
Open Access, Volume 10
Complications of cardiac surgery - post pump chorea
Petr Hollý1*; Petr Dušek1,2; Petra Reková1; Manuela Vaneckova2; Hana Brožová1
1Department of Neurology and Centre of Clinical Neuroscience, First Faculty of Medicine, Charles University and General University Hospital in Prague, Czech Republic.
2Department of Radiology, First Faculty of Medicine, Charles University and General University Hospital in Prague, Czech Republic.
Petr Hollý
Department of Neurology and Centre of Clinical Neuroscience, Charles University, 1st Faculty of Medicine and General University Hospital in Prague, 30, 128 08, Praha 2, Czech Republic.
Tel: +420-721634451;
Email: petr.holly@vfn.cz
Received : June 01, 2024,
Accepted : June 18, 2024
Published : June 20, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Post-pump chorea is a relatively common complication of cardiac surgery in childhood (0.6-3%). If it develops in adulthood, it is often permanent and less responsive to treatment. We report a case of a 47-year-old woman who developed chorea in all limbs 15 days after cardiac surgery (thrombectomy of a prosthetic aortic valve, reoperation 12 years after Bentall operation for type A aortic dissection). Symptomatic treatment with haloperidol led to amelioration of involuntary movements. This case illustrates both the rare occurrence of post-pump chorea in adulthood and the follow-up of this patient for 8 years.
Keywords: Abnormal movements; Movement disorders; Neuroimaging; Neuroleptics; Post-pump chorea.
Abbreviations: MRI: Magnetic Resonance Imaging; PPC: Post-Pump Chorea.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Hollý P (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Hollý P, Dušek P, Reková P, Vaneckova M, Brožová H. Complications of cardiac surgery - post pump chorea. Open J Clin Med Case Rep. 2024; 2259.
Introduction
Post-Pump Chorea (PPC) is a common complication of cardiac surgery in childhood, and it is rare in adulthood. If it appears, it is often permanent and insufficiently responsive to treatment.
Here we report a case of a 47-year-old female patient with sudden onset of chorea of all four limbs following cardiac surgery in extracorporeal circulation with hypothermia. The patient had a history of Bentall’s surgery - aortic valve replacement for type A dissection at the age of 35 years.
Case Presentation
The story of our patient has begun in 2004, when she was 35 years old, at 23rd weeks of gestation, and had an aortic dissection type A. She had undergone Bentall’s procedure, replacing the ascending aorta and aortic valve. The patient was followed up regularly until she was diagnosed with a pseudoaneurysm arising from the medial margin of the distal part of the anastomosis, and this finding progressed over time (to a size of 45x29 mm with mural thrombus). Reoperation including thrombectomy of the prosthetic aortic valve was performed in the autumn of 2016, approximately 12 years after the initial surgery; the patient was 47 years old.
The cardiac surgery was prolonged, the patient was on extracorporeal circulation for 496 minutes, and cardiac arrest in hypothermia lasted 70 minutes in total. She was transiently severely desaturated with the lowest value of blood oxygen saturation reaching 30% measured by near-infrared spectroscopy.
The day after surgery, the patient was extubated early and awakened to full contact. Upon awakening, clinical manifestations of psychoorganic syndrome (slowed psychomotor pace, longer response latency) were present.
The postoperative course was complicated by the development of pneumothorax treated by chest drainage, and compartment syndrome of the right calf treated by fasciotomy. Due to the development of severe bacterial pneumonia caused by Serratia marcescens, the patient had to be reintubated. She was treated with meropenem and vancomycin.
The first contact with the neurological consultant took place on the 15th postoperative day, when the patient developed abnormal movements in all limbs - chorea and ballism. A total of 1200 mg of tiapridal per day and 2 mg of clonazepam per day was administered. Due to ineffectiveness, the therapy was switched to haloperidol 10 mg per day, and the patient, already in a cardiopulmonary stable condition, was admitted to our neurological department on the 28th postoperative day.
On admission, the patient showed severe chorea of all four limbs with a mild dystonic component and hypotonia. The involuntary movements involved also the proximal parts of upper limbs with a slight right-sided predominance consistent with the definition of ballism. On haloperidol therapy, dyskinesias gradually improved.
Among the examinations performed beyond the basic laboratory tests, an autoimmune panel including antineutrophil cytoplasmic antibodies, antibodies to glutamic acid decarboxylase, antinuclear antibodies, and antiphospholipid antibodies were examined, which was negative. According to the consultation of the cardiologist, Marfan’s syndrome or other collagenopathy was not considered as a cause of vascular disorder in the past. Brain Magnetic Resonance Imaging (MRI) under general anaesthesia was performed showing increased T1 signal in the bilateral globus pallidus and posterior putamen (Figure 1) and multiple small cerebral microbleeds mainly in white matter and in basal ganglia (Figure 2). Single-photon emission tomography of the brain with 99m Tc hexamethylpropyleneaminoxime (HMPAO-SPECT) showed no perfusion abnormalities in basal ganglia. Follow-up brain MRI performed after 4 months showed partial resolution of basal ganglia T1 signal abnormalities (Figure 1).
The condition was clinically concluded as post-pump chorea after prolonged surgery in extracorporeal circulation with hypothermia. During the hospitalisation, the patient gradually improved, she could walk with a four-wheel walker. After the hospital discharge, she was able to walk without any support at home. The patient was hospitalized in a rehabilitation facility and subsequently attended outpatient rehabilitation. Ten months after the surgery haloperidol was discontinued due to fatigue and sleepiness with mild accentuation of chorea; instead, 3 mg of risperidone daily was introduced with effect.
Currently, she has difficulty with activities of daily living such as hygiene, showering or routine housework due to instability of standing and walking mainly due to chorea. She can eat alone but not prepare food. She can walk unsupported around the home and uses a four-wheeled walker for longer distances. She is temporarily working part-time as a gatekeeper.
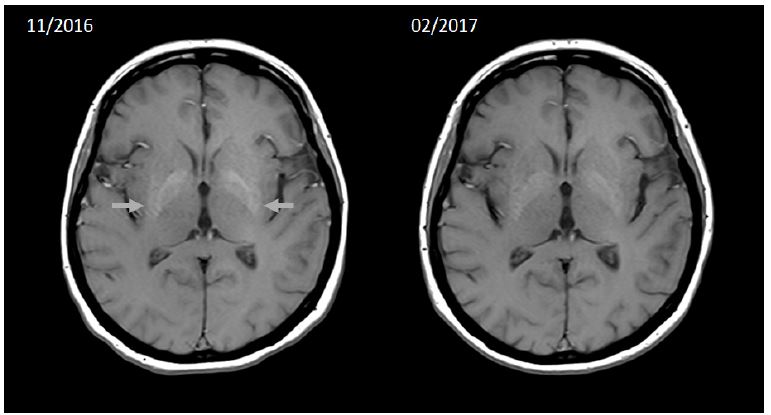
Figure 1: Axial T1 weighted image showing increased T1 signal in the bilateral globus pallidus and posterior putamen (grey arrows) which is almost normalized on a follow-up scan after 3 months. Both scans were acquired using the same scanner (Siemens Skyra 3T, Siemens Healthcare, Erlangen, Germany), and pulse sequence parameters (echo time = 6.4 ms, repetition time = 600 ms, flip angle = 150°, spatial resolution = 0.43x0.43x4 mm3).
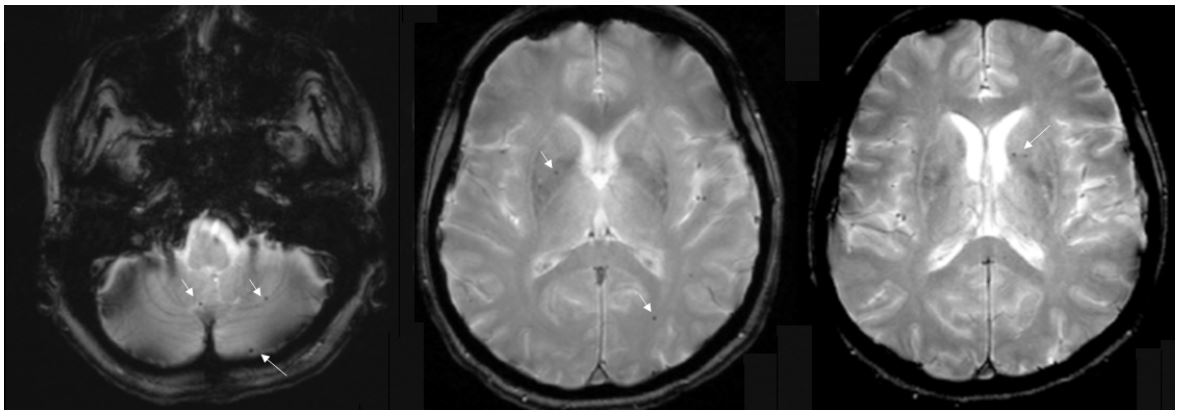
Figure 2: Axial T2* weighted image showing multiple cerebral microbleeds in the deep white matter, cerebellum, and basal ganglia (white arrows). Scan was acquired using the Siemens Skyra 3T (Siemens Healthcare, Erlangen, Germany) scanner and following pulse sequence parameters: echo time = 19.9 ms, repetition time = 675 ms, flip angle = 20°, and spatial resolution = 0.69x0.69x4 mm3.
Discussion
Cardiac surgery comes with many risks. The neurological ones include the development of involuntary movements following the procedure referred to as PPC. There is a higher incidence of PPC in the paediatric population reaching 0.6-3% [1] and it usually develops within 2 weeks of surgery [2].
The first descriptions of this disorder were from the 1960s [3,4]. The 10-year period follow-ups of children with PPC were published in 1993 [2]. Of the 668 children who underwent open heart surgery, 8 children (1.2%) developed PPC. The onset of symptoms in these children began between postoperative days 3 and 12. Computed tomography and MRI of the brain showed brain atrophy but no focal lesions. 18F Fluorodeoxyglucose Positron Emission Tomography (FDG-PET) of the brain showed patchy areas of decreased glucose metabolism. Of these paediatric patients, 3 had transient chorea symptoms and 5 had persistent chorea. There are very few described reports of PPC in adulthood [5-7].
The movement disorders in the reported patient occurred on day 15 after surgery. The postoperative period was burdened by numerous complications (pneumothorax, compartment syndrome in the lower limb, bacterial pneumonia with respiratory insufficiency and the need for artificial pulmonary ventilation). The pathophysiology of PPC in our patient is unknown, probably related to transient hypoxia with basal ganglia damage which is apparent as their increased T1 signal on brain MRI (in the differential diagnosis of these lesions is hyperglycaemia, which the patient did not have). These changes on brain MRI are reversible over time [8]. A study [7] comparing patients with PPC with patients without PPC after cardiac surgery concluded that lower body temperature during hypothermia and prolonged cardiac arrest during surgery are involved in the development of neurologic symptoms. Other authors considered low oesophageal temperature during surgery [9], deeper hypothermia (below 20°C), prolonged cardiac arrest [2], faster re-warming[10], and longer hypothermia time as risk factors. The sudden drop in partial pressure of carbon dioxide during re-warming may potentiate vasoconstriction of cerebral arteries and may lead to transient hypoxic damage [11]. In the case of our patient, the operation was complicated by several of these risk factors, especially prolonged cardiac arrest, and prolonged state of hypothermia. To date, there is no published case of an adult patient who had two complex cardiac surgeries in their lifetime (in our case, the first surgery combined with Caesarean delivery).
Combination of clonazepam and haloperidol therapy and later risperidone monotherapy were partially effective for a long-time alleviating chorea. According to the literature, risperidone [12] or tetrabenazine therapy may be effective [5].
Conclusion
PPC is one possible cause of chorea. Unlike in childhood, where this complication of extracorporeal circulation is common, in adulthood, it is very rare but should be considered. We present the case of a patient after two major cardiac surgeries and her follow-up for 8 years. As in the previously described cases, the therapeutic options are very limited, and the effect is not great - neuroleptic (preferably an atypical such as risperidone) or the dopamine depletor, tetrabenazine, should be administered.
Declarations
Acknowledgements: The authors thank the patient for her kind consent to publish this case report. Our thanks also go to the staff of the Radiodiagnostic Dept. 1st Faculty of Medicine Charles University and General University Hospital in Prague and the staff of the rehabilitation institutes where the patient was rehabilitated. Informed consent is available from the corresponding author upon request.
Financial disclosures: This study was supported by MH CZ-DRO-VFN64165 and The project National Institute for Neurological Research (Programme EXCELES, ID Project No. LX22NPO5107) – Funded by the European Union – Next Generation EU.
P.D. received funding from the Czech Ministry of Health and honoraria from Alexion Pharmaceuticals. The authors declare that there are no additional disclosures to report.
Ethical compliance statement: All 5 authors stated: “we confirm that we have read the journal’s position on issues involved in ethical publication and affirm that this work is consistent with those guidelines”.
References
- Kirkham FJ, Haywood P, Kashyape P, Borbone J, Lording A, et al. Movement disorder emergencies in childhood. Eur J Paediatr Neurol. 2011; 15(5): 390-404. doi:10.1016/j.ejpn.2011.04.005
- Medlock MD, Cruse RS, Winek SJ, Geiss DM, Horndasch RL, et al. A 10-year experience with postpump chorea. Ann Neurol. 1993; 34(6): 820-6. doi:10.1002/ana.410340611
- Björk VO HG. Brain Damage in Children after Deep Hypothermia for Open-heart Surgery. Thorax. 1960; 15: 284-291.
- Bergouignan M, Fontan F, Trarieux M, Julien J. [Choreiform syndromes in children during cardiosurgical operations under deep hypothermia]. Rev Obstet Ginecol Venez. 1961; 105: 48-60.
- Saft C, Reber D, Streuer M, Andrich J. Post pump chorea in a 77-year-old male. Neurol Sci. 2011; 32(4): 699-701. doi:10.1007/s10072-011-0583-7
- Park KW, Choi N, Ryu HS, Kim HJ, Lee CS, et al. Post-Pump Chorea and Progressive Supranuclear Palsy-Like Syndrome Following Major Cardiac Surgery. Mov Disord Clin Pract. 2020; 7(1): 78-82. doi:10.1002/mdc3.12867
- Ahn JH, Song J, Choi I, Youn J, Cho JW. Risk factors and prognosis of adult-onset post-pump chorea. J Neurol Sci. 2021; 422: 117328. doi:10.1016/j.jns.2021.117328
- Di Luca DG, Swinkin E, Lang A. Teaching Video NeuroImage: Reversible Caudate Changes in a Patient With Post-Pump Chorea. Neurology. 2022; 98(17): 731-732. doi:10.1212/WNL.0000000000200339
- Levin DA, Seay AR, Fullerton DA, Simoes EA, Sondheimer HM. Profound hypothermia with alpha-stat pH management during open-heart surgery is associated with choreoathetosis. Pediatr Cardiol. 2005; 26(1): 34-8. doi:10.1007/s00246-004-0669-6
- DeLeon S, Ilbawi M, Arcilla R, Cutilletta A, Egel R, et al. Choreoathetosis after deep hypothermia without circulatory arrest. Ann Thorac Surg. 1990; 50(5): 714-9. doi:10.1016/0003-4975(90)90668-v
- Passarin MG, Romito S, Avesani M, Alessandrini F, Petrilli G, et al. Late-onset choreoathetotic syndrome following heart surgery. Neurol Sci. 2010; 31(1): 95-7. doi:10.1007/s10072-009-0171-2
- Das P, Shinozaki G, McAlpine D. Post-pump chorea--choreiform movements developing after pulmonary thromboendarterectomy for chronic pulmonary hypertension presenting as functional movement disorder. Psychosomatics. 2011; 52(5): 459-62. doi:10.1016/j.psym.2011.01.022
