
Open Access, Volume 10
A noteworthy case of ultrasound guided laparoscopic partial splenectomy for a splenic cystic lymphangioma in a young girl: Case report and review of the literature
Davolio Alessia1*; Alberzoni Chiara3; Giandola Teresa3; Giulia Lo Bianco2; Mauro Alessandro Scotti2; Vimercati Chiara4; Eleonora Colciago2; Braga Marco1,2; Degrate Luca2
1School of Medicine and Surgery, University of Milano-Bicocca, Italy.
2Department of Surgery, Fondazione IRCCS San Gerardo dei Tintori, Monza, Italy.
3Department of Radiology, Fondazione IRCCS San Gerardo dei Tintori, Monza, Italy.
4Pediatrics, Fondazione IRCCS San Gerardo dei Tintori, Monza, Italy.
Davolio Alessia
School of Medicine and Surgery, University of Milano, Bicocca, Italy.
Email: a.davolio@campus.unimib.it
Received : October 26, 2024,
Accepted : November 14, 2024
Published : November 29, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Lymphangioma is a benign neoformation of the lymphatic system that develops in single or multiple cystic structures. Lymphangioma is more common in children, abdominal organs are seldom affected and isolated splenic cysts are extremely rare.
Clinical manifestations of splenic lymphangioma are related to the number of cysts and to their size. While small and isolated cysts are mostly incidentally detected through abdominal imaging, large cystic lesions can cause abdominal discomfort, palpable mass or symptoms from adjacent organs compression.
The treatment of splenic cystic lymphangioma is controversial, surgical splenectomy is recommended in case of symptomatic lesions or rapid growth. Total splenectomy is the traditional route of treatment but carries the risk of Overwhelming Post-Splenectomy Sepsis (OPSI), especially in children. Partial splenectomy is a recently reported technique for splenic lesions that allows both the prevention of recurrences and the preservation of the immune function of the spleen. There are only twenty-one reported cases of patients who underwent surgery for isolated splenic lymphangioma and only one of them was a child.
We report the case of a 14-year-old girl who complained of aspecific recurrent abdominal pain. Abdominal ultrasound showed an anechoic cystic lesion of the superior pole of the spleen. After three years the lesion appeared to have grown, causing splenomegaly. The choice of laparoscopic partial splenectomy with ultrasound guidance over total splenectomy was dictated by the young age, minimal symptoms and long life prospective of the patient. The immunohistochemical staining showed a lymphatic origin of the cyst, confirming the diagnosis of splenic unilocular cystic lymphangioma.
The postoperative period was uneventful. A Contrast Enhanced Ultrasound (CEUS) was performed at five days and at 12 months after surgery showing a normal perfusion of the residual spleen parenchyma and the absence of recurrent splenic cysts.
Our case focuses on the management of this very rare condition in a young girl by laparoscopic partial splenectomy with intraoperative ultrasound guidance. The postoperative follow-up was performed with CEUS. We also reviewed the existing literature about partial splenic resection and the application of intraoperative ultrasound and postoperative CEUS as tools to perform a successful surgery.
Keywords: Lymphangioma; Splenic cyst; Laparoscopic partial splenectomy; Laparoscopic total splenectomy; CEUS; IOUS; Children.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Alessia D(2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Alessia D, Chiara A, Teresa G, Bianco GL, Scotti MA, Chiara V, Colciago E, et al. A noteworthy case of ultrasound guided laparoscopic partial splenectomy for a splenic cystic lymphangioma in a young girl: Case report and review of the literature. Open J Clin Med Case Rep. 2024; 2302.
Introduction
Lymphangioma is a benign neoformation of the lymphatic system that is characterized by the abnormal development of lymphatic vessels in single or multiple cystic structures. The most frequent location sites are the neck (75%), the axilla (20%), the orbit and the bones. Abdominal organs are rarely affected and, notably, isolated splenic cystic lymphangioma is an extremely rare condition [1-4]. In case of multiple organs involvement we can have a lymphangiomatosis syndrome, such as Klippel-Trenaunay syndrome. Lymphangioma occurs more frequently in children [4] with almost 85% of reported cases involving patients of less than 2 years of age and only rare occurrences in adults [5].
The treatment of splenic cystic lymphangioma is controversial, however, splenectomy is recommended in case of lesion-related symptoms or rapid growth. There are only twenty-one reported cases of surgery for isolated splenic lymphangioma in literature and only one of them was a child. Partial splenectomy is a recently reported technique for splenic lesions that allows both the prevention of recurrences and the preservation of the immune function of the spleen [1]. Our case reports the management of an isolated cystic lymphangioma in a young girl by laparoscopic partial splenectomy achieved with Intraoperative Ultrasound (IOUS) guidance. We choosed Contrast Enhanced Ultrasonography (CEUS) for postoperative follow-up surveillance. A review of the Literature has also been conducted.
Case Presentation
We report the case of a 14-year-old girl who complained of aspecific recurrent abdominal pain. An abdominal ultrasound was performed, showing an anechoic cystic lesion of 14 mm of diameter in the superior pole of the spleen, without evidence of splenomegaly. We started an annual follow-up and after three years the ultrasound showed an increase in size of the splenic cyst, reaching 97 mm of diameter. The subsequent diagnostic work-up included blood exams that were found normal and a negative serology for Echinococcus granulosus. We also performed an abdominal Magnetic Resonance (MR) and Computed Tomography (CT) that showed a cystic lesion at the upper pole of the spleen, characterized by a single thin wall with a low density fluid content and multiple septa. The size of the cyst was 11x9x9 cm with no evidence of calcifications or further splenic lesions. The bipolar diameter of the spleen was 14.5 cm, with a compression of the stomach and dislocation of the left kidney (Figures 1,2). Based on to the radiological findings and on the progressive growth of the lesion we suspected a diagnosis of isolated splenic cystic lymphangioma.
We scheduled a multidisciplinary discussion with surgeons, radiologists and paediatricians and decided to manage the cystic lesion by laparoscopic partial splenectomy with ultrasound guidance. The patient had been previously vaccinated for encapsulated bacteria and was prescribed perioperative antibiotic prophylaxis with cefazoline and anti-thromboembolic prophylaxis with enoxaparin. The operation was performed under general anaesthesia. The patient was placed in a supine position on the operative table and we placed four trocars (three 5 mm trocar and one 15 mm trocar) as described in previous works [6]. The exploration of the abdomen showed a cystic lesion of the upper pole of the spleen (Figure 3). IOUS was performed, marking the margins of the lesion and confirming the absence of further cysts. After division of the gastrosplenic ligament and mobilization of the posterior spleen’s attachments, we emptied the cystic lesion with a needle and collected about 50 ml of clear fluid. We coagulated the feeding vessels with a radiofrequency device (LigaSure™ Medtronic) keeping a 1 cm distance from the margin of the lesion as identified with IOUS until we obtained an ischemic demarcation of the splenic parenchyma. The transection of the parenchyma was then performed, under IOUS guidance, using the radiofrequency device. A bipolar coagulation device (Aquamantys™ bipolar sealers Medtronic) was used for haemostasis (Figure 4). The residual spleen was estimated to be about a third of the entire initial splenic volume (Figure 5). A laparoscopic stitch was placed in order to fix the remaining spleen to the omentum and avoid a possible torsion of the pedicle’s vessels and subsequent ischaemia of the residual organ.
The surgical specimen (Figure 6) was extracted with an endobag through the 15 mm incision and a drainage was placed in the splenic bed. The postoperative period was uneventful. A CEUS was performed five days after surgery showing that the residual spleen maintained a normal perfusion of the parenchyma [7]. At 12-month follow up, CEUS confirmed the absence of recurrent splenic cysts and the normal perfusion of the remnant spleen (Figure 7).
The histological analysis showed the presence of one single cystic lesion; the immunohistochemical staining revealed the lymphatic origin of the cyst, confirming the diagnosis of splenic unilocular cystic lymphangioma.
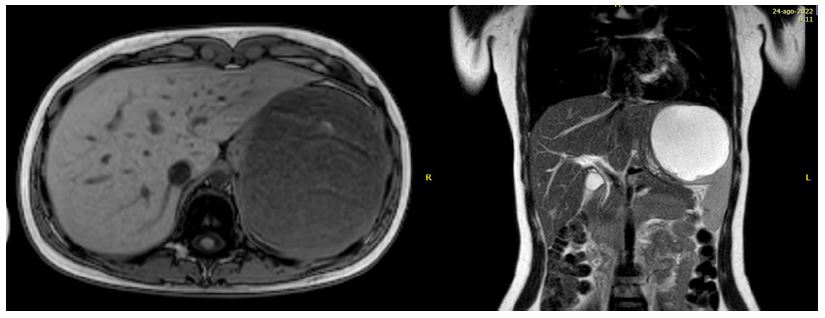
Figure 1: FluoroscopyPreoperative abdominal MR: Splenomegaly with cystic lesion of the upper pole of the spleen with a thin wall, septa, characterized by hyperintensity in T2 weighted images and hypointensity at T1 weighted imaging.
Table 1: Literature reported cases of isolated splenic lymphangioma (LTS laparoscopic total splenectomy, LPS laparoscopic partial splenectomy, OTS open total splenectomy, TS total splenectomy).
| Reference | Year | Age | Gender | Symptoms | Dimensions | HistopathologicalDiagnosis | Single/ multiplecyst | Type of surgery | Pre/post-surgeryenhanced ultrasound | Recurrences andcomplications |
|---|---|---|---|---|---|---|---|---|---|---|
| [26] | 2001 | 69 | F | NO | 5x3 cm,2x2,5 cm | Lymphangioma | Multiple | LTS | NO | - |
| [12] | 2007 | 26 | F | YES | 3 cm | Lymphangioma | Single | LTS | NO | NO |
| [12] | 2007 | 30 | F | YES | 4,5 cm | Lymphangioma | Single | LTS | NO | NO |
| [12] | 2007 | 40 | F | YES | 6 cm | Lymphangioma | Multiple | LTS | NO | NO |
| [11] | 2007 | 46 | F | YES | 4 cm | Lymphangioma | Single | OTS | NO | NO |
| [10] | 2012 | 59 | F | YES | 2 cm | Lymphangioma | Single | LTS | NO | NO |
| [15] | 2012 | 67 | M | NO | 6 cm | Lymphangioma | Single | Not done | YES | - |
| [13] | 2013 | 30 | F | YES | - | Lymphangioma | Single | OTS | NO | - |
| [25] | 2014 | 22 | M | - | 4,2 cm | Lymphangioma | Single | LPS | NO | - |
| [16] | 2016 | 28 | F | NO | 1,2x1,4 cm | Lymphangioma | Single | OTS | NO | - |
| [25] | 2014 | 47 | F | - | 4,4 cm | Lymphangioma | Single | LPS | NO | - |
| [25] | 2014 | 56 | F | - | 4 cm | Lymphangioma | Multiple | LPS | NO | - |
| [9] | 2015 | 41 | F | NO | 3,5 cm | Lymphangioma | Single | LTS | NO | - |
| [21] | 2015 | 51 | F | YES | 1,5x1 cm | Lymphangioma | Single | LPS | NO | NO |
| [14] | 2015 | 64 | F | NO | 12x9x9 cm | Lymphangioma | Single | OTS | NO | NO |
| [16] | 2016 | 6 | M | YES | 1x 1.5cm, 1x2 cm, 1x3 cm | Lymphangioma | Multiple | LTS | NO | - |
| [16] | 2016 | 70 | F | NO | 0,8 cm (max diameter) | Lymphangioma | Multiple | OTS | NO | - |
| [5] | 2017 | 34 | F | YES | 2,5x2,5 cm | Lymphangioma | Single | OTS | NO | NO |
| [4] | 2018 | 40 | F | YES | 25 cm | Lymphangioma | Single | OTS | NO | NO |
| [3] | 2019 | 63 | F | YES | - | Lymphangioma | Multiple | OTS | NO | NO |
| [1] | 2020 | 18 | F | YES | 6 cm | Lymphangioma | Single | LPS | NO | NO |
| [29] | 2022 | 73 | F | YES | 19x11x7 cm | Lymphangioma | Single | TS | NO | NO |
| OUR CASE | 2023 | 15 | F | YES | 11x9x9 cm | Lymphangioma | Single | LPS | YES | NO |
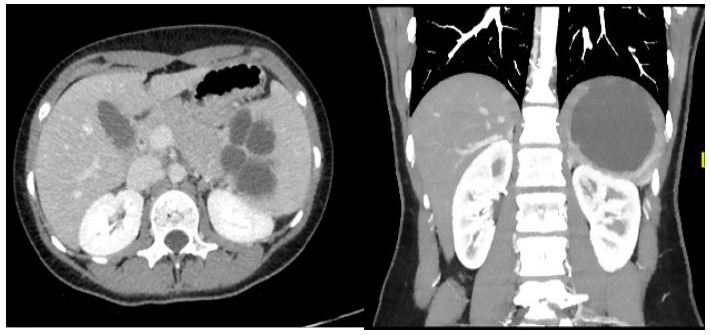
Figure 2: Preoperative abdominal CT scan: Compression of the stomach and dislocation of the left kidney due to splenomegaly and a cystic lesion with single thin wall, low density fluid content and multiple septa. No calcifications are present.

Figure 3: Laparoscopic view of the cystic lymphangioma ot the upper splenic pole.
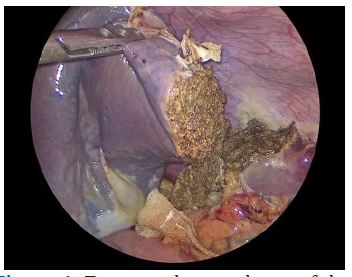
Figure 4: Transected parenchyma of the residual spleen.
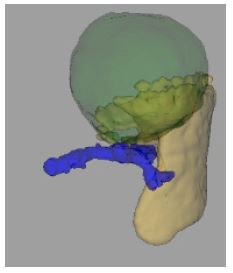
Figure 5: CT-based calculation of the volume of splenic parenchyma (yellow colour) and cyst (green colour) using Philips HealthCare® Program. The splenic vein is indicated with the blue colour.

Figure 6: The surgical piece: anterior surface of the upper splenic pole with the cystic lesion.
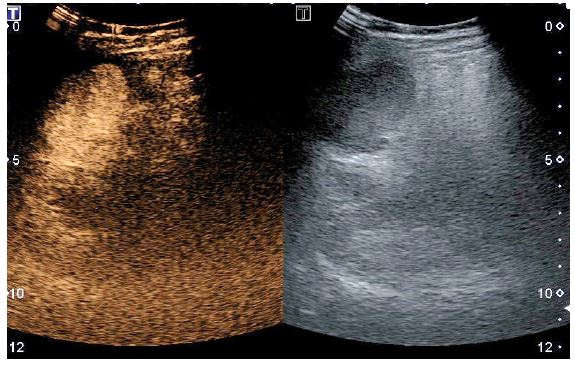
Figure 7: Contrast enhanced ultrasonography 12 months after surgery.
Discussion
Cystic lymphangioma is a congenital benign condition due to the malformation of the lymphatic system, characterized by confluent, dilated, thin-walled, fluid filled cystic structures that could be in single or multiple formations. No consensus has yet been reached on whether lymphangioma is a neoplasm or a hamartoma [8,9]. The incidence of this condition is higher in children, while the single localization in the splenic parenchyma is extremely uncommon.
The clinical manifestations of the splenic lymphangioma are related to the number of cysts and to their size. Small and isolated cysts are most commonly incidentally detected through abdominal ultrasonography or abdominal CT, while large cystic lesions can cause abdominal discomfort, palpable mass or symptoms from compression of adjacent organs, like stomach or kidneys [2].
At ultrasonography, splenic lymphangioma appears as a hypoechoic or anechoic lesion with possible septations and calcifications. Color Doppler ultrasonography can be useful to rule out intrinsic cystic vascularization. CT analysis can show single or multiple low-density cysts, with a «swiss cheese» appearance in the case of multiple cystic lymphangioma [10].
MR and CT are shown to have similar sensibility, while MR is employed to identify possible areas of malignant degeneration [3,11,12]. Only two cases of splenic lymphangioma have been reported to appear as solid lesions with diffuse and prolonged enhancement at CT scan or as an inhomogeneous, mostly hyperechoic, septated masses at ultrasonography: a histopathological evaluation was mandatory in these cases to clarify the radiological findings [13,14].
Histopathological classification divides splenic lymphangiomas into capillary, cavernous or cystic based on the size of the dilated channels. The distinction is not always clear and is not uniformly accepted among pathologists. The cystic type is the most frequent [5,15]. The immunohistochemical analysis allows to confirm the lymphatic derivation: the lymphatic endothelial component showing positive results for podoplanin antibody, CD34, CD31 and FVIII.
Because of its variable presentation, the definitive diagnosis of cystic splenic lymphangioma should be based on a sum of clinical, radiological, and histopathological elements [11]. Cystic lymphangiomas must be differentiated from other cystic lesions of the spleen, that are generally classified in primary and secondary cysts. Secondary cysts (pseudocysts) account for nearly 80% of all splenic cystic lesions. They usually develop after trauma or previous infection or infarction. Histologically, they are lined by a fibrous wall without specific lining cells. Primary cysts are classified into parasitic (60%) and non-parasitic cysts. Parasitic cysts are mostly caused by echinococcal infection. Non-parasitic cysts commonly include epithelial cysts (epidermoid and mesothelial cysts), haemangiomas and lymphangiomas. Haemangiomas and lymphangiomas are histologically positive to the same endothelial markers except D2-40, which is only positive in lymphangioma [5]. The possibility of malignant transformation is reported only in few cases [3,16].
The treatment of splenic cystic lymphangioma is controversial. A medical conservative treatment of splenic lymphangioma with alpha interferon has been described and showed good tolerance in children, but no consensus has yet been found on the dosage and period of treatment [3,17]. Other therapeutic modalities including drainage and aspiration have shown unsatisfactory results [18-20]. Complete surgical resection is considered the best treatment in case of lesion-related symptoms or rapid growth. The rate of recurrence after surgical resection is very low, reaching 9.5% in case of incomplete resection [2,20].
Laparoscopic splenectomy is increasingly advocated as a minimally invasive and safe technique to treat splenic lesions. As opposed to the open approach, it requires more technical skills, longer operative time and adequate materials and it may be contraindicated, or difficult to perform, in patients with massive splenomegaly [1,2,4,5,7,19,21,22]. Laparoscopic splenectomy in the paediatric age group is generally considered a highly demanding procedure owing to the limited abdominal space, the fragility of the splenic tissue and the relative rarity of splenic disease [23]. On the other hand, the laparoscopic approach has demonstrated, both in adults and paediatric patients, lower morbidity, shorter hospitalisation, reduction of the pain and a better cosmetic outcome with less wound dehiscence and infections than open splenectomy [24,25]. To remove splenic lesions, total splenectomy has been the traditional choice, but this option carries the risk of Overwhelming Post-Splenectomy Sepsis (OPSI), especially in children, with an incidence of 4.4%, and a mortality risk of approximately 50-80% [1,12,23,26]. Partial splenectomy allows for both the prevention of recurrences and the preservation of the immune function of the spleen. According to literature, patients undergoing partial resection can maintain an efficient immune system and avoid OPSI as long as 25% volume of the initial total spleen is preserved [21,23,27]. Only one case of OPSI after partial splenectomy is reported in literature, but in that case the remaining splenic parenchyma was only about 20% [7]. The choice between total or partial splenectomy depends on the size of the lesion, on the amount of healthy remnant parenchyma and on the proximity of the lesion to splenic vessels. Recent studies suggest that a transection of the splenic parenchyma keeping a 1 cm margin from the line of ischemic demarcation (obtained after ligation of the lesion feeding vessels) is an effective way to minimise blood loss [7]. Besides bleeding, another potential postoperative complication in case of partial splenectomy is called “wandering spleen”: An intermittent or acute spontaneous torsion of the remaining splenic vessels that may cause different degrees of abdominal pain.
In our case, we opted for a laparoscopic partial splenectomy over total splenectomy, despite the initial splenomegaly, because of the young age, minimal symptoms and long life prospective of the patient. In our case, the choice of performing a partial resection allowed us to leave a sufficient volume of spleen parenchyma to protect the young patient from the risk of OPSI and to maintain a functioning and performing immune system.
The surgery was performed with IOUS guidance to accurately define the anatomical limits of the lesion. This enabled us to perform a radical resection limiting the risk of recurrence while sparing the healthy parenchyma.
We chose CEUS for follow up surveillance to limit the patient’s exposition to rays and ionising radiations [18]. CEUS is regarded as safe and effective in children, according to the limited available data: The contrast agent of the CEUS technique has less adverse effects than the radiocontrast agents used for the CT scans and has a safety comparable to the MR contrast agent. Also, the setting of an ultrasonography is considered “patient-friendly” [28].
Our case reports the management of a very rare isolated unilocular cystic lymphangioma in a young girl by laparoscopic partial splenectomy, using IOUS and postoperative follow-up with CEUS: It appears to be the first case in Literature managed in a such way (Table 1) [1]. From a literature review, in the majority of the reported cases, patients arrived at the surgeon’s attention with non-specific abdominal symptoms. Only twenty-two patients who underwent surgery for splenic lymphangioma have been reported in literature including our own, and only two of them were children. The histological and immunohistochemical analysis of these cases confirmed the diagnosis of lymphangioma. In 16 cases it was a single cystic lymphangioma, and in 6 cases a multiple cystic lymphangioma. In a single case the diagnosis was made based on a splenic biopsy without surgery: It was the case of a patient with a history of two colonic tumours for whom the possibility of a splenic surgery was contraindicated.
The size of the lesions appears to be very variable as also their location within the splenic parenchyma. Total splenectomy was performed in ten cases of single cystic lymphangioma while only in five cases patients underwent a partial splenectomy. In multiple cystic lymphangioma only one patient out of six had been treated with partial splenectomy while the other required total splenectomy. The laparoscopic technique is reported in Literature as the most used: thirteen cases overall as opposed to eight cases managed with the open technique. Looking at these results, it appears that the laparoscopic technique may become the surgical method of choice.
As far as the choice between total and partial splenectomy is concerned, despite the benefits of partial spleen preservation in terms of immune response and better impact on the patient’s quality of life, there are still many limitations and difficulties like the necessity to maintain a vital remaining volume, the increased risk of bleeding and the technical difficulties. In fact, total splenectomy is still very common. No complications or recurrences were reported in any of the articles.
In addition, besides our case, perioperative CEUS was reported to be used only for diagnostic purpose in one patient that had not been candidate to surgery [15].
Conclusion
Lymphangioma is a benign disease that mainly affects the paediatric population, its presentation as a sole splenic lesion is unusual and it’s reported in Literature only in a few cases. Indications over diagnosis and treatment of this benign splenic lesion are still controversial, surgery is considered the first choice in terms of efficacy and radicality, but there are still cases in which it is contraindicated. The choice of surgical technique is also evolving: laparoscopy, thanks to developments both in terms of technique and instruments, may be preferable to the open technique and scores better outcomes in terms of morbidity, hospitalization time, cosmetic results, wound infection and wound dehiscence prevention and pain management. In addition, partial splenectomy may allow to maintain the full function of the patients’ immune system and to prevent OPSI which should be taken into consideration especially in the case of a young patient. In conclusion, according to our experience, we consider laparoscopic partial splenectomy a safe and effective way to treat a benign but symptomatic condition in a young patient with cystic lymphangioma. We would also advise the employ of IOUS and postoperative follow up CEUS especially in children.
Abbreviations: CEUS: Contrast Enhanced Ultrasonography; IOUS: Intraoperative Ultrasound; MR: Magnetic Resonance; CT: Computed Tomography; OPSI: Overwhelming Post-Splenectomy Sepsis; OTS: Open Total Splenectomy; LPS: Laparoscopic Partial Splenectomy; LTS: Laparoscopic Total Splenectomy.
References
- Kimura K, Kurashima Y, Tanaka K, Asano T, Ebihara Y, et al. Laparoscopic partial splenectomy for splenic lymphangioma: a case report. Surg case report. 2020; 6: 140.
- Ioannidis I, Kahn AG. Splenic lymphangioma. Arch Path Lab Med. 2015; 139(2): 278-282.
- Ousmane T, Mamadou FP, Sitor SI, Abdou N, Madieng D. Splenic lymphangioma. Int J Surg Case Rep. 2019; 62: 40-42.
- Efared B, Atsame-Ebang G, Zabeirou A, Hammas N, Mazaz K, et al. Isolated splenic lymphangioma presenting as a huge mass causing anemia and abdominal distension in an adult patient: A case report. J Med Case Rep. 2018; 12(1): 97.
- Al-Shaikh SA, Mubarak AM, Harb ZF. Splenic lymphangioma in an adult. Saudi Med J. 2017; 38(11): 1148-1152.
- Degrate L, Zanframundo C, Bernasconi DP, Real G, Garancini M, et al. Futility of abdominal drain In elective laparoscopic splenectomy. Langenbecks Arch Surg. 2020; 405(5): 665-672.
- De la Villeon B, Zarzavadjian Le Bian A, Vuarnesson H, Munoz Bongrand N, Halimi B, et al. Laparoscopic partial splenectomy: a technical tip. Surg Endosc. 2015; 29: 94-99.
- Kim N, Auerbach A, Manning MA. Algorithmic Approach to the Splenic Lesion Based on Radiologic Pathologic Correlation. Radiographics. 2022; 42(3): 683-701.
- Kim SY, Kwon HJ, Park HW, Lee SY, Son BH, et al. Multiple cystic lymphangiomas of the spleen: radiologic and histopathologic findings. J Med Ultrason. 2015; 42(3): 409-412.
- Crema E, Etchebehere RM, Gonzaga MN, Lima RS, Bertulucci PA, et al. Splenic lymphangioma: A rare benign tumor of the spleen treated by laparoscopic surgery. Arq Bras Cir Dig. 2012; 25(3): 178-179.
- Chang WC, Liou CH, Kao HW, Hsu CC, Chen CY, et al. Solitary lymphangioma of the spleen: dynamic MR findings with pathological correlation. Br J Radiol. 2007; 80(949): e4-6.
- Barbaros U, Deveci U, Ozlük Y, Tiriyaki B, Erbil Y, et al. Laparoscopic treatment of splenic lymphangiomas: Report of three cases. G Chir. 2007; 28(10): 403-6.
- Yang F, Chen WX. Splenic lymphangioma that manifested as a solid-cystic mass: A case report. World Journal of Gastroenterology : WJG. 2013; 19 (5): 781.
- Roman A, Iancu C, Andreica V, Socaciu M, Anton O, et al. Splenic cystic lymphangioma with atypical ultrasound findings. J Med Ultrasonics. 2016; 43: 99-105.
- Eghtedari M, Sicklick J, Kono Y, Peterson MR, Santillan CS. Unusual imaging profile of a solitary splenic lymphangioma. Acta Radiol Short Rep. 2012; 1(8).
- Rodríguez-Montes JA, Collantes-Bellido E, Marín-Serrano E, Prieto-Nieto I, Pérez-Robledo JP. Linfangioma esplénico. Un tumor raro. Presentación de 3 casos y revisión de la bibliografía. Cirugía y Cirujanos 2016; 84(2): 154-159.
- Masuya R, Nakame K, Tahira K, Kai K, Hamada T, et al. Laparoscopic dome resection for pediatric nonparasitic huge splenic cyst safely performed using indocyanine green fluorescence and percutaneous needle grasper. Asian J Endosc Surg. 2022; 15(3): 693-696.
- Yu X, Yu J, Liang P, Liu F. Real-time contrast-enhanced ultrasound in diagnosing of focal spleen lesions. Eur J Radiol. 2012; 81(3): 430-6
- Makrin V, Avital S, White I, Sagie B, Szold A. Laparoscopic splenectomy for solitary splenic tumors. Surg endosc. 2008; 22(9): 2009-2012.
- Chung SH, Park YS, Jo YJ, Kim SH, Jun DW, et al. Asymptomatic lymphangioma involving the spleen and retroperitoneum in adults. World J Gastroenterol. 2009; 15(44): 5620-5623.
- Wang WD, Lin J, Wu ZQ, Liu QB, Ma J, et al. Partial splenectomy using a laparoscopic bipolar radiofrequency device: A case report. World J Gastroenterol. 2015; 21(11): 3420-4.
- Maurus CF, Schäfer M, Müller MK, Clavien PA, Weber M. Laparoscopic versus open splenectomy for nontraumatic diseases. World J Surg. 2008; 32(11): 2444-9.
- Qingjiang C, Wang L, Chen X, Zhang Y, Zhang L, et al. Laparoscopic management of benign splenic tumors in children. World J Pediatr Surg. 2022; 5(4): e000419.
- Zhang Y, Chen XM, Sun DL, Yang C. Treatment of hemolymphangioma of the spleen by laparoscopic partial splenectomy: A case report. World J Surg Oncol. 2014; 12: 60.
- Wang X, Wang M, Zhang H, Peng B. Laparoscopic partial splenectomy is safe and effective in patients with focal benign splenic lesion. Surg Endosc. 2014; 28(12): 3273-8.
- Kwon AH, Inui H, Tsuji K, Takai S, Imamura A, et al. Laparoscopic splenectomy for a lymphangioma of the spleen: report of a case. Surg Today. 2001; 31(3): 258-61.
- Goldthorn JF, Schwartz AD, Swift AJ, Winkelstein JA. Protective effect of residual splenic tissue after subtotal splenectomy. J Pediatr Surg 1978; 13(6D): 587-590
- Sidhu PS, Cantisani V, Deganello A, Dietrich CF, Duran C, et al. Role of Contrast-Enhanced Ultrasound (CEUS) in Paediatric Practice: An EFSUMB Position Statement. Ultraschall Med. 2017; 38(1): 33-43.
- Hussein Al-Janabi M, Abodest R, Adnan Alshabab M, Kannan S, Issa R. Splenic cystic lymphangioma in adults: A rare case report from Syria. Ann Med Surg (Lond). 2022; 80: 104152.
