
Open Access, Volume 10
Eight and a Half Syndrome with negative imaging
Gengxin Lu#; Zhihui Zheng#; Junyu Wu; Zhezhi Deng; Haiwei Huang*
Department of Neurology, The First Affiliated Hospital, Sun Yat-sen University, China.
Guangdong Provincial Key Laboratory of Diagnosis and Treatment of Major Neurological Diseases, China.
National Key Clinical Department and Key Discipline of Neurology, No.58 Zhongshan Road 2, Guangzhou, 510080, China.
#These authors contributed equally to this work.
Haiwei Huang
Department of Neurology, The First Affiliated Hospital, Sun Yat-sen University, China.
Guangdong Provincial Key Laboratory of Diagnosis and Treatment of Major Neurological Diseases, China.
National Key Clinical Department and Key Discipline of Neurology, Guangzhou 510080, China.
Email: huanghw@mail.sysu.edu.cn
Received : October 03, 2024,
Accepted : October 24, 2024
Published : October 31, 2024,
Archived : www.jclinmedcasereports.com
Abstract
The eight-and-a-half syndrome is a clinical condition characterized by the combination of one-and-a-half syndrome with ipsilateral peripheral facial nerve palsy. This article presents a case of a 55-year-old male patient with eight-and-a-half syndrome. Routine laboratory tests showed no significant abnormalities, cranial imaging revealed no new cerebral infarction, and cerebrospinal fluid and neural antibody tests were negative. The patient improved and was discharged following treatment with antiplatelet agents, lipid regulation, fluid replacement, circulatory support, and neurotrophic therapy. This paper analyzes the localization, characterization, etiology, and treatment process of this syndrome. Additionally, the paper emphasizes the importance of clinical diagnosis and treatment when there is a mismatch between clinical symptoms and imaging findings.
Keywords: Eight-and-a-half syndrome; Facial nerve palsy; Cranial imaging; One-and-a-half syndrome.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Huang H (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Lu G, Zheng Z, Wu J, Deng Z, Huang H. Eight and a Half Syndrome with negative imaging. Open J Clin Med Case Rep. 2024; 2298.
Introduction
One-and-a-half syndrome is caused by damage to the medial longitudinal fasciculus and paracentral reticular formation on one side, resulting in limited adduction and abduction of the affected eye and limited adduction of the contralateral eye, with nystagmus during abduction. It was first described by C. Miller Fisher in 1967 [1]. When one-and-a-half syndrome occurs with ipsilateral peripheral facial nerve palsy, it is called eight-and-a-half syndrome. This condition was first described by Eggenberger in 1998 [2] and involves the medial longitudinal fasciculus, paracentral reticular formation, and facial nerve nucleus or tract on one side. The complexity of brainstem structures means that small lesions can damage multiple cranial nerves and conduction pathways, often leading to misdiagnosis or under diagnosis. Here, we integrate the examination of a patient with eight and a half syndromes with negative imaging and a review of the literature to improve understanding of these disorders.
Case Presentation
A 55-year-old man presented to the Department of Neurology with sudden onset diplopia for 4 days and a tilted mouth for 3 days. The patient’s main presentation was sudden double vision after fatigue, accompanied by vertigo and unsteadiness. On the second morning, incomplete closure of the left eyelid accompanied by tilting of the corner of the mouth to the right side was observed. He had a history of hypertension and no family history of hereditary diseases. Neurological examination revealed incomplete left eyelid closure, limited adduction and abduction of the left eye, limited adduction of the right eye, horizontal nystagmus during abduction, loss of left frontal lines, shallow left nasolabial sulcus, and rightward deviation of the mouth (Figure 1A). Blood, urine, stool routines, homocysteine, liver/kidney function, lipid profile, glycosylated hemoglobin, and male tumor screening showed no significant abnormalities after admission. Cranial MRI indicated right frontal white matter ischemia and cerebral atherosclerosis, with no new ischemic foci (Figure 1B).
Cerebrospinal fluid routine, biochemistry, and protein tests were normal; oligoclonal bands were negative. Antibodies in cerebrospinal fluid and blood for Central Nervous System (CNS) demyelinating diseases were negative; serum autoimmune neuropathy antibodies were negative for 24 items. The patient received antiplatelet, lipid-regulating, fluid therapy, circulation improvement, and neurotrophic treatment after admission. After 2 weeks, the left eye showed limited adduction with normal abduction; the right eye had normal adduction with nystagmus in abduction, and peripheral facial palsy showed no significant improvement (Figure 1C).
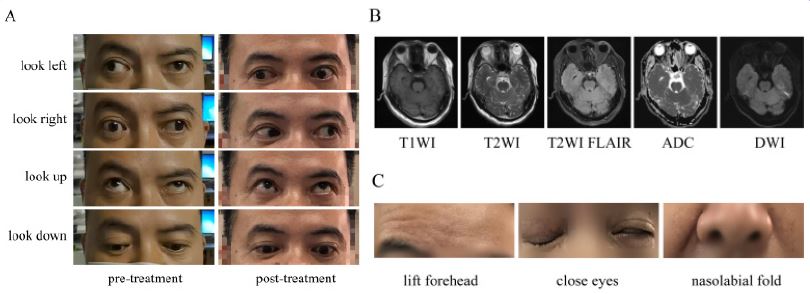
Figure 1: The patient’s clinical signs and imaging report findings. (A) Changes in the patient’s eye movements before and after treatment. Before treatment, the patient’s left eye was limited in internal adduction and abduction, and the right eye was limited in internal adduction. After treatment, the patient’s left eye was still limited in adduction, abduction was complete, and the right eye was complete. (B) The patient’s cranial MRI report indicated white matter cerebral ischemia and cerebral arteriosclerosis in the right frontal lobe, and no new ischemic foci were seen. (C) The patient has incomplete closure of the left eyelid, loss of the left frontal stripe, and shallowing of the left nasolabial groove.
Discussion/conclusion
The classic eight-and-a-half syndrome, first described by Eggenberger in 1998, presents as one-and-a-half syndrome with peripheral facial palsy on the affected side. It occurs when facial nerve fibers bypass the abducens nucleus, often affecting the facial nerve due to involvement of the parabrachial reticulo-pontine structures. Eight-and-a-half syndrome is commonly linked to cerebrovascular disease, particularly ischemic stroke. Other causes include vasculitis, capillary dilatation, cavernous hemangioma, cerebral hemorrhage, and demyelinating diseases like multiple sclerosis and neuromyelitis optica. Rare causes include tuberculosis and neoplasia [3]. Our literature review shows that eight-and-a-half syndrome has several variants. Marquart et al. [4] reported cases with ipsilateral superior colliculus or mesencephalic reticular formation lesions causing both eight-and-a-half syndrome and ipsilateral vertical gaze palsy. Felicio et al. [5-10] described a variant with bilateral horizontal gaze palsy and right-sided peripheral facial paralysis. Eight-and-a-half syndrome combined with hemiparesis or sensory deficits is called nine syndrome, indicating involvement of corticospinal and medial thalamic tracts. When a pontine lesion extends to the cerebellar peduncle and trigeminal nerve, it results in thirteen-and-a-half syndrome, involving trigeminal nerve paralysis [11-12]. When one-and-a-half syndrome combines with bilateral facial nerve paralysis, it is known as fifteen-and-a-half syndrome. The cause is thought to be a bifurcation of the paracentral middle artery supplying the pontine tegmentum bilaterally, leading to bilateral lateral nerve palsies due to vessel occlusion [13-15]. Sixteen hemi-syndromes [16-18] and twenty hemi-syndromes [19] have also been reported, presenting as eight hemi-syndromes combined with damage to the auditory nerves (1.5+7+8=16.5) and one-and-a-half syndrome plus damage to the bilateral facial nerves and the right trigeminal nerve (1.5+7+7+5=20.5), respectively.
This patient exhibited typical signs of eight-and-a-half syndrome, including left-sided one-and-a-half syndrome and left peripheral facial palsy, confirming the diagnosis. As a first-time patient, his cerebrospinal fluid tests and autoantibodies were negative, with no evidence of demyelinating disease. Trauma and poisoning were ruled out based on his medical history. This patient with eight-and-a-half syndromes had a history of hypertension, and the cranial magnetic resonance did not reveal any acute infarct foci or vascular abnormalities, which is rare. However, the possibility of cerebrovascular disease cannot be completely excluded. Due to the complexity of the brainstem structure, a very small lesion may produce a complex clinical picture. This was also confirmed by the effectiveness of antiplatelet, lipid-modulating, circulatory-improving, and neurotrophic treatment of the patient. This is a special part of this case and one that clinicians need to be aware of. At the same time, syndromes named with numbers are easier to remember, helping clinicians quickly identify and diagnose them.
Declarations
Author contributions: Gengxin Lu and Zhihui Zheng analyzed and interpreted the data and wrote the manuscript. Gengxin Lu and Zhihui Zheng and Junyu Wu revised the manuscript. Zhezhi Deng designed and conceptualized the study. Haiwei Huang interpreted the data and revised the manuscript.
Conflicts of interest: None of the authors has any conflict of interest.
Ethical approval: This study followed the tenets of the Declaration of Helsinki.
Data availability: Anonymized data will be shared by request from any qualifed investigator.
Funding source: This study was supported by grants from National Natural Science Foundation of China (82271410).
References
- Fisher CM. Some neuro-ophthalmological observations [J]. Journal of neurology, neurosurgery, and psychiatry. 1967; 30(5): 383.
- Eggenberger E. Eight-and-a-half syndrome: One-and-a-half syndrome plus cranial nerve VII palsy [J]. Journal of Neuro-ophthalmology. 1998; 18(2): 114-116.
- Cárdenas-Rodríguez MA, Castillo-Torres SA, Chávez-Luévanos B, et al. Eight-and-a-half syndrome: Video evidence and updated literature review [J]. BMJ Case Reports CP. 2020; 13(5): e234075.
- Marquart C, Strauss C, Alfieri A. Eight-and-a-half syndrome combined with an ipsilateral vertical gaze palsy: A pathophysiological explanation [J]. Clinical Neurology and Neurosurgery. 2013; 115(6): 767-769.
- Felicio AC, Bichuetti DB, Marin LF, et al. Bilateral horizontal gaze palsy with unilateral peripheral facial paralysis caused by pontine tegmentum infarction [J]. Journal of Stroke and Cerebrovascular Diseases. 2009; 18(3): 244-246.
- Rosini F, Pretegiani E, Guideri F, et al. Eight and a half syndrome with hemiparesis and hemihypesthesia: The nine syndrome? [J]. Journal of Stroke and Cerebrovascular Diseases. 2013; 22(8): e637-e638.
- Giuffrè GM, Iorio R, Masi G, et al. Nine syndrome [J]. Acta Neurologica Belgica. 2019; 119(3): 475-476.
- Cao S, Wang R, Xia M. Atypical nine syndrome in bilateral pontine infarction: A case report [J]. Medicine. 2019; 98(28).
- Jesuthasan J, Getheeswaran S, Pirasath S. An unusual presentation of hemiparesis with complex ophthalmoplegia: A nine syndrome [J]. SAGE Open Medical Case Reports. 2022; 10: 2050313X221135599.
- Cao S, Wang R, Xia M. Basilar artery dolichoectasia presenting as transverse pontine infarction and nine syndrome [J]. Neurological Sciences. 2022: 1-2.
- Allbon DS, La Hood B. Thirteen-and-a-half syndrome [J]. Journal of Neuro-Ophthalmology. 2016; 36(2): 191-192.
- Gosal JS, Khatri D, Das KK, et al. Thirteen-and-a-half Syndrome Secondary to the Brainstem Cavernoma [J]. Neurology India. 2022; 70(1): 355.
- Bae JS, Song HK. One-and-a-half syndrome with facial diplegia: The 15 1/2 syndrome? [J]. Journal of Neuro-Ophthalmology. 2005; 25(1): 52-53.
- Li M, Li X, Liu L, et al. A case report of the rare fifteen-and-a-half syndrome [J]. Medicine. 2019; 98(12).
- Zhu FY, Wang BC, Qian C, et al. Fifteen-and-a-half syndrome: A rare presentation of pontine infarction [J]. Clinical Neurology and Neurosurgery. 2018; 173: 150-153.
- Cummins G, O’hare A, Dunne R, et al. “Sixteen and a half”: A novel pontine neuro-ophthalmological syndrome [J]. Journal of neurology. 2011; 258(7): 1347.
- Choi SM, Kim TG, Chung J, et al. Sixteen-and-a-half syndrome with metastatic pons tumor: A case report [J]. Medicine. 2019; 98(47).
- Borgman CJ, Jackson AM. Sixteen‐and‐a‐half syndrome: A variant in the spectrum of Fisher’s one‐and‐a‐half syndrome [J]. Clinical and Experimental Optometry. 2019; 102(1): 94-96.
- Dube Mukesh, et al. Twenty-and-a-half syndrome: A case report [J]. Journal of medical case reports. 2019; 13(1): 35.
