
Intravenous administration of sodium thiosulfate at a dose of 25 g, given over each hemodialysis, has demonstrated good efficacy [10]. For patients weighing less than 60 kg, reducing doses helps to prevent adverse events such as vomiting, metabolic acidosis, hypotension, and volume overload. Wound management plays a pivotal role in the treatment of calciphylaxis. Therefore, multidisciplinary collaboration between dermatologists, surgeons and burn centers is important to optimize wound care and determine the need for surgical debridement. Prognosis of CUA remains poor with a high mortality rate.
Conclusion
Calciphylaxis or CUA is a rare and potentially lethal disease, mainly affecting patients with end-stage renal disease. The diverse clinical presentations often result in delayed diagnosis. Skin biopsy remains the gold standard for diagnosis and typically reveals calcium deposits within the vessels of the dermis and subcutaneous fat, as well as thrombi and ischemic necrosis. A multidisciplinary approach is essential to assess the need for surgical debridement and optimize wound care. Treatment focuses on improving metabolic control, discontinuing causative medications, and wound care. Additionally, sodium thiosulfate may provide benefit, but further research remains necessary to determine how to optimize care for this devastating disease.
References
- Sagar U, Nigwekar SU. Calciphylaxis. Curr Opin Nephrol Hypertens. 2017; 26(4): 276-281.
- Seyle H, Gentile G, Prioreschi P. Cutaneous molt induced by calciphylaxis in the rat. Sciences. 1961; 134(3493): 1876-7.
- Moe SM, Chen NX. Mechanisms of vascular calcification in chronic kidney disease. J Am Soc Nephrol. 2008; 19(2): 213-6.
- Nigwekar SU, Hadhani R, Brandenburg VM. Calciphylaxis. N Engl J Med. 2018; 378(18): 1704-1714.
- Nigwekar SU, Bloch DB, Nazarian RM, et al. Vitamin K dependent carboxylation of matrix gla protein influences the risk of calciphylaxis. J Am Soc Nephrol. 2017; 28(6): 1717-1722.
- Chen NX, O’Neil K, Akl NK, Moe SM. Adipocyte induced arterial calcification is prevented with sodium thiosulfate. Bio-chem Biophys Resp Commun. 2014; 449(1): 151-156.
- Nigwekar SU, Zhao S, Wenger J, et al. A nationally representative study of calcific uremic arteriolopathy risk factors. J Am Soc Nephrol. 2016; 27(11): 3421-3429.
- Bajaj R, Courbebaisse M, Kroshinsky D, Thadhani RI, Nigwekar SU. Calciphylaxis in patients with normal renal function: a case series and systematic review. Mayo Clin Proc. 2018; 93(9): 1202-12.
- Colboc H, Moguelet P, Bazin D, Carvalho P, Dillies AS, et al. Localization, morphologic features, and chemical composition of calciphylaxis- related skin deposits in patients with Calcemic Uremic Arteriolopathy. JAMA Dermatol. 2019; 155(7): 789-796.
- Garcia CP, Roson E, Peon G, et al. Calciphylaxis treated with sodium thiosulfate: Report of two cases. Dermatol Online J. 2013; 19(9): 19616.
