
Open Access, Volume 10
Breast parenchyma leiomyoma: A diagnostic challenge to treat
Georgiou IA1; Rigas GI2; Kritikos NG1; Arkoumani ED3; Mpoti EI3; Nicholaos Kelessis G4*
1Breast Imaging Department, «St. Savvas» Oncologic Hospital, Athens, Greece.
2Breast Surgery Department, «St. Savvas» Oncologic Hospital, Athens, Greece.
3Pathology Department, «St. Savvas» Oncologic Hospital, Athens, Greece.
4Head of Surgical Oncology Department, “Therapis” General Hospital, Athens, Greece.
Nikolaos Kelessis
Head of Surgical Oncology Department, “Therapis” General Hospital, Athens, Greece.
Email: nkelessis@doctors.org.uk
Received : May 24, 2024,
Accepted : June 12, 2024
Published : June 20, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Breast leiomyoma is an infrequent entity and accounts for less than 1% of all breast tumors. The disease may affect both sexes with a preference for middle-aged women and its etiology still remains unclear. The nipple and subareolar area harbor the neoplasm in the majority of cases, however the intraparenchymal location, especially in older women has been noted. Histologically, this mesenchymal tumor derives from smooth muscle cells metaplasia or from myofibroblastic cells of the subareolar area. Triple assessment makes up the basic diagnostic tool. Surgical resection in macroscopic clear margins contributes not only to diagnosis but also rules out malignancy. Herein, we present our case of intramammary leiomyoma with a parallel review of world literature.
Keywords: Breast; Leiomyoma; Mammogram; Benign; Immunohistochemistry.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kelessis NG (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Georgiou IA, Rigas GI, Kritikos NG, Arkoumani ED, Mpoti EI, Kelessis NG. Breast parenchyma leiomyoma: A diagnostic challenge to treat. Open J Clin Med Case Rep. 2024; 2256.
Introduction
Intraparenchymal breast leiomyoma is an extremely rare non-epithelial mesenchymatic lesion which accounts for less than 1% of all breast tumors and since 2018 only 31 cases are referred to in world literature [1,2]. It may occur in both sexes; however women between the ages of 30 and 60 with a mean age of 45 exhibit the neoplasm in the majority of cases [3]. Based on the origin site, two types have been described. One is superficial, deriving from dermal smooth muscles, and affects the nipple-areola complex; the other a vascular type from the endothelium which is usually located deep in breast parenchyma and represents an extremely atypical site [3,4]. Histopathology usually demonstrates interlacing fascicles of spindle-shaped cells with oval nuclei with no atypia and low mitotic activity [5]. Symptoms apart from a painless and an occasionally palpable nodule are unremarkable. Ultrasound usually exposes a hypoechoic oval shape nodule, with no detectable Doppler flow, while the mammogram reveals a dense, well-circumscribed oval lesion without microcalcifications [6]. Due to the lack of distinct characteristics in imaging and the similarities with other benign and malignant lesions, surgical excision in macroscopic clear margins is highly recommended. In several cases where a tru-cut biopsy is applied, diagnosis may comprise a challenge due to small and inadequate material. Then, a differential diagnosis should involve entities which exhibit imaging and pathological similarities with leiomyoma. Among them, phyllodes tumors, fibroadenomas, myoepitheliomas, myoids and hamartomas incorporate the benign lesions, while leiomyosarcoma and metaplastic carcinoma represent the malignant counterparts [7]. A complete excision with clear margins is an adequate treatment due to benign nature of the tumor.
Case Presentation
A 45-year-old Caucasian female attended our outpatient clinic during her annual follow-up, with a painless, palpable mass in the upper outer quadrant of her left breast. She denied family history with breast or gynecological malignancies and had never received hormonal therapy or other medication. A clinical examination revealed a painless palpable mobile lump in the aforementioned area at a distance of approximately 10 cm from the nipple. There was no axillary or supraclavicular lymphadenopathy. The other breast was into normal appearance and consistency. The lesion had incidentally been found two years previous to this during her annual mammogram and was originally considered to be fibroadenoma. That ultrasound had detected a hypoechoic oval shape nodule, with no detectable Doppler flow, located in the upper outer quadrant of the left breast, measuring 2.6 cm (Figure 1). The follow-up mammogram detected an enlarged, dense, well-circumscribed oval lesion with no calcifications inside or around, without lymphadenopathy (Figure 2). The lump was classified as category 4 according to BIRADS (Breast ImagingReporting and Data System) criteria. Based on clinical and imaging findings, a Tru Cut biopsy through U/S was then conducted. The resulting pathology revealed spindle cells with elongated cigar-shaped nuclei and eosinophilic cytoplasm (H+E stain x 20) (Figure 3). Despite the benign nature of the tumor, the patient was offered the option of surgical removal of the lump in order to avoid diagnostic dilemmas and pitfalls. A consent form was signed and under general anesthesia the lesion was resected in macroscopic clear margins leaving a drain in place. Postoperative course was without noteworthy incidence and the patient was discharged the hospital the next day. The pathology of the specimen showed intersecting fascicles of elongated smooth muscle cells with no atypia or mitotic activity. Immunohistochemistry depicted strong expression of desmin, a characteristic of smooth muscle neoplasms, which confirmed the diagnosis of leiomyoma, while the absence of p63 marker excluded metaplastic carcinoma (Figures 4,5). Two years after the operation the patient has no symptoms and the mammogram shows no evidence of recurrence.

Figure 1: Solid Mass with heterogeneous morphology without vascularization in Doppler image.
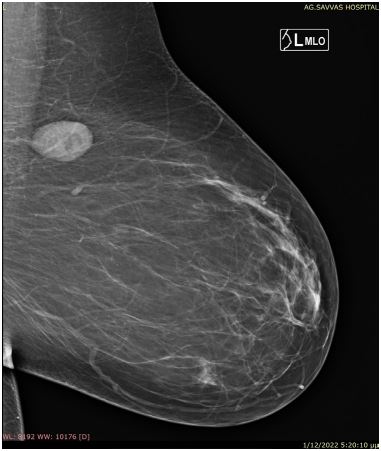
Figure 2: Round mass in the upper outer
quadrant of the left breast without lymph
nodes enlargement.
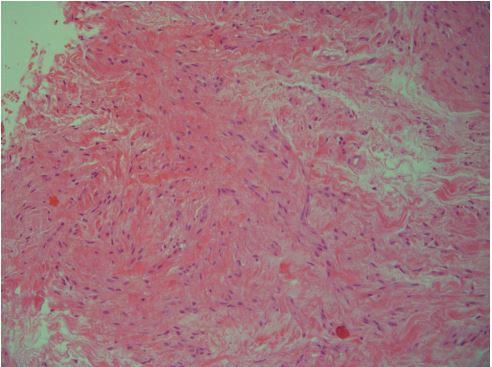
Figure 3: Higher magnification of the lesion showing
spindle cells with elongated cigar-shaped nuclei and eosinophilic cytoplasm. (H+E stain x 20).
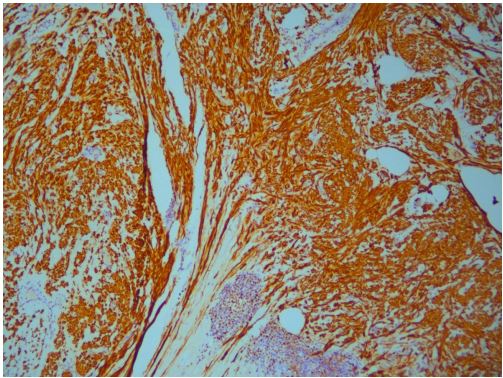
Figure 4: Strong and diffuse expression of desmin, a characteristic of smooth muscle neoplasms (magnification x10).
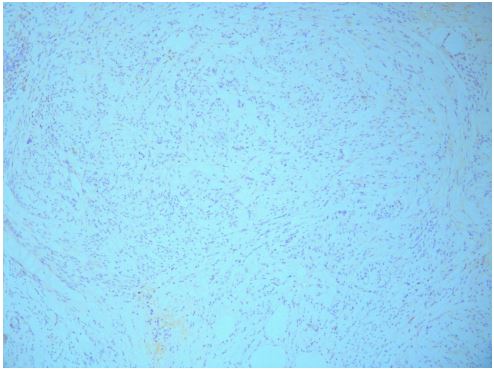
Figure 5: Absence of p63, a marker to exclude metaplastic
carcinoma (magnification x10).
Discussion
Intraparenchymal leiomyoma is an extremely rare entity and despite its first publication by Strong et al. [8] in 1913 the etiology still remains uncertain. In the vast majority of cases the neoplasm develops in the subareolar area presumably due to the increased amount of smooth muscle cells. Various theories have been put forward in an effort to explain the origin and evolution of this tumor in breast parenchyma. According to Kaufman and Hirsch [9], the tumor originates from the myocytes around the capillaries in the subcutaneous tissue. Melnick and Shauder [10,11] proposed the theory of the relocation of the multipotent mesenchymal cells deep in parenchyma during the embryologic period, while Diaz-Arias et al. [12] ruled out the scenario of the teratoid origin, supporting the hypothesis of the hypertrophy of myomatous elements. An intriguing assumption by Son EJ et al. [6] incorporates the tamoxifen use in the armamentarium of etiologic factors.
Intraparenchymal lesions are usually located in the right breast, are well-defined and their size varies greatly between 1.0-14.0 cm in diameter [13]. Clinical examination apart of a painless, motile, palpable mass is unremarkable in the majority of cases. No evidence of irritation, inflammation or nipple retraction has been observed. The role of imaging in the evaluation is very limited as leiomyomas exhibit no specific findings leading to diagnostic challenge. Radiologic findings of our patient were compatible with those referred to in the world literature. Due to the rarity of the lesion and the lack of distinct mammographic findings, a core biopsy under ultrasound guidance or a limited excisional biopsy in macroscopic clear borders is highly recommended. A careful pathological and immunohistochemical examination greatly contributes to differentiation of leiomyomas from other benign or malignant pathologies. Furthermore, a differential diagnosis from other tumors which share the same cellular origin is essential in order to choose the proper treatment. In certain cases, an overlap in morphological features of these lesions may be observed, which can lead to misdiagnosis, especially when the biopsied sample is too small or inadequate [14]. Leiomyosarcoma exhibits many similarities with intraparenchymal leiomyomas in mammogram. A low-grade leiomyosarcoma is a malignant tumor which may originate from smooth muscle cells of the breast. It tends to recur and metastasize long after surgery, however several microscopic characteristics, like the evidence of marked cellular atypia, increased numbers of mitoses (2-16 mitoses per 10 highpower fields), vascular invasion, and necrosis confirm the diagnosis of this aggressive neoplasm [15,16]. Conclusively, in cases where the immunohistochemistry, exhibits a positive test for smooth muscle actin and vimentin, interlacing fascicles of desmin, spindle cells, absent or low mitotic activity and a negative S100 protein, then the diagnosis of leiomyoma is settled upon. In our patient, the results of the pathological and immunohistochemical studies were compatible with those of the world literature.
Limited surgical excision in macroscopic clear margins is the treatment of choice for this benign lesion offering not only an accurate diagnosis but also helping to rule out malignancy. Very recently another treatment alternative, Ultrasound-Guided Microwave Ablation (US-MWA) has been applied, especially in. women with large tumors who desire the best cosmetic result [17].
Conclusion
Breast leiomyomas are extremely rare entities. Despite the plethora of etiologies about the origin of such a tumor, uncertainty still exists. Clinical and radiologic findings are not characteristic of the disease. Thus, Breast Surgeons, Oncologists and Pathologists must be aware of this rare lesion in order to avoid diagnostic dilemmas and pitfalls. Surgical resection is mandatory not only to set the diagnosis, but also to rule out malignancy.
References
- Rad FS, Zangivand AA. Breast leiomyoma: a case report and review of the literature. Comp Clin Pathol. 2014; 23: 483-5.
- Brandão RG, Elias S, Pinto Nazário AC, Alcoforado Assunção MDCG, Esposito Papa CC, et al. Leiomyoma of the breast parenchyma: a case report and review of the literature. Sao Paulo Medical Journal = Revista Paulista de Medicina. 2017; 136(2): 177-181. https://doi.org/10.1590/1516-3180.2016.0253040117
- Kafadar MT, Yalçın M, Gok MA, Aktaş A, Yürekli TC, et al. Intraparenchymal Leiomyoma of the Breast: A Rare Location for an Infrequent Tumor. Eur J Breast Health. 2017; 13: 156-158. DOI: 10.5152/ejbh.2017.3472
- Abd el-All HS. Breast spindle cell tumours: about eight cases. Diagn Pathol. 2006; 1: 13. doi: 10.1186/1746-1596-1-13.
- Pourbagher A, Pourbagher MA, Bal N, Oguzkurt L, Ezer A. Leiomyoma of the breast parenchyma. AJR Am J Roentgenol. 2005; 185(6): 1595-7.
- Son EJ, Oh KK, Kim EK, Son HJ, Jung WH, et al. Leiomyoma of the breast in a 50-year-old woman receiving tamoxifen. AJR. 1998; 171: 1684-1686.
- Granic M, Stefanovic-Radovic M, Zdravkovic D, Ivanovic N, Nikolic D, et al. Intraparenchimal leiomyoma of the breast. Arch Iran Med. 2015; 18: 608-612.
- Strong LW. Leiomyoma of the breast. Am J Obstet. 1913; 68: 53-5.
- Kaufman HL, Hirsch EF. Leiomyoma of the breast. J Surg Oncol. 1996; 62: 62-64. https://doi.org/10.1002/(SICI)1096-9098(199605)62:1<62::AID-JSO13>3.0.CO;2-V
- Melnick PJ. Fibromyoma of the breast. Arch Pathol. 1932; 14: 794-798.
- Schauder H. Über Leiomyome der Brustdrüse. Deutsche Zeitschrift für Chirurgie. 1927; 205(1): 58-68. http://link.springer.com/article/10.1007/BF02794721 Accessed in 2017 (Apr 26)
- Diaz-Arias AA, Hurt MA, Loy TS, Seeger RM, Bickel JT. Leiomyoma of the breast. Hum Pathol. 1989; 20: 396-399. https://doi.org/10.1016/0046-8177(89)90052-X.
- Vecchio GM, Cavaliere A, Cartaginese F, Lucaccioni A, Lombardi T, et al. Intraparenchymal leiomyoma of the breast: Report of a case with emphasis on needle core biopsy-based diagnosis. Pathologica. 2013; 105: 122-127.
- Magro G, Salvatorelli L, Puzzo L, Piombino E, Bartoloni G, et al. Practical approach to diagnosis of bland-looking spindle cell lesions of the breast. Pathologica. 2019; 111(4): 344-360. doi: 10.32074/1591-951X-31-19
- Stafyla VK, Gauvin JM, Farley DR. A 53-year- old woman with a leiomyosarcoma of the breast. Curr Surg. 2004; 61: 572-575. https://doi.org/10.1016/j.cursur.2004.05.008.
- Magro G. Mammary Myofibroblastoma: A tumor with a wide Morphologic Spectrum. Arch Pathol Lab Med. 2008; 132 (11): 1813-1820. https://doi.org/10.1043/1543-2165-132.11.1813
- Zhang S, Wang L, Yang J, Lu M. Ultrasound-guided microwave ablation for giant breast leiomyoma: A case report. Front Oncology. 2023; 13: 1095891. https://doi.org/10.3389/fonc.2023.109589.
