
Open Access, Volume 10
Esterified hyaluronic acid regenerative dermal matrix effectively augments secondary intent healing of mohs micrographic surgery defects with exposed cartilage
Kevin M. Crawford, MD1*; Mallori Hathaway, PA-C2; Caroline Crawford2
1Department of Dermatology, Marian University College of Osteopathic Medicine, Indianapolis, USA.
Department of Dermatology, Indiana University School of Medicine, Indianapolis, Indiana, USA.
2Forefront Dermatology, 303 South Walnut Street, Seymour, IN 47274, USA.
Kevin M. Crawford, MD
Forefront Dermatology, 880 Baywood Ct, Columbus, IN 47201, USA.
Email: kcrawford@forefrontderm.com
Received : September 12, 2024,
Accepted : October 10, 2024
Published : October 15, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Mohs Micrographic Surgery (MMS) creates a defect following the removal of cutaneous malignancies. Due to lack of adjacent tissue reservoirs and laxity, primary closure or local skin flaps are not always viable options for closure of these defects. Skin graft necrosis and failure is high in these situations, due to the avascular nature of cartilage. When secondary intention is utilized these wounds with exposed cartilage may take longer to heal and be more painful. We wanted to determine if an esterified Hyaluronic Acid Matrix (eHAM) can augment secondary intent healing of MMS defects with exposed cartilage. We evaluated 20 patients with cutaneous malignancies and exposed cartilage following MMS including: 16 cases of the nose and 4 cases of the ear. Patients received weekly eHAM applications for a total of 2-14 applications. The initial defect area ranged from 0.70 to 13.50 cm2 and following 2-13 weeks of eHAM treatment (average 7±3 weeks) the final defect area ranged from 0.01 to 3.10 cm2. The average area of defect closure was 77± 23% at a rate of closure of 0.03 to 3.71 cm2/week. Patients required minimal treatment for pain and none of the patients required delayed skin grafting. There we no infections or complications during the eHAM application and secondary intent healing process. According to clinician observation, the final cosmetic appearance was excellent. Following MMS, eHAM is an effective treatment for secondary healing of defects with exposed cartilage. Patients experienced minimal pain or anxiety during the eHAM treatment period.Mohs Micrographic Surgery (MMS) creates a defect following the removal of cutaneous malignancies. Due to lack of adjacent tissue reservoirs and laxity, primary closure or local skin flaps are not always viable options for closure of these defects. Skin graft necrosis and failure is high in these situations, due to the avascular nature of cartilage. When secondary intention is utilized these wounds with exposed cartilage may take longer to heal and be more painful. We wanted to determine if an esterified Hyaluronic Acid Matrix (eHAM) can augment secondary intent healing of MMS defects with exposed cartilage. We evaluated 20 patients with cutaneous malignancies and exposed cartilage following MMS including: 16 cases of the nose and 4 cases of the ear. Patients received weekly eHAM applications for a total of 2-14 applications. The initial defect area ranged from 0.70 to 13.50 cm2 and following 2-13 weeks of eHAM treatment (average 7±3 weeks) the final defect area ranged from 0.01 to 3.10 cm2. The average area of defect closure was 77± 23% at a rate of closure of 0.03 to 3.71 cm2/week. Patients required minimal treatment for pain and none of the patients required delayed skin grafting. There we no infections or complications during the eHAM application and secondary intent healing process. According to clinician observation, the final cosmetic appearance was excellent. Following MMS, eHAM is an effective treatment for secondary healing of defects with exposed cartilage. Patients experienced minimal pain or anxiety during the eHAM treatment period.
Keywords: Mohs Micrographic Surgery (MMS); Cutaneous malignancies; Esterified hyaluronic acid.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Crawford KM (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Crawford KM, Hathaway M. Esterified hyaluronic acid regenerative dermal matrix effectively augments secondary intent healing of mohs micrographic surgery defects with exposed cartilage. Open J Clin Med Case Rep. 2024; 2294.
Introduction
Mohs Micrographic Surgery (MMS) is the standard of care for the treatment of recurrent cutaneous malignancies [1]. MMS is the treatment of choice for most skin cancers located on the head and neck [1]. Other treatment options include conservative excision, electrodessication and curettage, radiation, photodynamic therapy, topical chemotherapy, sonic-hedgehog inhibitors (systemic chemotherapy), or immunotherapy [2]. The choice of repair methods often depends on the location and extent of the wound defect created following surgery and would include secondary intention, primary (linear) repair, skin grafting, and skin flaps [3]. Other factors may impact the final defect size following MMS including tumor type, aggressive tumor pathology, and anatomic location [4]. In a study of 101 cases with auricular cutaneous malignancies, wound defects with cartilage loss were treated with a skin graft. More complex MMS involve cartilage loss, antibiotic use, and discomfort to the patient [3]. Auricular reconstruction may require cartilaginous replacement for wound defects with cartilaginous loss [5]. Nasal defects involving the loss of cartilage following MMS may require autogenous grafting of cartilaginous material from septal or auricular reservoirs. Alternatively, costal cartilage can be used in a free cartilage graft or composite cartilage graft [6]. Excessive cartilage loss following MMS treated with cartilage grafts and skin flaps may require up to 3 months to heal [7].
Careful analysis of available tissue reservoirs, adjacent anatomic structures, and cosmesis impact the decision of how to appropriately reconstruct each MMS defect [8]. Choosing the appropriate MMS defect closure can be challenging and must be individualized for each patient’s unique setting. In a ten-year MMS study, a total of 975 facial and extra-facial defect repairs were evaluated that included; 40.7% flaps, 39.2% primary repair, and 10% skin grafts [9]. In a large MMS study of 3937 patients with basal cell or squamous cell carcinomas, 1540 patients received MMS in the hospital and 2397 patients underwent MMS in an out-patient setting [10]. The resulting wound defect following MMS averaged 2.4x1.8 cm (area of 4.3 cm2). Primary repair, skin flaps, secondary intent, and skin grafts were utilized in 69%, 14%, 11%, and 6% of defects, respectively. Wound closures were similar in either the hospital or the out-patient setting [10].
In another clinical study, 397 patients underwent MMS followed by Full-Thickness Skin Graft (FTSG) reconstruction [11]. Thirty-six of the 397 (9.1%) patients required treatment for FTSG complications. Early complications included infections, hematoma, and seroma formation. Long-term complications were mainly cosmetic because of FTSG color and texture mismatch [11]. The use of advancement flaps following nasal Mohs surgery has been shown to provide good cosmetic outcomes resulting from matched skin color, texture, thickness, and reduced scarring [12]. However, there is increased risk of pain, infection, bleeding, flap necrosis and other complications when compared to primary closure or secondary intent healing [12].
Significant postoperative pain related to MMS has been reported in 33-50% of patients on the day of the Mohs surgery [13]. Pain was more common in patients who spent more time in the office, had three or more layers excised, or when a skin flap or skin graft was utilized for reconstruction. Anatomic sites where complaint of significant pain was most common following MMS were the nose or periorbital area [13]. In a survey of 471 dermatology patients, patients with no prior Mohs surgery had significantly higher levels of anxiety compared to patients with prior Mohs surgery [14]. Approximately three fourths (72.5%) of Mohs patients found a narrative video describing the MMS procedure including a testimonial from a previous patient to be comforting [15]. When patients were asked what they were most concerned about the responses included: scarring, danger of skin cancer, pain, the MMS procedure itself, and recovery following the MMS procedure [15].
Perioperative anxiety to MMS contributes to poor outcomes and patient dissatisfaction [16]. Patient anxiety can be attributed to general concerns of skin cancer, pain, complications, and overall cosmetic outcome. In a study of 88 patients undergoing MMS for removal of non-melanoma skin cancer, patients received education using a 3D-printed MMS model prior to the actual MMS [16]. When compared to standardized education methods, the 3D-printed MMS model reduced perioperative anxiety. The reduction of anxiety was attributed to be a result of better patient education [16]. In a study of seven patients with removal of nasal basal cell carcinoma by MMS the surgical defect area ranged from 2.7 to 20 cm2. The wound defects were then treated with human cadaveric allograph as an alternative to granulation. The average healing times for wounds with and without exposed cartilage were 6 weeks and 5 weeks, respectively [17].
Hyaluronic Acid (HA) has been shown to aid in wound healing by increasing fibroblast infiltration, collagen deposition, and capillary formation [18]. Esterification of the Hyaluronic Acid Matrix (eHAM) can prolong the half-life and can provide the necessary ECM for extended wound healing [19]. During the early stage of the wound healing process, eHAM provides a durable Extracellular Matrix (ECM) which supports keratinocyte migration and re-epithelization [20]. However, the de-esterification and degradation of the eHAM is just as critical for wound healing. The slowly emerging HA moieties in the biodegrading esterified hyaluronic acid matrix scaffold elicit the neodermal healing response. The eHAM forms a scaffold for the orderly colonization of fibroblasts, endothelial cells, ECM formation, and “steady state” wound healing process [21,22]. For the treatment of deep wounds and burns, eHAM can provide a suitable scaffold for endothelial cell migration and generation of engineered vascular grafts [22].
The eHAM acts as a regenerative dermal substitute using a silicone membrane to maintain moisture at the wound site which is subsequently removed following incorporation of the eHAM matrix. The silicone membrane additionally provides barrier function while avoiding vapor loss resulting in a reduced incidence of bacterial infection. The application of eHAM allows close monitoring of the wound repair process and reconstruction of the dermal tissue [23]. The use of biologically tissue engineered acellular dermal matrices have been used in the wound management of upper and lower extremities where there is exposed bone, tendon, and muscle [24]. In a case series and literature review eHAM was shown to be an effective treatment for difficult to heal diabetic ulcers with exposed bone and tendon following surgical debridement [19].
Based on the knowledge that eHAM can effectively heal exposed bone and tendon wounds we undertook a study to treat 20 patients with exposed cartilage defects following MMS. Here we report on the utility of eHAM being used in cases where there is exposed cartilage. Exposed cartilage predisposes patient to pain, desiccation of the cartilage, increased risk of infection, poor cosmetic outcomes, and impaired function of the involved anatomic structure. Exposed cartilage wounds require more time for healing than wounds without exposed cartilage wounds. We sought to avoid the use of skin flaps, skin grafting, cartilage grafts, and cadaveric skin and relied on eHAM to provide the necessary defect healing. We report on the findings of 20 patients in this MMS study using eHAM.
Material and Methods
Study design
Twenty patients aged 45-91 years (median 71 years) participated in a Mohs surgery case study conducted in an outpatient setting (Table 1). Patients were seen by appointment to replace the eHAM weekly in an outpatient setting.
Study treatments
All patients received Mohs surgery as treatment for non-melanoma skin cancer. Sixteen cases involved the nose, while four cases involved the ear. Tumor morphology included 14 basal cell carcinomas and 6 squamous cell carcinomas. All 20 cases in this study resulted in a final defect with exposed cartilage. Wound locations and tumor histology are shown in (Table 1). All patients received a prescription for Tramadol to take as needed for post-operative pain. Following Mohs surgery, the patients received one application of eHAM (Hyalomatrix®, Medline Industries, LP. Northfield, IL). The eHAM was applied to the wound and secured with interrupted nylon or polypropylene suture. A bolster bandage was applied directly over the eHAM to protect the wound and assist in hemostasis.
One-week post-surgery, the patients were seen in follow-up and the bolster bandage was removed. At this time any residual eHAM was removed from the surgical site, the wound was cleansed, and excess granulation or necrotic tissue was debrided as appropriate. A new eHAM was then placed on the wound. Patients received a total of 2-14 applications of eHAM over the ensuing 4-15 weeks. Visual defects were measured and photographed weekly when the patient was seen during wound care appointments. During the weekly wound care appointments, additional eHAM applications were performed until the wound was fully healed. Photographs of the surgical site were taken prior to Mohs surgery, following Mohs surgery (initial defect), and prior to each eHAM application until the wound had closed (final defect). Final images post-operatively were taken when possible.
Study assessments
The initial size of the surgical defect was measured post-operatively following the Mohs surgery and during each patient’s outpatient visit. The final defect measurements were taken approximately one week after the final eHAM application. The percentage of defect closure was determined based on the last day of the defect measurement. The percentage of defect closure was determined by dividing the area of the initial defect by the area of the final defect x100 (Table 2). The rate of defect closure was determined per week by dividing the difference between the initial and final defect at the end of eHAM treatment by the number of weeks of eHAM treatment, Images of the defect were taken during each patient visit following eHAM applications. No eHAM was applied during the patient’s final evaluation. The final data point is defined as the end of eHAM treatment. The eHAM treatment was used until the defect was on a good trajectory to heal. The final decision to stop the eHAM treatment was made at this point.
Results
Study population
Patient demographics, comorbidities, cancer type, and anatomic location are provided in Table 1 for the 20 cases on this study. The age range was 45-91 years old with 13 male and 7 female cases. All patients were Caucasian. The most common comorbidities included: six cases with HTN and three cases with HTG. Twelve patients had no reported comorbidities. The types of carcinomas included 14 cases of basal cell cancer and six cases of squamous cell cancer. The basal cell carcinomas included nodular, infiltrative, and superficial histology. The squamous cell carcinomas included well differentiated, in-situ, and invasive histology. Sixteen cases were located on the nose (nasal), while 4 cases involved the ear.
Table 1: Patient demographics, comorbidities, and wound location.
| Case | Sex, Age, Ethnicity | Comorbidities | Type of Carcinoma | Anatomic Location |
|---|---|---|---|---|
| 1 | Male, 65 y/o, Caucasian | Psoriasis | Squamous cell in situ | Left antihelix |
| 2 | Male, 76 y/o, Caucasian | HTN, HTG | Moderately differentiated squamous cell | Nasal dorsum |
| 3 | Female, 69 y/o, Caucasian | None | Ulcerated Basal cell nodular and infiltrative types | Nasal supratip |
| 4 | Female, 75 y/o, Caucasian | HTN, HTG, Arthritis | Basal cell, nodular type | L nasal sidewall |
| 5 | Male, 57 y/o, Caucasian | HTN | Basal cell, nodular type | Right nasal ala |
| 6 | Male, 71 y/o, Caucasian | None | Micro-invasive squamous cell | Right nasal sidewall |
| 7 | Male, 91 y/o, Caucasian | HTN, HTG, GERD | Basal cell, nodular type | Right crus |
| 8 | Male, 77 y/o, Caucasian | None | Basal cell, nodular type | Right posterior auricle |
| 9 | Female, 79 y/o, Caucasian | HTN | Basal cell, nodular type | Nasal dorsum |
| 10 | Female, 77 y/o, Caucasian | None | Basal cell, nodulo-infiltrative type | Nasal supratip |
| 11 | Male, 66 y/o, Caucasian | None | Basal cell, nodular type, ulcerated | Nasal root |
| 12 | Female, 71 y/o, Caucasian | None | Basal cell, superficial, nodular and infiltrative type | Left nasal tip |
| 13 | Male, 71 y/o, Caucasian | None | Squamous cell in situ | Left antihelix |
| 14 | Male, 54 y/o, Caucasian | HTN | Basal cell, nodulo-infiltrative type | Left nasal sidewall |
| 15 | Male, 62 y/o, Caucasian | None | Basal cell, nodular and infiltrative types | Nasal supratip |
| 16 | Male, 57 y/o, Caucasian | None | Squamous cell, well differentiated | Left nasal supratip |
| 17 | Female, 45 y/o, Caucasian | None | Basal cell, nodular type | Right nasal ala |
| 18 | Female, 84 y/o, Caucasian | HTN, Diabetes | Basal cell, nodulo-infiltrative type | Right nasal sidewall |
| 19 | Male, 76 y/o, Caucasian | None | Squamous cell, nodular type | Left nasal tip |
| 20 | Male, 69 y/o, Caucasian | None | Basal cell, superficial and nodular type | Right nasal supratip |
Abbreviations: HTN: Hypertension; HTG: Hypertriglyceridemia; GERD: Gastroesophageal Reflux Disease.
All 20 patient cases in this study underwent Mohs surgery that resulted in cartilage exposure at the wound defect. The initial defect area, final defect area at the end of eHAM treatment, percent of defect closure, rate of defect closure, number of weeks of eHAM treatment, number of eHAM applications, and total weeks of observation are summarized in (Table 2). The initial wound defect area ranged from 0.70 to 13.50 cm2 while the final defect area ranged from 0.01 to 3.10 cm2. The average reduction in area of the wound during treatment with eHAM was 77±23%. The average rate of defect closure per week was 0.65±1.00 cm2/week. Wounds required an average of 8±3 weeks for complete healing. During treatment, patients received 2-14 eHAM applications. With the exception of Case 12, all patients received a prescription for Tramadol to use as needed for pain. Case 14 also received Hydrocodone - Acetaminophen at 5-325 mg for pain management. None of the patients in the study required skin grafts for wound closure.
Table 2: Wound defect area prior to and following treatment with Eham.
| Case Number | Initial defect area(cm2) | Final defectarea at the end of eHAM treatment (cm2) | %Defectclosure | Rate of defectclosure per week(cm2/week) | Weeksof eHAMtreatment | Number of eHAMapplications | Totalweeks ofobservation |
|---|---|---|---|---|---|---|---|
| 1 | 1.10 | 0.20 | 82% | 0.23 | 4 | 3 | 4 |
| 2 | 3.60 | 0.40 | 89% | 0.40 | 8 | 7 | 11 |
| 3 | 2.10 | 0.12 | 94% | 0.40 | 5 | 5 | 5 |
| 4 | 1.40 | 0.01 | 99% | 0.20 | 7 | 5 | 7 |
| 5 | 2.40 | 0.80 | 67% | 0.40 | 4 | 5 | 6 |
| 6 | 6.20 | 0.80 | 87% | 0.68 | 8 | 7 | 9 |
| 7 | 4.20 | 3.10 | 26% | 0.12 | 7 | 8 | 9 |
| 8 | 3.20 | 0.40 | 88% | 0.29 | 7 | 6 | 8 |
| 9 | 1.50 | 0.56 | 63% | 3.27 | 4 | 4 | 5 |
| 10 | 2.70 | 0.64 | 76% | 0.03 | 12 | 12 | 13 |
| 11 | 13.50 | 0.42 | 97% | 0.65 | 7 | 8 | 9 |
| 12 | 0.70 | 0.30 | 57% | 3.71 | 3 | 4 | 5 |
| 13 | 4.60 | 0.08 | 98% | 0.11 | 10 | 10 | 11 |
| 14 | 11.20 | 0.06 | 99% | 0.03 | 9 | 9 | 10 |
| 15 | 1.10 | 0.81 | 26% | 0.23 | 4 | 4 | 5 |
| 16 | 1.80 | 0.90 | 50% | 0.62 | 2 | 2 | 5 |
| 17 | 1.80 | 0.56 | 69% | 0.47 | 6 | 6 | 7 |
| 18 | 4.90 | 0.16 | 97% | 0.59 | 8 | 8 | 9 |
| 19 | 3.80 | 0.50 | 87% | 0.25 | 13 | 14 | 15 |
| 20 | 2.72 | 0.48 | 82% | 0.25 | 9 | 10 | 11 |
| Ave ± Std | 3.73±3.30 | 0.57±0.66 | 77±23% | 0.65±1.00 | 7±3 | 7±3 | 8±3 |
| Range | 0.70 to 13.50 | 0.01 to 3.10 | 0.26 to 0.99 | 0.03 to 3.71 | 2 to 13 | 2 to 14 | 4 to 15 |
Ave: Average; SD: Standard Deviation
Case Study Images
Case 1 (Figure 1) is a 65 y/o male with psoriasis who underwent Mohs surgery for squamous cell carcinoma, in situ, of the antihelix of the left ear. Images shown are A) pre-operative, B) defect following Mohs surgery, C) following eHAM application at day 10, D) at day 18 and E) final image at day 25. The final eHAM application was on day 18 (week 3). The initial defect area was 1.1 cm2 that decreased to 0.2 cm2 at day 25 (week 4) following three applications of eHAM.

Figure 1: Case 1 Mohs surgery of antihelix of the left ear prior to Mohs surgery. A) pre-operative, B) defect following Mohs surgery, /C) day 10 following eHAM application, D) day 18 and E) day 25.
Case 2 (Figure 2) is a 76 y/o male with hypertension and hypertriglyceridemia who underwent Mohs surgery for moderately differentiated squamous cell carcinoma of the nasal dorsum. Images demonstrate A) pre-operative, B) defect following Mohs surgery, C) following eHAM application at day 9, D) at day 21, E) at day 58 and F) final image at day 79 (week 11). The final eHAM application was on day 58 (week 8). The initial defect area was 3.6 cm2 which decreased to 0.4 cm2 at day 58 (week 8) following seven applications of eHAM. The final image at day 79 (week 11) is shown in (Figure 2F).

Figure 2: Case 2 shows the nasal dorsum of the nose prior to Mohs surgery. A) pre-operative, B) defect following Mohs surgery, C) day 9 following eHAM application, D) at day 21, E) at day 58 and, F) day 79.
Case 3 (Figure 3) is a 69 y/o female with no comorbidities who underwent Mohs surgery for a nodular and infiltrative basal cell carcinoma involving the nasal supratip. Images include A) pre-operative, B) defect following Mohs surgery, C) following eHAM application at day 7, D) at day 14, E) and at day 21. The final eHAM application was on day 21 (week 3). No eHAM was applied on day 28 (week 4). The initial defect area was 2.1 cm2 which decreased to 0.12 cm2 at day 35 (week 5) requiring five applications of eHAM. The final image was taken at day 45 (week 5) shown in (Figure 3E).

Figure 3: Case 3 shows the nasal supratip of the nose prior to Mohs surgery. A) pre-operative, B) defect following Mohs surgery, C) day 14 following eHAM application, D) at day 35, E) and at day 45.
Case 4 (Figure 4) is a 75 y/o female with arthritis, hypertension, and hypertriglyceridemia who underwent Mohs surgery for a nodular basal cell carcinoma of the left nasal sidewall. Images include A) pre-operative, B) defect following Mohs surgery, C) following eHAM application at day 9, D) at day 17, E) at day 24, F) at day 29 G) at day 39 and H) final image at day 46. The final eHAM application was on day 29 (week 4). The patient did not receive an eHAM application on day 39 (week 5). The initial defect area was 1.4 cm2 that decreased to 0.01 cm2 at day 46 (week 7) following five applications of eHAM.
Case 5 (Figure 5) is a 57 y/o male with hypertension who underwent Mohs surgery for a nodular basal cell carcinoma of the right nasal sidewall. Images include A) pre-operative, B) defect following Mohs surgery, C) following eHAM application at day 8, D) at day 15, E) at day 22 and F) at day 28. The final eHAM application was on day 28 (week 4). The initial defect area was 2.4 cm2 that decreased to 0.8 cm2 at day 28 (week 4) following five applications of eHAM.
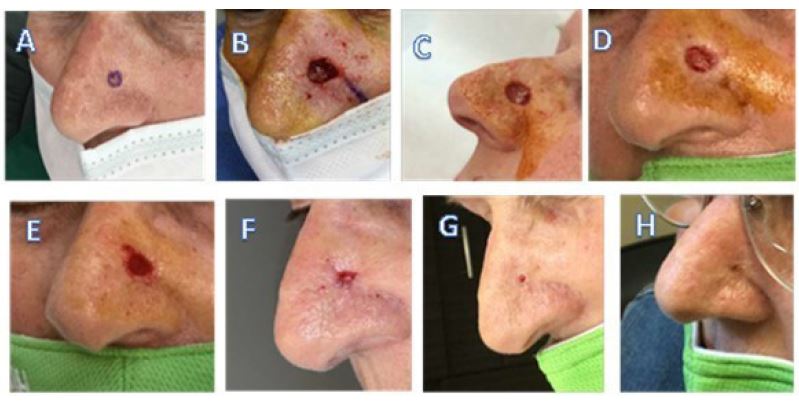
Figure 4: Case 4 shows the left nasal sidewall of the nose prior to Mohs surgery. A) pre-operative, B) defect following Mohs surgery, C) day 9 following eHAM application, D) at day 17, E) at day 24, F) at day 29, G) at day 39, and H) day 46.

Figure 5: Case 5 shows the right nasal sidewall of the nose prior to Mohs surgery. A) pre-operative, B) defect following Mohs surgery, C) day 8 following eHAM application, D) at day 15, E) at day 22, F) at day 28.
Case 6 (Figure 6) is a 71 y/o male with no comorbidities who underwent Mohs surgery for a micro-invasive, squamous cell carcinoma of the right nasal sidewall. Include: A) pre-operative, B) defect following Mohs surgery, C) following eHAM application at day 8, D) at day 17, E) at day 33 F) at day 40, G) at day 47, H) at day 54, and I) final image at day 60. The final eHAM application was on day 54 (week 8). The initial defect area was 6.2 cm2 that decreased to 0.8 cm2 at day 54 (week 8) following seven applications of eHAM. Complete healing was observed at day 60 (week 9) as shown in (Figure 6I).
Case 7 (Figure 7) is a 91 y/o male with hypertension, hypertriglyceridemia, and GERD who underwent Mohs surgery for a nodular basal cell carcinoma of the crus of the right ear. Images include A) pre-operative, B) following eHAM application at day 16, C) at day 26, D) at day 41 and E) at day 57. The final eHAM application was on day 57 (week 8). The initial defect area was 4.2 cm2 which decreased to 3.1 cm2 at day 57 (week 8) following eight applications of eHAM. This patient did not show typical defect healing which could be due to advanced age or because of multiple co-morbidities.
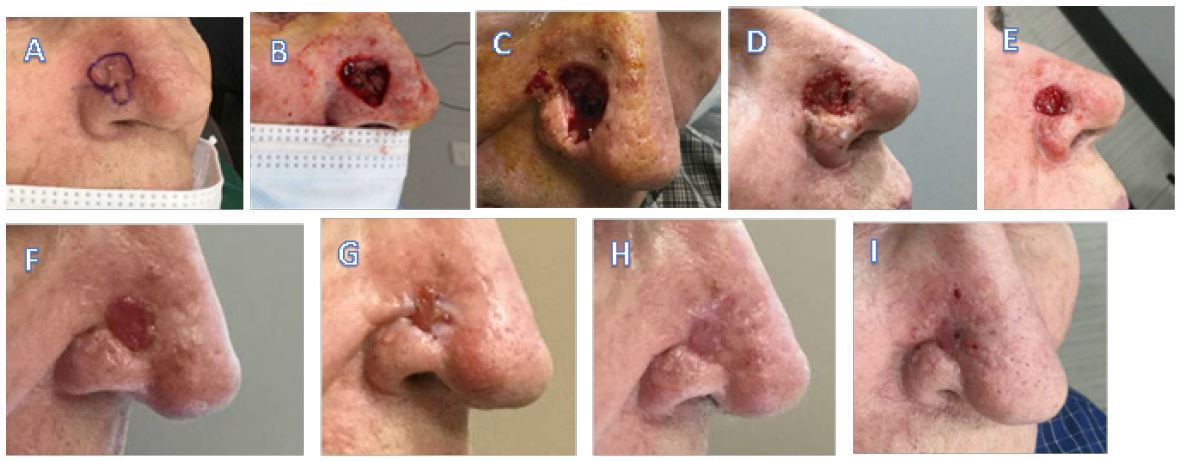
Figure 6: Case 6 shows the right nasal sidewall of a patient with Images showing A) pre-operative, B) defect following Mohs surgery, C) day 8 eHAM application, D) at day 17, E) at day 33 F) at day 40, G) at day 47, H) at day 54, and I) at day 60.

Figure 7: Case 7 shows the right crus of the ear with images showing A) pre-operative, B) following eHAM application at day 16, C) at day 26, D) at day 41 and E) at day 57.
Case 8 (Figure 8) is a 77 y/o male with no comorbidities who underwent Mohs surgery for a nodular basal cell carcinoma of the right posterior auricle. Images include A) pre-operative, B) defect following Mohs surgery, C) day 9, D) day 30, E) day 37, and F) and final image at day 52. The final eHAM application was on day 37 (week 5). The initial defect area was 3.2 cm2 that decreased to 0.4 cm2 at day 52 (week 7) following six applications of eHAM.

Figure 8: Case 8 showing the right posterior auricle of the ear. Images shown: A) pre-operative, B) defect following Mohs surgery, C) at day 9, D) at day 30, E) at day 37, and F) at day 52.
Results Summary
Figure 9 is a compiled graph comparing wound area closure to number of weeks of treatment for the 20 Mohs surgical defects in the case study. The average initial wound defect area with exposed cartilage was 3.73±3.30 cm2 and ranged from 0.70 to 13.50 cm2. The average final defect area was 0.57±0.67 cm2 and ranged from 0.01 to 3.10 cm2 (Table 2). The average area defect closure was 77±23% during eHAM treatment that required an average of 7±3 weeks for defect closure. During treatment, the number of eHAM applications ranged from 2-14 applications for these 20 patients that were treated on the study. None of the 20 defects in the study required skin grafts for wound closure.
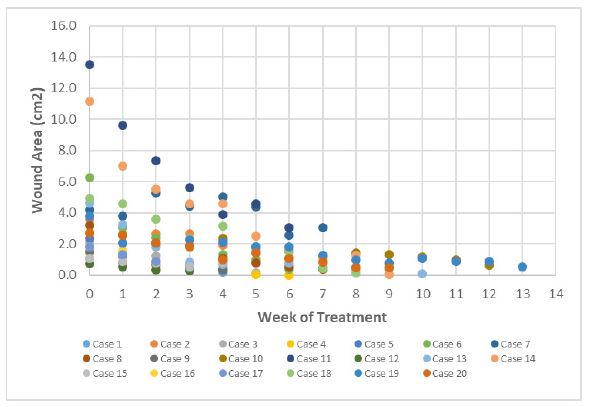
Figure 9: Comparison of wound area closure to number of weeks of treatment for 20 patients who received Mohs surgery followed by eHAM treatment.
Discussion
MMS challenges
Mohs Micrographic Surgery (MMS) is the standard of care for the treatment of cutaneous malignancies of the face, nose, and ears [1]. Following MMS to remove basal cell carcinomas, there are fewer reoccurrences compared to other types of treatments [25]. The MMS creates a wound defect that allows complete evaluation of the surgical margins with maximum tissue preservation [26]. However, MMS defects with exposed cartilage are typically more painful and can take longer to heal. A dermal regenerative matrix composed of a 3-dimensional porous matrix, bovine collagen, and chondroitin-6-sulphate was previously shown to be an effective treatment following MMS [27]. However, this treatment provides only a temporary surgical wound dressing while waiting for skin grafting that may take up to three weeks or more to be eventually placed on the wound bed for wound closure.
Additional challenges are caused by exposed cartilage during MMS that pose a threat to wound healing. The avascular structure of cartilage may be barrier to sustaining a Full Thickness Skin Graft (FTSG). As a results, FTSGs have an increased risk of necrosis and graft failure when placed directly on exposed cartilage. In some locations, such as the ear, the risk of graft necrosis may be reduced by making cartilage windows in hopes to access vascular beds underneath the cartilage. However, such practices are not universally successful. Additionally, defects with exposed cartilage are often quite deep. Therefore, placing a FTSG on them at the time of surgery may result in a permanent contour deformity (i.e. divot) in the skin. This may not always be overcome by taking a thicker graft because as the graft becomes “thicker” its metabolic demand will increase. The increase metabolic demand (especially when combined with the low vascular supply of cartilage) increases the risk of necrosis and graft failure. In the case of a deep MMS defect involving cartilage, secondary intent healing followed by a delayed FTSG may be utilized. Delayed grafting allows granulation tissue to partially fill the defect, thereby reducing the risk of a contour deformity while providing a more robust vascular bed for graft sustenance. The use of eHAM provides mitigation of some of these challenges encountered from MMS defects with exposed cartilage. Using eHAM allows a relatively pain free experience for the patient and effective method of healing wounds with cartilage exposure. The eHAM effectively granulates a wound prior to reepithelization of the tissue. The result is an improved cosmetic and functional outcome vs. FTSG and other traditional reconstruction options.
Comparison to other studies
In a study by Dessy et al., eHAM was applied following non-melanoma skin cancer MMS in 10 patients to repair defects with basal cell carcinoma (n=8) and squamous cell carcinoma (n=2) [28]. Similar to our study, the range in age was 65-78 years with defect sites located on the nose (1 patient with columella, 6 patients with nasal ala/side wall, 3 patients with dorsum/tip). Following MMS, a single eHAM application was applied to the defect. Skin grafting was performed 14-21 days after MMS and at the last dressing change. Skin grafting take was between 90-99% and complete wound healing was achieved 25-35 days (average 4.3 weeks) after MMS. No infections or graft rejection was reported. All patients remained tumor-fee during a 2-year follow-up period. For our study, we observed the best results when eHAM was removed and then applied weekly. This treatment plan was modified from the protocol in which eHAM remains in place for 2-3 weeks which normally allows vascularization to occur. Our 20 patients required 2 to 13 weeks (average 7±3 weeks) but were spared excess trauma associated with skin grafts. No infections, rejection, or reoccurrence of tumor was observed in the current study.
Historically at our facility prior to use of eHAM, these types of Mohs defects would have been repaired utilizing secondary intent, FTSG, or a skin flap. The specific type of reconstruction would have been chosen based on the individual defect with careful consideration of available tissue reservoirs and anatomy while optimizing overall cosmesis and function. Wound defect sizes would be comparable to what was seen in this study, but that is not a data point we routinely track in our facility. In general, FTSG and skin flaps offer a shorter healing time, but involve a larger, more complicated, and more painful surgical procedure for the patient. Secondary intent healing, in general, has been well received by patients but anecdotally the healing time was 3-4 weeks longer when compared to patients who utilized eHAM. Also, anecdotally, there has been increased patient and surgeon satisfaction with the final cosmetic appearance of the fully healed wound when eHAM has been utilized when compared to secondary intent healing.
In this study, 20 patients with cartilage exposed MMS surgical wound defects were evaluated for wound defect closure using an eHAM regenerative dermal matrix. The MMS procedure was used for removal of basal cell and squamous cell cutaneous carcinomas located on the nose and ear. None of the 20 patients required skin grafting following eHAM treatment thereby, sparing the patients additional pain or possible complications. In this study, 2-14 applications of eHAM alone were sufficient at reducing the wound area defect by an average of 77±23% during the treatment period. Eighteen of the 20 patients had >50% defect closure after 2-13 weeks of eHAM treatment with only 2 patients being less responsive at 26% defect closure. The average initial wound defect area was 3.73±3.30 cm2 (range 0.70 to 13.50 cm2) and average final defect area was 0.57±0.67 cm2 (range 0.01 to 3.10 cm2). The time to wound defect closure required an average of 7±3 weeks (range 2-13 weeks) and the average rate of defect closure was 0.65±1.00 cm2/week. According to clinician observation, the cosmetic appearance was excellent in all patients following MMS and eHAM treatment. All patients received a prescription for pain medications to use as needed but, most did not utilize them during the post-surgery period.
Conclusion
In this retrospective study, we evaluated 20 patients with defects involving exposed cartilage following MMS for cutaneous malignancies of the head and neck. These included 16 cases of the nose and four cases of the ear. None of the patients required skin grafts, skin flaps, scar revisions, or other invasive surgery following treatment with an eHAM regenerative dermal substitute. One patient required hydrocodone – acetaminophen for post-surgical pain. Otherwise, patients complained of minimal to no pain. Patients were pleased with the final achieved cosmesis, and function of the surgical sites once healed. We conclude treatment with eHAM can promote healing with a good cosmetic and functional outcome for MMS defects involving cartilage. Furthermore, most patients treated with eHAM appear to experience minimal pain following MMS and during the eHAM treatment period. In conclusion, eHAM appears to be an effective option to consider for the healing of MMS defects with exposed cartilage defects of the nose and ear.
Declarations
Funding: No funding was received by the authors.
Conflict of interest: The author declares that they have no known competing financial interests that could have appeared to influence the work reported in this manuscript. Medline Industries, LP provided medical writing support for the manuscript. The body of the manuscript, the choice of cases and conclusions were at the sole discretion of the author.
Availability of data and material: The data that support the findings of this study are proprietary and are not publicly available.
Ethics approval: This was a retrospective study that reflects the use of standard practice at Forefront Dermatology. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent to participate. Written informed consent was obtained from all participants in the study.
Consent for publication: All patients signed consent and approval for the use of the images taken during the course of their treatment.
Acknowledgement: The author acknowledges the manuscript writing support provided by Stephen Smith, PhD. Sr Medical Writer, Medline Industries, LP.
Author agreement: The manuscript, including related figures, has not been previously published and is not under consideration elsewhere. The named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship, take responsibility for the integrity of the work, agrees to be accountable for all aspects of the work. All of the authors have read and approved the final version.
References
- Dibelius GS, Toriumi DM. Reconstruction of Cutaneous Nasal Defects. Facial Plast Surg Clin North Am. 2017; 25(3): 409-426.
- Paoli J, Gyllencreutz JD, Fougelberg J, Backman EJ, Modin M, et al. Nonsurgical Options for the Treatment of Basal Cell Carcinoma. Dermatol Pract Concept. 2019; 9(2): 75-81.
- Bittner GC, Kubo EM, Fantini BC, Cerci FB. Auricular reconstruction after Mohs micrographic surgery: Analysis of 101 cases. Ann Bras Dermatol. 2021; 96(4): 408-415.
- Thomas CL, Lam A, Lam J, Paver R, et al. Factors affecting choice of repair in Mohs micrographic surgery for non-melanoma skin cancer of the head. Australas J Dermatol. 2017; 58(3): 189-193.
- Cook TA, Miller PJ. Auricular reconstruction. Facial Plast Surg. 1995 Oct; 11(4): 319-29.
- Immerman S, White WM, Constantinides M. Cartilage grafting in nasal reconstruction. Facial Plast Surg Clin North Am. 2011; 19(1): 175-82.
- Nemir S, Hunter-Ellul L, Codrea V, Wagner R. Reconstruction of a Large Anterior Ear Defect after Mohs Micrographic Surgery with a Cartilage Graft and Postauricular Revolving Door Flap. Case Rep Dermatol Med. 2015; 2015: 484819.
- Zhang AY, Meine JG. Flaps and grafts reconstruction. Dermatol Clin. 2011; 29(2): 217-30.
- Brandão CM, Weimann ETS, Terzian LR, Machado Filho CDS, Paschoal FM, et al. Keep it simple. A ten-year experience in reconstructions after Mohs micrographic surgery. An Bras Dermatol. 2020; 95(6): 714-720.
- Kimyai-Asadi A, Goldberg LH, Peterson SR, Silapint S, Jih MH. The incidence of major complications from Mohs micrographic surgery performed in office-based and hospital-based settings. J Am Acad Dermatol. 2005; 53(4): 628-34.
- Leibovitch I, Huilgol SC, Hsuan JD, Selva D. Incidence of host site complications in periocular full thickness skin grafts. Br J Ophthalmol. 2005; 89(2): 219-22.
- Cerci FB. Versatility of advancement flaps for nasal reconstruction following Mohs` micrographic surgery. Ann Bras Dermatol. 2018; 93(5): 719-722.
- Connolly KL, Nehal KS, Dusza SW, Rossi AM, Lee EH. Assessment of intraoperative pain during Mohs micrographic surgery (MMS): An opportunity for improved patient care. J Am Acad Dermatol. 2016; 75(3): 590-594. Epub 2016 Apr 25. Erratum in: J Am Acad Dermatol. 2017; 77(4): 794.
- Kamangar F, Petukhova TA, Monico G, Mathis S, Joo J, et al. Anxiety levels of patients undergoing common dermatologic procedures versus those seeking general dermatologic care. Dermatol Online J. 2017; 23(5): 13030/qt64d8r1gq.
- Newsom E, Lee E, Rossi A, Dusza S, Nehal K. Modernizing the Mohs Surgery Consultation: Instituting a Video Module for Improved Patient Education and Satisfaction. Dermatol Surg. 2018; 44(6): 778-784.
- Biro M, Kim I, Huynh A, Fu P, Mann M, et al. The use of 3-dimensionally printed models to optimize patient education and alleviate perioperative anxiety in Mohs micrographic surgery: A randomized controlled trial. J Am Acad Dermatol. 2019; 81(6): 1339-1345.
- Carucci JA, Kolenik SA 3rd, Leffell DJ. Human cadaveric allograft for repair of nasal defects after extirpation of Basal cell carcinoma by Mohs micrographic surgery. Dermatol Surg. 2002; 28(4): 340-3.
- Mast BA, Haynes JH, Krummel TM, Diegelmann RF, Cohen IK. In vivo degradation of fetal wound hyaluronic acid results in increased fibroplasia, collagen deposition, and neovascularization. Plast Reconstr Surg. 1992; 89(3): 503-9.
- Simman R, Hermans MHE. Managing Wounds with Exposed Bone and Tendon with an Esterified Hyaluronic Acid Matrix (eHAM): A Literature Review and Personal Experience. J Am Coll Clin Wound Spec. 2018; 9(1-3): 1-9.
- Bourguignon LY. Matrix hyaluronan-activated CD44 signaling promotes keratinocyte activities and improves abnormal epidermal functions. Am J Pathol. 2014; 184(7): 1912-9.
- Onesti MG, Fino P, Ponzo I, Ruggieri M, Scuderi N. Non-surgical treatment of deep wounds triggered by harmful physical and chemical agents: A successful combined use of collagenase and hyaluronic acid. Int Wound J. 2016; 13(1): 22-6.
- Turner NJ, Kielty CM, Walker MG, Canfield AE. A novel hyaluronan-based biomaterial (Hyaff-11) as a scaffold for endothelial cells in tissue engineered vascular grafts. Biomaterials. 2004; 25(28): 5955-64.
- Motolese A, Vignati F, Brambilla R, Cerati M, Passi A. Interaction between a regenerative matrix and wound bed in nonhealing ulcers: results with 16 cases. Biomed Res Int. 2013; 2013: 849321
- Iorio ML, Shuck J, Attinger CE. Wound healing in the upper and lower extremities: A systematic review on the use of acellular dermal matrices. Plast Reconstr Surg. 2012; 130(5 Suppl 2): 232S-241S.
- Roscher I, Brevig T, Mørk G, Helsing P, Gjersvik P. Mohs’ kirurgi ved basalcellekarsinom i ansiktet [Mohs surgery in basal cell carcinoma on the face]. Tidsskr nor Laegeforen. 2011; 131(24): 2475-9. Norwegian.
- Cortés-Peralta EC, Garza-Rodríguez V, Vázquez-Martínez OT, Gutiérrez-Villarreal IM, et al. micrográfica de Mohs: 27 años de experiencia en el Noreste de México [Mohs micrographic surgery: 27-year experience in the Northeast of Mexico]. Cir Cir. 2017; 85(4): 279-283.
- Loh CY, Loh M, Mashhadi SA. Integra as a temporary method of wound cover post Mohs surgery. Int Wound J. 2016; 13(1): 143.
- Dessy LA, Marcasciano M, Fanelli B, Mazzocchi M, Ribuffo D. Surgical treatment of nasal non-melanoma skin cancer in elderly patients using dermal substitute. Acta Otolaryngol. 2016; 136(12): 1299-1303.
