
Open Access, Volume 10
Bilateral breast metastasis originating from alveolar rhabdomyosarcoma
Kristian Bugeja*; Denise Hili; Serkan Ilgun; Michelle Ceci; Sandro Galea Soler; John Agius
Mater Dei Hospital, Malta.
Kristian Bugeja
Mater Dei Hospital, Malta.
Email: bugejakristian1232@gmail.com
Received : October 15, 2024,
Accepted : November 12, 2024
Published : November 29, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Metastasis to the breast from other primary sites is extremely rare. We present the case of a 19-year- old pregnant female with right forearm alveolar rhabdomyosarcoma who developed bilateral breast metastases during follow-up. After the diagnosis of primary rhabdomyosarcoma, the patient underwent neoadjuvant chemotherapy followed by primary tumour excision, which included sacrificing the ulnar nerve. During follow-ups, bilateral breast masses were detected, and biopsy results confirmed sarcoma metastasis. The patient then underwent a course of chemotherapy, which resulted in a clinical complete response, followed by a bilateral mastectomy as part of the management strategy. The patient’s ongoing surveillance protocol and the multidisciplinary approach adopted for her treatment highlight the complexities involved in treating metastatic rhabdomyosarcoma. This report underscores the rarity of breast metastases and the unique challenges faced in managing such a case during pregnancy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Bugeja K (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Bugeja K, Hili D, Ilgun S, Ceci M, Galea Soler S, Agius J. Bilateral breast metastasis originating from alveolar rhabdomyosarcoma. Open J Clin Med Case Rep. 2024; 2301.
Introduction
Rhabdomyosarcoma (RMS) is a rare soft tissue malignancy primarily affecting children, but its occurrence in adults can present unique diagnostic and therapeutic challenges. This case report presents an alveolar subtype of RMS in a 19-year-old female, initially presenting with a forearm mass. The rarity of this case is underscored by the subsequent discovery of metastases to the breasts, an uncommon site for RMS dissemination. This introduction sets the stage for a detailed exploration of the clinical approach to managing these unusual breast metastases, emphasizing the necessity for vigilance and a tailored therapeutic strategy in such atypical presentations.
Case Report
In January 2022, a 19-year-old pregnant female in her 36th week of pregnancy presented with a mass in the right forearm. The mass was investigated using Magnetic Resonance Imaging (MRI), the results of which are shown in Figures 1 and 2, revealing a suspicious lesion in the forearm flexor compartment. A subsequent biopsy was performed, and histopathological analysis confirmed the diagnosis of alveolar rhabdomyosarcoma as can be seen in Figure 3.
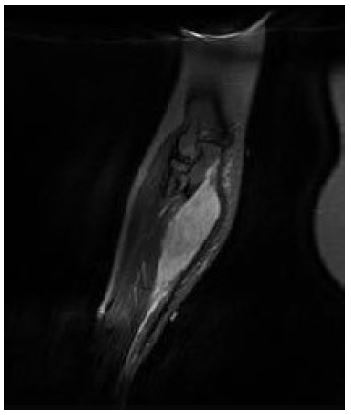
Figure 1: Coronal large field of view Proton Density, Fat Suppressed (PD FS) image demonstrating a homogeneously fluid hyper intense lesion at the medial aspect of the right forearm.
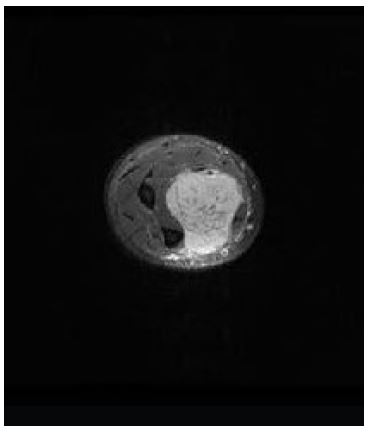
Figure 2: Axial diffuse weighted imaging through the patient’s right forearm demonstrating restricted intralesional diffusion, highlighting underlying hypercellularity.
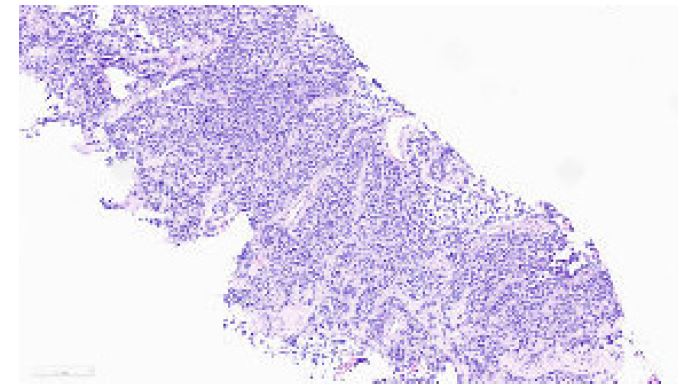
Figure 3: Core biopsy reveals cohesive nests of small cells exhibiting a high nuclear to cytoplasmic ratio and hyperchromatic nuclei. Notably, rhabdoid differentiation is observed a long side brisk mitotic activity.
Following the delivery of her baby via induction in mid-February 2022, an MDT discussion recommended a staging PET-CT scan, which showed no further uptake in other areas of the body, indicating no additional metastasis. In view of this, she began three months of neoadjuvant chemotherapy as part of the IVADo regimen, which included ifosfamide, vincristine, actinomycin D, and doxorubicin. By May 2022, she had completed a total of four cycles. The tumor was excised en bloc, including the ulnar nerve, ulnar artery, parts of the flexor muscle groups, and the periosteum of the ulnar shaft. This was followed by a nerve transfer from the motor branch of the median nerve to the distal end of the ulnar motor nerve and subsequent physiotherapy. Following MDT discussion, the patient was noted to have an excellent clinical and radiological response to chemotherapy. However, a poor histological response was observed, with more than 85% viable cells remaining in the specimen post-surgery. For this reason, post-operative radiotherapy, rather than chemotherapy, was recommended.
In September 2022, a CT scan of the thorax, abdomen, and pelvis was performed for re-staging. While no pulmonary disease was detected, the scan revealed four suspicious breast nodules (two on each side), as shown in Figure 4. A biopsy later confirmed these nodules to be metastatic sarcoma, identical to the forearm mass, with pathology slides presented in Figures 5 and 6. Prior to the mastectomy, the patient received six rounds of VIT chemotherapy, which included vincristine, irinotecan, and temozolomide. Subsequently, a bilateral mastectomy with partial excision of the pectoralis major muscle was performed in March 2023. The procedure was successful, and no complications were reported. The patient was subsequently referred to physiotherapy.

Figure 4: Axial CT scan revealing bilateral breast metastatic deposits.
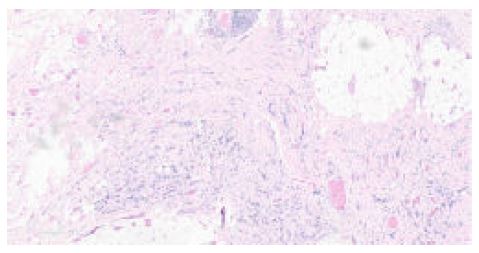
Figure 5: A section from the affected breast.

Figure 6: A low-power view reveals the breast.
The patient re-presented in early May 2023 with a palpable mass in the distal right arm, located proximal to the field of the previous sarcoma excision. This raised concern for recurrence or a new malignancy, and an MRI of the right upper limb was performed to further investigate. The MRI included T1-weighted, T2-weighted, and fat-suppressed contrast-enhanced sequences of the distal arm. The scans revealed a mass in the anteromedial aspect of the distal arm, suspicious for malignancy, as can be seen in Figure 7. The lesion appeared heterogeneously hyperintense on T2- weighted images and demonstrated irregular contrast enhancement, consistent with a possible sarcomatous recurrence. No direct invasion into the surrounding bone or neurovascular structures was noted. Further evaluation, including biopsy, was recommended to confirm the nature of the mass.
The biopsied lesion showed features of rhabdomyosarcoma identical to those reported previously. PET scan confirmed disease recurrence proximal to the right antecubital fossa with no new abnormalities in the rest of the body segments. The patient underwent an excision of the lesion with nerve transfer in September 2023 and is currently receiving further chemotherapy.
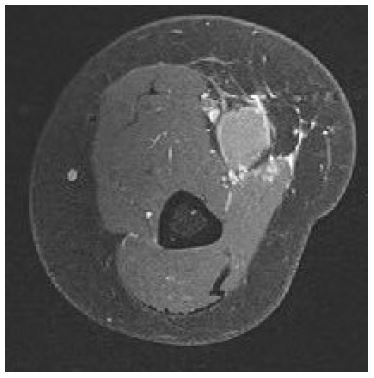
Figure 7: MR study indicating recurrence at the level of the medial upper arm.
Discussion
This case emphasises the complex management decisions faced in treating rhabdomyosarcoma.
The occurrence of metastases in the bilateral breasts postoperatively led to a shift in the management plan, highlighting the importance of ongoing surveillance and adaptability in managing this rare malignancy.
Surveillance following the MDT meeting includes biannual surgical site evaluations with serial MRIs of the forearm for three years, followed by annual assessments for a minimum of two additional years. This comprehensive follow-up strategy aims to detect potential recurrences and metastases early, ensuring timely intervention and optimal patient outcomes. The unique challenges and decisions faced in this case underscore the importance of a multidisciplinary and adaptable approach in managing rare and complex oncological scenarios.
Metastatic breast malignancies are very uncommon, with rates of 0.5% to 3%. Metastasis to the breast has been demonstrated from primary tumours such as mesotheliomas, malignant melanomas, appendiceal carcinoid, epidermoid cervical carcinoma, and rhabdomyosarcoma [1,2]. Identifying the histological type is necessary for optimal management and prescribing the appropriate systemic therapy. In our case, sarcoma metastases were detected in both breasts during follow-up, and upon receiving a good response to chemotherapy, bilateral mastectomy was performed.
Xia Bai et al. described the solitary breast metastasis of RMS from the maxillary sinus in a 15-year- old premenarchal female [3]. Similarly, Hongmei Liu et al. [4] described breast metastasis from RMS of the paranasal sinuses and nasopharynx in a 42-year-old Asian female. D M Hays et al. [5] claimed that metastasis of Alveolar Rhabdomyosarcoma (ARMS) to breast tissue may indicate more unfavorable out comes. They compared 26 patients with breast RMS (both as primary (7) or secondary tumours (19)) with 47 patients from other literature reviews. Alveolar type was far more common (24 cases) than embryonal type (1 case). All patients were female, with a median age of 15.2 years. Marie Luporsi et al. [6] described a case of a 38-year-old female whose breast RMS metastasis was the initial presentation, with further tests and imaging locating the primary soft tissue mass in the distal lower limb. S P Jung et al. [7] discussed a case of an adolescent female having breast RMS metastasis from an anal primary. The breast mass was diagnosed after receiving radio-chemotherapy for the anal lesion.
R Kebudi et al. [8] discussed three cases of adolescent girls having breast metastasis from ARMS. In their literature review, they quoted 70 reported cases of such presentations, with only one patient being male. Commonly, these were treated with chemotherapy, surgery, and then radiotherapy. However, most cases had a very poor prognosis.
Sarcomas and other soft tissue tumours are rarely diagnosed in pregnancy. Between 1963 and 2014, 137 cases have been well documented in the worldwide English literature [9]. This makes the management of such malignancies more difficult, as chemotherapeutic agents are teratogenic, lethal, or may result in developmental malformations, especially when administered in the first trimester. Some chemotherapy may be considered in the second trimester. Hormonal medication cannot be used, and radiotherapy to the mother’s trunk will result in lethal effects on the foetus. Sarcomas are not known to metastasise to the fetus or products of conception. G Zarkavelis et al. described 14 cases of gestational RMS reported in the past 45 years.
This literature review demonstrates the rarity of RMS during gestation, especially those presenting with breast metastasis. In view of this, regular screening of mammary glands is recommended in adolescent females with known RMS [10].
Conclusion
This case report highlights the extraordinary rarity of bilateral breast metastases originating from alveolar rhabdomyosarcoma, particularly in the context of pregnancy. The clinical journey of the patient underscores the unique diagnostic and therapeutic challenges faced in such uncommon presentations. The successful management, involving a combination of neoadjuvant chemotherapy, surgical excision, and rigorous follow-up, demonstrates the importance of a multidisciplinary approach. This case serves as a critical reminder of the necessity for ongoing surveillance in patients with metastatic rhabdomyosarcoma and the potential for atypical metastatic sites, such as the breasts.
Abbreviations: RMS: Rhabdomyosarcoma; MRI: Magnetic Resonance Imaging; CT: Computed Tomography; PET-CT: Positron Emission Tomography - Computed Tomography; MDT: Multidisciplinary Team; PET-CT: Positron Emission Tomography - Computed Tomography; IVADo: Ifosfamide Vincristine Actinomycin D Doxorubicin; VIT: Vincristine Irinotecan, Temozolomide; ARMS: Alveolar Rhabdomyosarcoma.
Declarations
Patient consent: Informed consent was obtained from the patient for the publication of this case report and accompanying images. The patient has agreed to share her medical history and treatment details to contribute to the understanding and management of similar cases.
Conflict of interest: The authors declare no conflict of interest regarding the publication of this case report. All authors have approved the final manuscript and have no financial or personal relationships that could inappropriately influence the content of this paper.
References
- Vergier B, Trojani M, de Mascarel I, Coindre JM, Le Treut A. Metastases to the breast: Differential diagnosis from primary breast carcinoma. J Surg Oncol. 1991; 48(2): 112-6. doi: 10.1002/jso.2930480208.
- Sheen-Chen SM, Eng HL, Ko SF. Metastatic rhabdomyosarcoma to the breast. Anticancer Res. 2005; 25(1B): 527-9. PMID: 15816623.
- Bai X, Wang X. Solitary Breast Metastasis From Rhabdomyosarcoma Shown on FDG PET/CT. Clin Nucl Med. 2018; 43(7): 556-558. doi: 10.1097/RLU.0000000000002125.
- Liu H, Zhao W, Huang M, Zhou X, Gong Y, et al. Alveolar rhabdomyosarcoma of nasopharynx and paranasal sinuses with metastasis to breast in a middle-aged woman: A case report and literature review. Int J Clin Exp Pathol. 2015; 8(11): 15316-21. PMID: 26823887; PMCID: PMC4713673.
- Hays DM, Donaldson SS, Shimada H, Crist WM, Newton WA, et al. Primary and metastatic rhabdomyosarcoma in the breast: Neoplasms of adolescent females, a report from the Intergroup Rhabdomyosarcoma Study. Med Pediatr Oncol. 1997; 29(3): 181-9. doi: 10.1002/(sici)1096-911x(199709)29:3<181::aid-mpo4>3.0.co;2-9.
- Luporsi M, Cassou-Mounat T, Amiot HM, Laurence V, Jehanno N. Rhabdomyosarcoma Revealed by a Breast Metastasis. Clin Nucl Med. 2018; 43(3): e98-e100. doi: 10.1097/ RLU.0000000000001971.
- Jung SP, Lee Y, Han KM, Lee SK, Kim S, et al. Breast metastasis from rhabdomyosarcoma of the anus in an adolescent female. J Breast Cancer. 2013; 16(3): 345-8. doi: 10.4048/jbc.2013.16.3.345.
- Kebudi R, Koc BS, Gorgun O, Celik A, Kebudi A, et al. Breast Metastases in Children and Adolescents With Rhabdomyosarcoma: A Large Single-Institution Experience and Literature Review. J Pediatr Hematol Oncol. 2017; 39(1): 67-71. doi: 10.1097/ MPH.0000000000000680.
- George Zarkavelis, Dimitrios Petrakis, George Fotopoulos, Sotirios Mitrou, Nicholas Pavlidis, Bone and soft tissue sarcomas during pregnancy: A narrative.
- Haddad RN, Ghattas S, Torbey PH. Isolated Breast Relapse after Metastatic Alveolar Rhabdomyosarcoma in a Young Premenarcheal Girl: What Could Have Been Done? Case Rep Oncol. 2019; 12(3): 890-895. doi: 10.1159/000504337.
