
Open Access, Volume 10
Endoprosthesis in distal esophageal perforations: A therapeutic possibility
Daniel Cuenca Leal*; Laura Alonso Murillo; Cristina Rihuete Caro; Victoria Antolín Sánchez; Maria Victoria Vieiro Medina; Marta de la Fuente Bartolomé; Victor Nieto Barros; Marta de Mingo Martin; Juan Felipe Vélez Pinto; Pedro Antonio Pacheco Martinez; Miguel Suárez Sánchez; Marta Urzay Gutiérrez; Marta Reguera Sánchez-Vera; Carlos García Vásquez; Santos Jiménez de los Galanes Marchán
Department of general and digestive surgery, Hospital Universitario Infanta Elena, Madrid, Spain.
Daniel Cuenca Leal
Department of general and digestive surgery, Hospital Universitario Infanta Elena, Madrid, Spain.
Email: daniel.cuenca@quironsalud.es
Received : May 20, 2024,
Accepted : June 07, 2024
Published : June 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Esophageal perforation presents a diagnostic and therapeutic challenge due to its variability in clinical manifestations and the lack of published literature.
Keywords: Esophageal perforation; Endoscopic stent; Esophagectomy; Esophagus; Boerhaave syndrome.
Abbreviations: EGJ: Esophagogastric Junction; CT: Computed Tomography; DET: Thoracic Endothoratic Tube; ICU: Intensive Care Unit; PTFE: Polytetrafluoroethylene.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Leal DC (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Leal DC, Murillo LA, Caro CR, Sánchez VA, Medina MVV, Bartolomé MF, Barros VN. Endoprosthesis in distal esophageal perforations: A therapeutic possibility. Open J Clin Med Case Rep. 2024; 2254.
Introduction
Esophageal perforation poses a diagnostic and therapeutic challenge due to its variable presentation and the lack of experience in its management. Published literature consists mainly of retrospective studies and expert opinions. Although perforations can occur anywhere in the esophagus, there is a preference for three key areas due to anatomical narrowing: the cricopharyngeal muscle, the bronchoaortic constriction, and the Esophagogastric Junction (EGJ) [1]. More than half of esophageal perforations are iatrogenic, mostly occurring during endoscopic procedures [2,3]. Spontaneous perforation or Boerhaave syndrome accounts for 15% of cases, while intraoperative injuries represent 2%. Other causes include foreign body ingestion (12%), trauma (9%), and malignancy (1%) [5].
The crucial principles in the initial management of esophageal perforation include early diagnosis, patient stabilization, and the choice of treatment, which should be evaluated multidisciplinarily. Regardless of etiology, esophageal perforation is a surgical emergency [5,6], as the leakage of esophageal and gastric contents into the mediastinal cavity involves a severe septic process that can lead to multiorgan failure and patient demise [7]. A delay in initiating treatment for this condition beyond 24 hours doubles its mortality [8].
Once diagnosed, managing esophageal perforation poses a therapeutic challenge. While primary surgical repair is considered the optimal procedure, factors must be considered that could negatively impact the outcome of this decision [9]. It is essential to individualize each case, evaluating various surgical alternatives to primary repair, including mediastinal drainage, placement of endoprostheses, and resective surgery (esophagectomy), among others [10].
Case Presentation
Summary of two clinical cases
A 70-year-old woman presented to the emergency room on 03/01/2020 with severe interscapular pain and dyspnea after a 12-hour vomiting episode. Chest Computed Tomography (CT) without contrast revealed left hydropneumothorax, pneumomediastinum, and left pleural effusion. Evaluation by a thoracic surgeon resulted in the placement of a left thoracic Endothoratic Tube (DET) with air and bilioenteric material drainage. A second CT with oral contrast, suspecting Boerhaave syndrome, showed gastrografin leakage into the left pleural space with a laminar wall defect on the left lateral aspect of the distal esophagus, approximately 4 x 15 mm. Due to the patient’s clinical stability, a conservative approach was chosen with Intensive Care Unit (ICU) admission for close monitoring and broad-spectrum antibiotic therapy. After 12-20 hours in the ICU, the patient experienced significant clinical deterioration, requiring intubation and vasoactive drugs. Emergency surgery, including thoracotomy and optimization of mediastinal drainage, revealed a phlogistic field with abundant purulent material and periesophageal necrosis. Intraoperative gastroscopy showed a linear esophageal perforation 5 cm long, 2 cm from the EGJ. Due to contamination intensity, time elapsed since diagnosis, and the patient’s hemodynamic instability, primary closure was ruled out, opting for a combined surgical-endoscopic approach. Endoscopic placement of a 125x23 mm WallFlex covered esophageal prosthesis was performed, securing the proximal end with two non-absorbable 3/0 transmural monofilament sutures (emergency conditions precluded endoscopic fixation) and a feeding jejunostomy. The patient had a slow but favorable postoperative course, requiring up to 5 prosthesis replacements spaced 3-4 weeks apart. The last prosthesis was removed on 09/04/2020, revealing an intact esophageal mucosa with no apparent discontinuity. The patient resumed oral intake without issues and was discharged on 21/04/2020, three and a half months after presenting to the emergency room. Due to the Covid-19 pandemic, the possibility of discharge between replacements was not considered.

Figure 1: CT scan upon arrival at the emergency department.
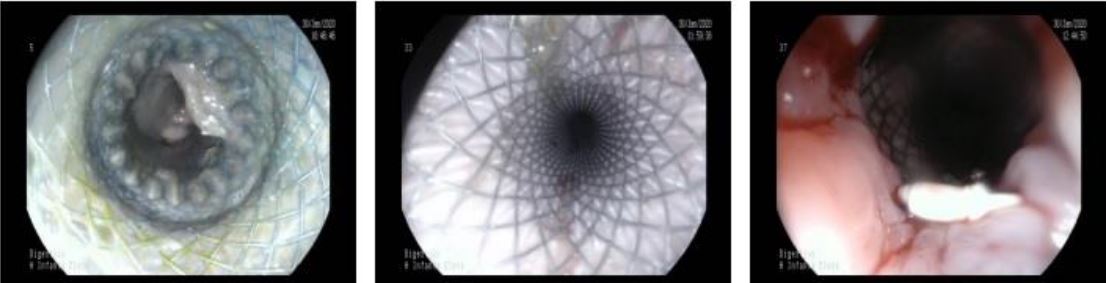
Figure 2: Second endoprosthesis replacement.
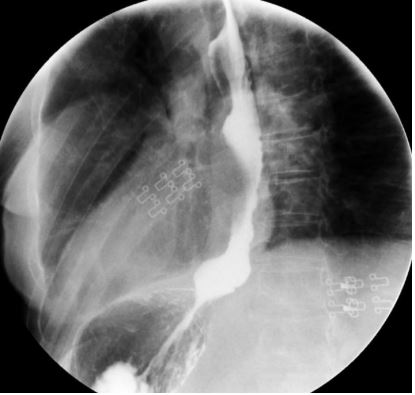
Figure 3: Esophagogastroduodenal transit one year after perforation.
A 67-year-old woman underwent surgery in February 2020 for a giant hiatal hernia containing the entire stomach and part of the transverse colon, with a diaphragmatic hiatus measuring 15x20 cm. CollisNissen fundoplication was performed (EGJ was at the carina level), and the hernial defect was corrected using a 7.5 x 10 cm PTFE (polytetrafluoroethylene) prosthetic mesh without complications at discharge. During outpatient follow-up, the patient reported progressive dysphagia, chest pain, regurgitation, vomiting, and occasional food impaction. A gastroscopy one year post-surgery revealed partial inclusion of the mesh in the esophageal lumen and Collis-Nissen gastroplasty. Initially managed conservatively, a slow mesh inclusion and worsening symptoms led to surgical revision in January 2022. Two perforations were found on the anterior and posterolateral aspects of the neoesophagus formed by the Collis gastroplasty, involving 70% of the circumference. Extrapulmonary mesh, forming an intrathoracic cavity adjacent to the perforation site, was resected. Intraoperative gastroscopy identified the perforation sites, which were sutured, and a Dor-type fundoplication was added, along with a feeding jejunostomy. Postoperatively, the patient experienced dehiscence of the primary perforation repair. Considering the complex situation, the high morbidity associated with esophageal replacement in the infected mediastinal environment, and the elapsed time since the initial problem, and since the leak was well-drained and clinically tolerated, an endoprosthesis was placed. On endoscopy performed on 03/02/2022, a large defect in the esophageal wall covering 70% of the circumference was observed at 34 cm from the dental arch (gastric folds were at 37 cm). A self-expanding metallic WallFlex esophageal prosthesis coated with 105 x 23 mm was placed, anchored proximally with two endoscopic stitches using the OverStich system. The patient was discharged on 18/02/2022 under home hospitalization. The last prosthesis removal on 02/06/2022, after four replacements every four weeks, revealed an elevated mucosal patch replacing the previously described defect. Fluoroscopy confirmed the absence of leakage, and contrast-enhanced oral and intravenous CT showed no complications. The patient resumed a soft diet before hospital discharge. Currently, the patient is asymptomatic from a digestive perspective, with an esophagogastroduodenal transit performed on 27/09/2022 showing no contrast leakage.
Discussion
Esophageal perforation poses both diagnostic and therapeutic challenges due to its variable presentation and rarity. The surgical management of this condition relies mainly on small retrospective studies and expert opinions [11].
Several basic principles must be applied to the management of a patient with esophageal perforation:
• Early diagnosis.
• Hemodynamic monitoring and support.
• Early antibiotic therapy.
• Restoration of luminal integrity when feasible.
• Control of extraluminal contamination.
Primary surgical repair is performed when an experienced surgeon believes the perforation can heal, considering various factors such as [12]:
• Factors related to the perforation itself, including etiology, location, and severity.
• Time elapsed from symptom onset to treatment application.
• Patient-related factors: age, performance status (ECOG), comorbidities, presence of concomitant known esophageal injury.
• Clinical impact and involvement of surrounding tissues.
Surgical management of esophageal perforation includes various approaches, but there are general principles for performing primary repair, including debridement of devitalized tissue at the perforation site, incision of the upper and lower muscle fibers to expose the entire extent of the injured mucosa, and precise edge reapproximation to prevent subsequent stenosis.
If there has been a diagnostic or therapeutic delay of more than 24 hours or substantial extraluminal contamination, primary repair is usually not a good option [13]. In this scenario, the use of a vascularized pedicled flap surgically can improve results.
Traditionally, esophageal stents were used for palliative treatment of dysphagia in patients with cancer. With the advent of covered stents, their use in esophageal perforations has expanded, and patient selection for this therapeutic approach remains controversial [14].
Several case series published since 2007 support the use of esophageal stents in esophageal perforations as an optimal therapeutic option when patient selection is correct. Kiev et al. [15] reported 14 consecutive cases of intrathoracic esophageal perforations of different etiologies treated with a covered PolyFlex prosthesis, achieving functional closure without evidence of leakage in 78% with no mortality. Freeman et al. [16] reported 17 cases of iatrogenic esophageal perforations during endoscopic procedures with good results. The two longest and most recent case series are from two German groups. In one study [17], endoprostheses were used in 32 patients with intrathoracic esophageal perforation or intrathoracic anastomotic leak after gastrectomy or esophagectomy, achieving functional closure in 78% with a mortality of 15.6% (n=5), limited to oncological patients with advanced disease where therapeutic measures were restricted. The second study [18] described a series of 31 cases of iatrogenic perforations during endoscopic procedures, achieving complete coverage of esophageal perforations with self-expanding metallic prostheses in 92%, with complications limited to prosthesis migration in one case.
In 2011, D’Cunha et al. [19] published inclusion and exclusion criteria for patients eligible for endoscopic treatment of esophageal perforation. Inclusion criteria include intrathoracic esophageal perforations, benign etiologies (iatrogenic, Boerhaave syndrome, undilated achalasia), and malignancies only as a palliative measure in non-surgical candidates. Exclusion criteria consist of perforations within 2 cm of the cricopharyngeal muscle, perforated cancers (considering prosthesis only in purely palliative patients), and patients with a motor disorder causing esophageal dilation (diameter >3 cm) due to a high probability of prosthesis migration.
Therefore, the use of endoprostheses should be considered a therapeutic option for restoring luminal integrity after esophageal perforation when primary repair is not feasible [20]. While adhering to basic principles of use is essential, each case should be individualized to achieve the best possible results. In some instances, a sole endoscopic approach is not possible, necessitating additional surgical intervention for mediastinal drainage, devitalized tissue debridement, and concurrent feeding jejunostomy [21]. This combined approach can help avoid esophageal resection and diversion surgery, with its associated morbidity and mortality, allowing preservation of the intact esophagus in benign pathology.
Conclusion
Esophageal perforation poses both diagnostic and therapeutic challenges due to its variability in presentation and low frequency. Surgical management is based on fundamental principles, emphasizing the importance of early diagnosis, hemodynamic monitoring, antibiotic therapy, and restoration of luminal integrity. The decision for primary surgical repair depends on various factors, including the etiology of the perforation, time elapsed since symptoms, and the patient’s condition. The effectiveness of esophageal stents is highlighted in certain cases, especially when primary repair is not feasible, underscoring the importance of careful patient selection. This approach, combined in some cases with additional surgical interventions, may be crucial in avoiding esophageal resections and preserving esophageal integrity in benign pathologies.
References
- Cooke DT, Lau CL. Primary repair of esophageal perforation. Operative Techniques in Thoracic and Cardiovascular Surgery. 2008; 13: 126.
- Merchea A, Cullinane DC, Sawyer MD, et al. Esophagogastroduodenoscopy-associated gastrointestinal perforations: A singlecenter experience. Surgery. 2010; 148: 876.
- Kavic SM, Basson MD. Complications of endoscopy. Am J Surg. 2001; 181: 319.
- Brinster CJ, Singhal S, Lee L, et al. Evolving options in the management of esophageal perforation. Ann Thorac Surg. 2004; 77: 1475.
- Curci JJ, Horman MJ. Boerhaave’s syndrome: The importance of early diagnosis and treatment. Ann Surg. 1976; 183: 401.
- de Schipper JP, Pull ter Gunne AF, Oostvogel HJ, van Laarhoven CJ. Spontaneous rupture of the oesophagus: Boerhaave’s syndrome in 2008. Literature review and treatment algorithm. Dig Surg. 2009; 26: 1.
- Vallböhmer D, Hölscher AH, Hölscher M, et al. Options in the management of esophageal perforation: analysis over a 12-year period. Dis Esophagus. 2010; 23: 185.
- Shaker H, Elsayed H, Whittle I, et al. The influence of the golden 24-h rule on the prognosis of oesophageal perforation in the modern era. Eur J Cardiothorac Surg. 2010; 38: 216.
- Salo JA, Isolauri JO, Heikkilä LJ, et al. Management of delayed esophageal perforation with mediastinal sepsis. Esophagectomy or primary repair? J Thorac Cardiovasc Surg. 1993; 106: 1088.
- Kim-Deobald J, Kozarek RA. Esophageal perforation: An 8-year review of a multispecialty clinic’s experience. Am J Gastroenterol. 1992; 87: 1112.
- Clayton J Brinser BA, Sunil Singhal MD, Lawrence Lee BS, et al. Evolving options in the management of esophageal perforation. Ann Thorac Surg. 2008; 77: 1475-1483.
- White RK, Morris DM. Diagnosis and management of esophageal perforation. Ann Surg. 1992; 58: 112-119.
- Shaker H, Elsayed H, Whittle I, et al. The influence of the Golden 24-h rule on the prognosis of esophageal perforation in the modern era. Eur J Cardiothorac Surg. 2010; 38: 216.
- Sepsi B, Raymond DP, Peters JH. Esophageal perforation: surgical, endoscopic and medical management strategies. Current opinion in Gastroenterology. 2010; 26: 379-383.
- Kiev J, Amendola M, Bouhaidar D, et al. A management agorithm for esophageal perforation. Am J Surg. 2007; 194: 103-106.
- Freeman RK, Van Woerkom JM, Ascioti AJ. Esophageal stent placement for the treatment of iatrogenic intrathoracic esophageal perforation. Ann Thorac Surg. 2007; 83: 2003-2007.
- Salminen P, Gullichsen R, Laine S. Use of self-expandable metal stents for the treatment of esophageal perforations and anastomotic leaks. Surg Endosc. 2009; 23: 1526-1530.
- Leers JM, Vivaldi C, Schafer H, et al. Endoscopic therapy for esophageal perforation or anastomotic leak with a self-expandable metallic stent. Surg Endosc. 2009; 23: 2258-2262.
- D´Cunha J. Esophageal Stents for leaks and perforations. J Thorac Cardiovasc Surg. 2011; 142: 39-46.
- De Schipper JP, Pull ter Gunne AF, Oostvogel HJ, van Laarhoven CJ. Spontaneous ruptura of the esophagus: Boerhaave´s síndrome in 2008. Literature review and treatment algorithm. Dig Surg. 2009; 26: 1.
- Port JL, Kent MS, Korst RJ, et al. Thoracic esophageal perforations: A decade of experience. Ann Thorac Surg. 2003; 75: 1071-1074.
