
Open Access, Volume 10
Granulomatous mastitis caused by corynebacterium bovis mimicking inflammatory breast cancer: A case report
Iris Lebbe1*; Stijn Rommers1; Laura Heireman2; Kevin Wetzels3; Bernard Cambier1; Jan Decloedt4
1Department of Plastic surgery, AZ Sint-Blasius, Dendermonde, Belgium.
2Department of Laboratory and Microbiology, AZ Sint-Blasius, Dendermonde, Belgium.
3Department of Pathology, AZ Sint-Blasius, Dendermonde, Belgium.
4Department of Senology, AZ Sint-Blasius, Dendermonde, Belgium.
Iris Lebbe
Department of Plastic surgery, AZ Sint-Blasius Dendermonde, Belgium.
Email: dririslebbe@gmail.com
Received : September 24, 2024,
Accepted : October 21, 2024
Published : October 23, 2024,
Archived : www.jclinmedcasereports.com
Abstract
This case report presents the clinical course, diagnosis, and treatment of a 52-year-old woman presenting with progressive right unilateral breast pain. Initial concern for malignancy was raised; however, further investigations yielded inconclusive results. Ultimately, Corynebacterium Bovis was identified as the underlying pathogen responsible for granulomatous mastitis. This case underscores the significance of maintaining a broad range of differential diagnoses for breast pain and highlights the necessity for thorough clinical and imaging assessments to support appropriate management strategies.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Lebbe I (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Lebbe I, Rommers S, Heireman L, Wetzels K, Cambier B, Decloedt J. Granulomatous mastitis caused by corynebacterium bovis mimicking inflammatory breast cancer: A case report. Open J Clin Med Case Rep. 2024; 2297.
Introduction
Mastitis poses a clinical challenge due to its varied pathophysiological manifestations, often only leading to a diagnosis after ruling out more severe causes. Granulomatous Mastitis (GM), a relatively uncommon form of mastitis, predominantly affects middle-aged women [1]. Despite its clinical significance, the pathogenesis of GM remains incompletely understood, resulting in a lack of consensus regarding both its underlying pathophysiological mechanisms and standardized treatment approaches. Patients typically present with nonspecific symptoms, often initially managed as conventional non-lactational mastitis or malignancy. However, when standard antibiotic regimens fail, chronic inflammation ensues. This inflammation often results in fistula formation and abscess formation [2]. Diagnostic imaging often fails to definitively distinguish GM from malignancy, further complicating the diagnostic process [3]. This case study delves into the diagnostic odyssey of a patient experiencing persistent unilateral breast pain, ultimately attributed to cystic mastitis caused by a rare opportunistic pathogen.
Case Presentation
In August 2023, a 52-year-old menopausal woman Mrs. D, presented at the emergency department with complaints of extreme localized pain in her left breast. She described the pain as a unbearable continuous, dull ache, aggravated by touch and palpation. Mrs. D denied experiencing any nipple discharge, changes in skin appearance, or other associated symptoms. Her medical history showed no noteworthy past illnesses, trauma, recent lactation, or hormonal therapy. Although she had been in contact with patients with tuberculosis in the preceding months, she had not experienced any symptoms herself.
During the initial physical examination in August, extreme tenderness and hardening were observed in the lateral area of the right breast, with no palpable masses, enlarged lymph nodes in the armpit, or changes in the skin. An ultrasound revealed a diffuse inflammatory process behind the nipple, along with the presence of one cyst and one fluid collection. Both Fine Needle (FNB) and core biopsies were performed by a radiologist. No lymph node enlargement was reported (Figure 1).
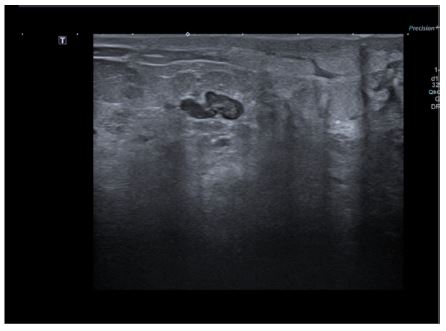
Figure 1: Ultrasound of the right breast showing the presence of a cyst and fluid collection along diffuse retroareolar inflammation. No lymph node enlargement was reported.
Intravenous penicillin antibiotics were initiated to address the abscess and observe evaluation. Despite 24 hours of observation showing no symptom improvement, the patient underwent abscess drainage in the operating room. However, only a minimal fluid collection could be drained, and pain persisted after the procedure. She was discharged the following day with oral amoxicillin clavulanic acid 875 mg/125 mg for a fourteen-day course and instructed in local wound care. Results from the biopsy specimens indicated inflammation in all biopsies, ruling out characteristics of carcinomatous mastitis. Microbiologyresults of the biopsy showed Corynebacterium bovis (low count), which was initially interpreted as contamination. Therefore, no further antimicrobial susceptibility testing was performed. Routine follow-up appointments were scheduled, where clinical exam showed more suspicious findings for malignancy. In late November, after three months of persistent symptoms, an MRI scan revealed a retroareolar BI-RADS 5 lesion with multiple nodular components (Figure 2). Subsequent biopsies were taken for pathological and microbiological testing, but again showed inflammation without evidence of malignancy. Corticosteroid therapy was initiated for non-infectious granulomatous mastitis; however, after three weeks with no improvement along with slight exacerbation of skin induration and retraction, alternative treatment approaches were considered.
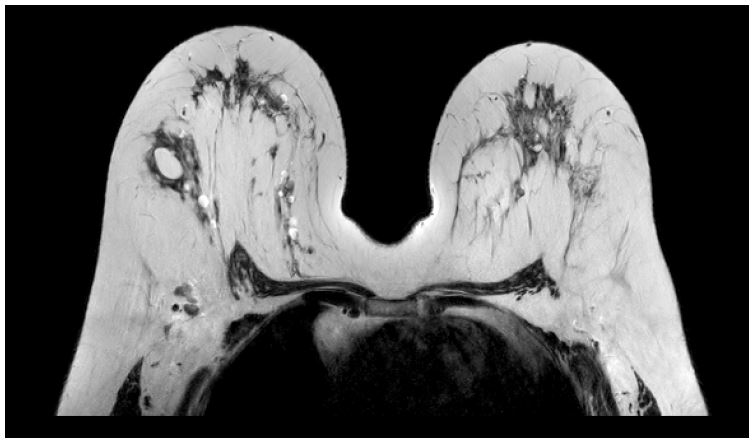
Figure 2: MRI-scan of the breast showing a retroareolar BI-RADS 5 lesion with multiple nodular components.

Figure 3: Presentation patient’s breast in November with nipple retraction and induration of the breast.
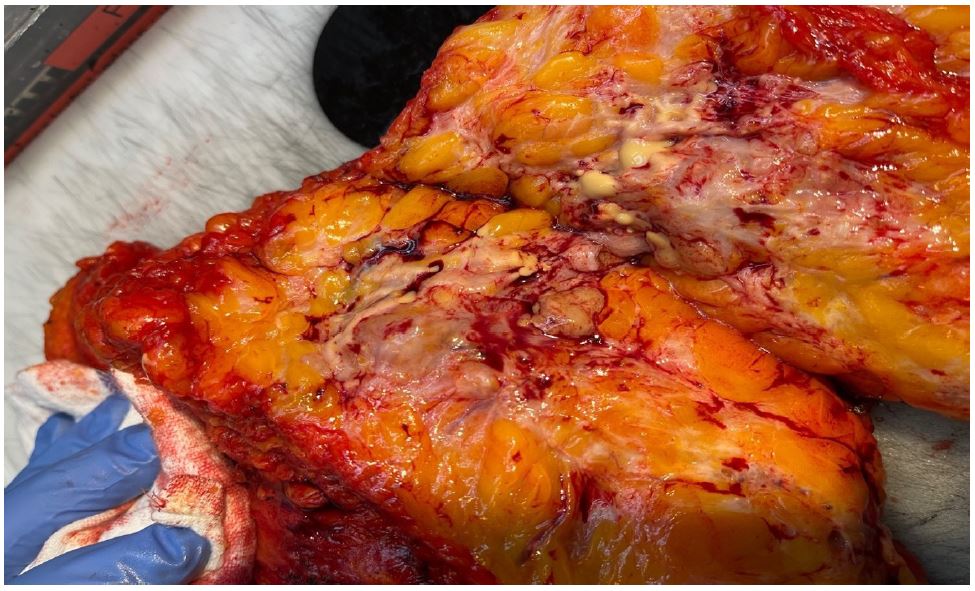
Figure 4: Peroperative image after cutting the lesion in half with visable cystic abcedation.
Due to the persistent symptoms of extreme discomfort and lack of improvement with prior treatment, the patient’s case was discussed during the oncological multidisciplinary team discussion. Vacuum-assisted core needle biopies were performed for microbiological examination to exclude tuberculosis. The patient underwent a PET scan to rule out malignancy, given the expected disparity in metabolic activity between tumor and abscess/inflammation.
The targeted biopsies did not reveal tuberculosis but once again detected Corynebacterium bovis in microbiological culture (few colonies). Antibiotic sensitivity testing demonstrated intermediate resistance to benzylpenicillin and ciprofloxacin, while exhibiting susceptibility to clindamycin and doxycycline. Consequently, the patient commenced oral doxycycline 2x100 mg therapy for a duration of three weeks. A follow-up PET scan conducted three weeks later indicated three hypercaptating lesions, raising significant suspicion for malignancy, along with reactive axillary lymph nodes secondary to inflammation.
This discordance between bacterial presence and hypercaptating lesions in diagnostic findings ultimately prompted a mutual decision between the medical team and the patient to proceed with mastectomy in January 2024. Peroperative images were taken of the lesions and were suspect for an necrotising/cystic process (Figure 4). Subsequent histopathological analysis confirmed the diagnosis of cystic mastitis without evidence of malignancy. Remnants of Corynebacterium were identified within multiple of the cysts (Figure 5).
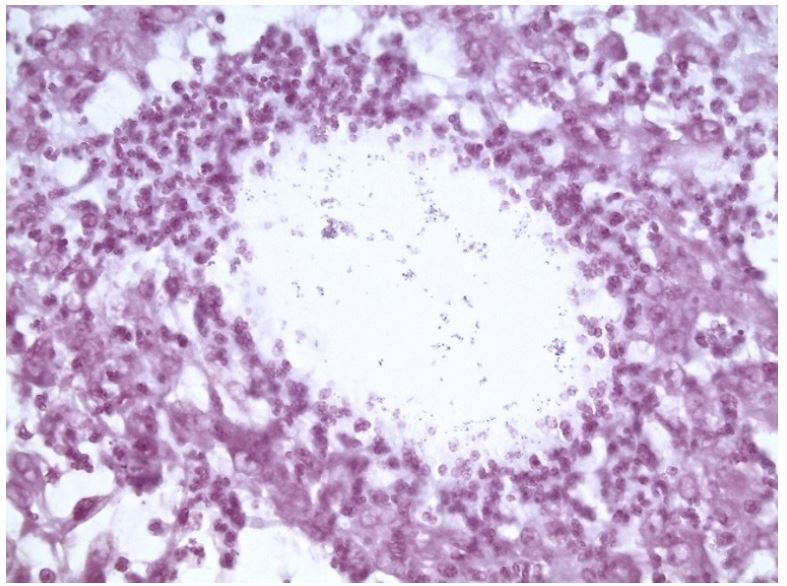
Figure 5: Micro-abscesses and inflammatory foci with tissue necrosis, multinucleated giant cells due to phagocytosis and plasma cells. Gram staining showed remnants of bacteria (consistent with Corynebacteria) in multiple cysts.
The patient’s postoperative recovery was unremarkable with significant improvement of symptoms. As a result, there has been an improvement in her overall quality of life. She was offered a referral to the plastic surgery department for reconstruction of her breast in the future.
Discussion
This case highlights the significance of employing a systematic approach in the evaluation of breast pain, encompassing both common and rare etiologies. While malignancy typically remains a primary consideration and may initially manifest as mastitis, the differential diagnosis should also encompass less common pathogens such as tuberculosis or other infectious agents. This is particularly important in the absence of overtly alarming clinical features. Corticosteroids were initiated to manage Granulomatous Mastitis (GM), based on the pathophysiological rationale of suppressing granuloma formation by inhibiting the production of inflammatory cytokines such as TNF-α and IFN-γ. This therapeutic approach is analogous to its application in other non-infectious granulomatous disorders like sarcoidosis. However, this therapeutic rationale suggests that GM may not be solely attributable to infectious origins.
The ethical dilemma at hand involves balancing the risks and benefits of prolonged antibiotic treatment versus surgical intervention (mastectomy) based on suspicion of malignancy that ultimately proves to be non-malignant. On one hand, delaying surgical intervention in favor of antibiotic therapy poses the risk of allowing potential malignancy to progress if present, potentially impacting prognosis and treatment outcomes. On the other hand, opting for mastectomy based on suspicion alone carries the risk of subjecting the patient to an invasive procedure with inherent physical and psychological consequences, especially if malignancy is ultimately ruled out postoperatively. This dilemma underscores the importance of judicious clinical decision-making, weighing the available diagnostic evidence, patient preferences, and potential risks associated with each course of action to ensure the best possible outcome for the patient. In our case, extreme discomfort and pain were leading us in the direction of a mastectomy.
Contrary to previous beliefs, a significant observation by Taylor et al. in 2003 revealed a frequent presence of Gram-positive bacilli within the granulomas of women diagnosed with Granulomatous Mastitis (GM). Notably, Corynebacterium Kroppenstedii was isolated in 44% of cases within the observed case series. This finding prompted the assertion that despite being commonly regarded as contaminants, corynebacteria are likely genuine pathogens when isolated from breast tissue [4-6].
Corynebacterium bovis (CB), a gram-positive pathogen recognized for causing mastitis in cattle, was previously presumed to rarely instigate infections in humans [7]. However, subsequent studies have increasingly implicated CB in human infections, such as brain infections, autologous fat grafting infections, eye infections and granulomatous mastitis [8-10]. Nonetheless, achieving consistent isolation remains challenging due to the prolonged incubation periods or specialized growth media required for certain Corynebacterium spp.
When contemplating antibiotic therapy for Corynebacterium (CB) infections, penicillin and other beta-lactam antibiotics are frequently efficacious. However, in our case, CB exhibited susceptibility to benzylpenicillin (susceptibile, increased exposure) and doxycycline (susceptible). Despite antibiotic treatment, the patient’s symptoms persisted. This may be attributed, as noted in other studies, to the necessity for prolonged administration of lipophilic antibiotics to achieve optimal outcomes and enhanced tissue penetration [11,12].
Corynebacterium spp. typically inhabit lipid-filled vacuoles within the granuloma rather than the surrounding inflamed tissue [2]. In our case, an extended course of antibiotics was not recommended due to the suspicion raised by the PET-scan, which required prompt initiation of malignancy treatment. Consequently, in collaboration with the patient, the breast surgeons elected for mastectomy given her compromised quality of life due to persistent right breast pain and suspected underlying malignancy. Tissue expanders were deferred during mastectomy to mitigate the risk of implant-related infection. Subsequent reconstruction of the breast will be planned in a staged manner, and not immediate as described by Hladik et al. (2011) to avoid infection of the operated area [13].
If there is suspicion of a microbiological cause of GM or if it cannot be definitively ruled out, Williams et al. (2021) outlined a methodology for assessing and managing infectious agents, particularly targeting Corynebacterium spp. This approach entails: 1) seeking species-level identification of Corynebacterium spp. either through culture isolation or Polymerase Chain Reaction (PCR), 2) employing lipophilic antibiotics or higher doses of non-lipophilic antibiotics to enhance tissue penetration, 3) advocating for prolonged medical treatment due to the inhibitory effect of granuloma structure and function on antibiotic efficacy, 4) considering adjunctive glucocorticoid therapy for cases resistant to conventional treatment, and 5) recommending surgical intervention in the presence of drainable lesions or for symptomatic relief as needed [2,14].
Additional studies are required to comprehensively assess the involvement of corynebacteria in Granulomatous Mastitis (GM).
Although Corynebacteria are frequent skin colonizers, their presence in breast tissue should be interpreted as truly pathogenic in the diagnostic work-up of granulomatous mastitis. To our knowledge, this is the first case of granulomatous mastitis caused by the Corynebacteria species C. bovis. In the presented case, a treatment course of three weeks with a lipophilic antibiotic was not sufficient to eliminate bacteria within the lipid-filled spaces. It is uncertain whether a longer antibiotic treatment duration could have prevented the mastectomy in this patient. Further research is necessary to determine how long the antibiotic (and corticosteroid) treatment should last before a potential effect on inflammation can be expected.
Declaration of artificial intelligence technologies in the writing process: During the preparation of this work, the authors used ChatGPT (OpenAI, San Francisco, California, USA, https://chat.openai.com/).
References
- Kessler E, Wolloch Y. Granulomatous mastitis: A lesion clinically simulating carcinoma. Am J Clin Pathol. 1972; 58(6): 642-6.
- Williams MS, McClintock AH, Bourassa L, Laya MB. Treatment of Granulomatous Mastitis: Is There a Role for Antibiotics? Eur J Breast Health. 2021; 17(3): 239-46.
- Heer R, Shrimankar J, Griffith CDM. Granulomatous mastitis can mimic breast cancer on clinical, radiological or cytological examination: a cautionary tale. Breast. 2003; 12(4): 283-6.
- Taylor GB, Paviour SD, Musaad S, Jones WO, Holland DJ. A clinicopathological review of 34 cases of inflammatory breast disease showing an association between corynebacteria infection and granulomatous mastitis. Pathology. 2003; 35(2): 109-19.
- Paviour S, Musaad S, Roberts S, Taylor G, Taylor S, et al. Corynebacterium species isolated from patients with mastitis. Clin Infect Dis. 2002; 35(11): 1434-40.
- Johnson MG, Leal S, Plongla R, Leone PA, Gilligan PH. Closing the Brief Case: Recurrent Granulomatous Mastitis Due to Corynebacterium kroppenstedtii. J Clin Microbiol. 2016; 54(8): 2212.
- Vale JA, Scott GW. Corynebacterium bovis as a cause of human disease. Lancet. 1977; 2(8040): 682-4.
- Gabay S, Tene Y, Ben-Ami R, Shapira Y. Corynebacterium bovis surgical site infection and brain abscess: The first case report and literature review. IDCases. 2023; 33: e01782.
- You X, Yao Y, Gao J, Liao Y. Corynebacterium bovis infection after autologous fat grafting in breast augmentation: a case report. Front Cell Infect Microbiol. 2023; 13: 1265872.
- Chow SK, Bui U, Clarridge JE. Corynebacterium bovis Eye Infections, Washington, USA, 2013. Emerg Infect Dis. 2015; 21(9): 1687-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4550150/
- Dobinson HC, Anderson TP, Chambers ST, Doogue MP, Seaward L, et al. Antimicrobial Treatment Options for Granulomatous Mastitis Caused by Corynebacterium Species. J Clin Microbiol. 2015; 53(9): 2895-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4540898/
- Néel A, Hello M, Cottereau A, Graveleau J, De Faucal P, et al. Long-term outcome in idiopathic granulomatous mastitis: a western multicentre study. QJM. 2013; 106(5): 433-41.
- Hladik M, Schoeller T, Ensat F, Wechselberger G. Idiopathic granulomatous mastitis: Successful treatment by mastectomy and immediate breast reconstruction. J Plast Reconstr Aesthet Surg. 2011; 64(12): 1604-7.
- Wilson BF, Chin JC. Idiopathic Granulomatous Lobular Mastitis: A Mimicker of Inflammatory Breast Cancer. Fed Pract. 2023; 40(9): 325-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10984687/
