
Open Access, Volume 10
Sustained response to immunotherapy in a renal collecting duct carcinoma: A glimmer of hope for an orphan tumor
Marta Martínez Cutillas1 ; Imanol Martínez Salas2 ; Ramón Aguado Noya1 ; Yago Garitaonaindía1 ; Alejandro González Sánchez1 ; Cesáreo Corbacho Cuevas3 ; Aranzazu González Del Alba1
1Medical Oncology Department, Puerta de Hierro Hospital, Majadahonda, Spain.
2Medical Oncology Department, Jiménez Díaz Foundation Hospital Madrid, Spain.
3Pathology Department, Puerta de Hierro Hospital, Majadahonda, Spain.
Marta Martínez Cutillas
Medical Oncology Department, Hospital Puerta de Hierro Majadahonda c/ Joaquin Rodrigo 1, Majadahonda, Madrid, Spain.
Tel: 0034-911-917-731;
Email: mmcutillas@salud.madrid.org
Received : May 14, 2024,
Accepted : June 06, 2024
Published : June 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Renal Collecting Duct Cell Carcinoma (RCDCC) is a distinctive and aggressive form of Renal Cell Carcinoma (RCC). To date, there is no defined therapeutic strategy, and the evidence for Immunotherapy (IT) is very limited. The latest advances in molecular biology are aimed at clarifying therapeutic targets to guide therapeutics in this orphan tumor.
Case report: We are presenting a case study of a 57-year-old Caucasian male diagnosed with stage IV renal collecting duct cell carcinoma. He received two lines of platinum based chemotherapy, with brain and bone progression requiring radiotherapy for local control. Given the limited options available, the decision was made to initiate treatment with immunotherapy, which resulted in an excellent, durable response.
Conclusion: RCDCC is a rare subtype of RCC with an aggressive course. Advances in molecular techniques have enabled us to gain a deeper understanding of its histogenesis and identify potential therapeutic targets. This treatment option could be a viable approach for treating this tumor.
Keywords: Pembrolizumab; Renal collecting duct cell carcinoma; Non-clear renal cell carcinoma; Orphan tumor.
Abbreviations: RCDCC: Renal Collecting Duct Cell Carcinoma; RCC: Renal Cell Carcinoma; IT: Immunotherapy; TKIs: Tyrosine Kinase Inhibitors; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; CK: Cytokeratin; PAX8: Paired-Box Gene 8; FH: Fumarate Hydratase; NGS: Next-Generation Sequencing; SETD2: SET Domain Containing 2; NF2: Type 2 Neurofibromatosis; PFS: Median Progression-Free Survival; OS: Overall Survival; CI: Confidence Interval; UCUT: Urothelial Carcinoma Of The Upper Urinary Tract; ORR: Objective Response Rate.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Cutillas MM (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Cutillas MM, Salas IM, Noya RA, Garitaonaindía Y, Sánchez AG, Cuevas CC, Del Alba AG. Sustained response to immunotherapy in a renal collecting duct carcinoma: A glimmer of hope for an orphan tumor. Open J Clin Med Case Rep. 2024; 2252.
Introduction
RCDCC is an atypical and aggressive variant of renal cell carcinoma. It originates from the cells of the renal collecting duct and represents approximately 1% of all renal tumors. The average age of presentation is 60 years, with a higher prevalence in males than in females. This is an aggressive tumor with a significantly higher cancer-specific mortality compared to other renal cancer subtypes (HR 1.6, p<0.01) [1]. Up to 70.7% of patients are diagnosed at an advanced stage, with an estimated median survival of approximately 13.2 months (95% CI 11.0 to 15.5) [2].
Due to the rarity of this tumor, there is currently no protocolized therapeutic management. Historically, platinum-based chemotherapy has been the most used treatment due to its similarity to urinary tract cancer and its aggressive course. Other alternatives that have been widely developed in RCC, such as Tyrosine Kinase Inhibitors (TKIs) (temsirolimus, sorafenib, pazopanib), have demonstrated poor and short-lived response rates in the subset of patients with RCDCC [3,4]. The evidence for immunotherapy in this tumor is limited, and the data available are based on isolated cases.
We present a case of a man with metastatic RCDCC in prolonged response to Immunotherapy (IT) to review the molecular classification of this tumor, its immunogenic profile, and to share the benefit obtained. This will promote research and benefit other patients.
Clinical Case
A 57-year-old white male, active smoker, presented in October 2021 with constitutional symptoms and back pain of 2 months’ duration.
A Computed Tomography (CT) scan was ordered, which showed a 3 cm solid lesion in the left lower renal pole (Figure 1), multiple bony blasts at the dorsal, lumbar, and sacral levels, and a left adrenal lesion suggestive of metastasis (Figure 2). A brain Magnetic Resonance Imaging (MRI) was performed to complete the study and showed a right frontal lesion suggestive of metastasis.
The biopsy of the left renal lesion revealed the presence of renal parenchymal casts with infiltration by an epithelial neoplasm with infiltrative growth, prominent nucleoli, and abundant mitotic figures. Additionally, a desmoplastic stromal reaction was observed. Immunohistochemistry demonstrated positivity for Cytokeratin (CK) 7 Vimentin, SMARCB1, while Paired-Box Gene 8 (PAX8) and CK20 were negative. The expression of SMARCB1 and the absence of a clinical history of sickle cell trait or other sickle hemoglobinopathies indicate that a SMARCB1-deficient medullary carcinoma is unlikely. While neither 2-succinocysteine/2SC nor Fumarate Hydratase (FH) expression can be used to rule out a mutation of the fumarate hydratase gene associated with renal carcinoma and hereditary leiomyomatosis, the expression of CK7 and the lack of racemase expression, along with the absence of clinical mention of leiomyomas in other locations, are inconsistent with this possible diagnosis. The most compatible histological diagnosis with all the findings described was RCDCC. A traumatology evaluation was requested to confirm metastatic disease by biopsy of a vertebral lesion in L1. The pathologist’s report showed nests of atypical epithelial cells compatible with metastasis of renal origin. Next-Generation Sequencing (NGS) in the primary biopsy was requested with detection of mutations in SET domain containing 2 (SETD2) and Type 2 Neurofibromatosis (NF2).
The patient started treatment in December 2021 with cisplatin 75 mg/m2 (D1) + gemcitabine 1000 mg/m2 (D1 and D8) every 21 days, completing 6 cycles in July 2021. At this time, cerebral progression was observed with the appearance of two new lesions, in the left frontal region and in the right cerebellar hemisphere, as well as growth of the left adrenal lesion. In addition, there was the impression of clinical bone progression, as the patient presented an increase in dorsal pain. A treatment of D3 and D10-L1 antalgic RT and radiosurgery on the new brain lesions was proposed, and in August 2022 he started second-line treatment with carboplatin AUC 4 / etopide 100 mg/m2 days 1-3 every 21 days. After 3 cycles, she presented progression of the left frontal brain lesion, and it was decided to treat with RT and start a new line of treatment with IT.
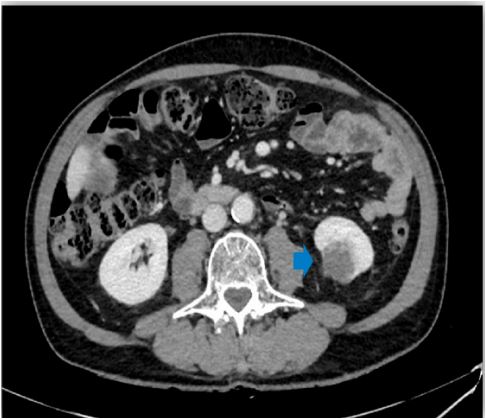
Figure 1: CT image, a 3 cm solid lesion in the left lower renal pole.

Figure 2: MRI image, dorsal vertebral metastases.
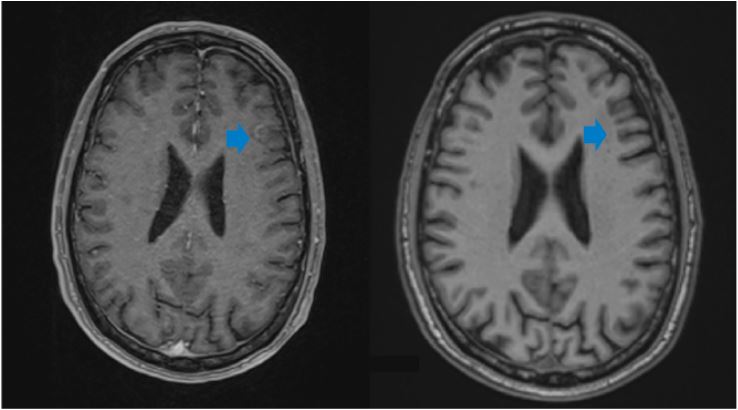
Figure 3: MRI image: Response to treatment of the left frontal lesion, baseline study October 2021 on
the left and after radiotherapy and IT treatment on the right in December 2023.
In October 2022, he started treatment with pembrolizumab 200 mg every 21 days, with stabilization of the disease at the first radiological re-evaluation. To date, he has completed 15 cycles with excellent tolerability and no relevant side effects, and analgesics have been discontinued. The patient was last evaluated in December 2023 and is in systemic and cerebral response (Figure 3).
Discussion
RCDCC is derived from duct cells, which has led to a correlation with urothelial carcinoma of the Upper Urinary Tract (UCUT). Consequently, the treatment of advanced RCDCC has been based on platinum based chemotherapy [5]. The GETUG group provided the strongest evidence that the platinum doublet is an active regimen in patients with RCDCC. In a prospective phase II study conducted by Oudard et al. [6] on 23 patients with RCDCC, the combination of platinum and gemcitabine demonstrated an objective response rate (ORR) of 26% (95% CI 8-44). The median Progression-Free Survival (PFS) and Overall Survival (OS) were 7.1 months (95% CI 3-11.3) and 10.5 months (95% CI 3.8-17.1), respectively.
The development of TKIs in the treatment of clear cell renal cell carcinoma has encouraged their investigation in other types of RCC with poorer prognosis, including RCDCC. In a phase II study of 26 patients with RCDCC, Sheng et al. [7] demonstrated that the combination of platinum-based chemotherapy and sorafenib followed by sorafenib maintenance was an effective and safe treatment strategy for this group of patients. The objective response rate was 30.8%, with a PFS and OS of 8.8 months (95% Confidence Interval [CI] 6.7-10.9) and 12.5 months (95% CI 9.6-15.4), respectively.
However, the implementation of MS techniques has shown that the overexpression of genes present in UCUT, such as GATA3 or TP63, is under expressed in RCDCC. These findings reinforce RCDCC as a unique and distinct entity from UCUT and encourage the search for specific alterations to better inform the development of targeted therapeutics. Among the most frequently identified genomic alterations in RCDCC are NF2 (29%) and SETD2 (24%), both present in the patient described above. The presence of these alterations may indicate that mTOR inhibition may be an attractive option for patients with RCDCC and NF2 mutations. Other potential avenues for investigation include histone deacetylase inhibition, EZH2 inhibition, antiangiogenic therapies, and CDK4/6 inhibition.
The use of IT has revolutionized the treatment of RCC and urothelial tumors. However, the evidence in RCC is limited. Some studies indicate that there is an overexpression of immune response genes related to T lymphocyte activation and proliferation, as well as a microenvironment enriched with tumor-infiltrating T lymphocytes and high expression of PD-L1 in RCDCC [8,9]. This theoretical framework could guide IT as an attractive therapeutic strategy in these patients. However, to date, data on the efficacy of checkpoint inhibitors in RCDCC are based on isolated cases published in the literature. In 2016, Rimar et al. published the first case of an objective response to nivolumab treatment in a patient with RCDCC after progression to chemotherapy and treatment with a TKI (pazopanib). One year later (2017), Mizutani et al. [11] published another case of RCDCC in response to nivolumab after failure of platinum doublet and temsirolimus.
PD-L1 expression was found to be significantly elevated in the patient’s histologic specimens, both in primary and metastatic disease. Subsequently, in 2018, Yasuoka et al. [12] published a similar case of a patient with metastatic RCDCC with an excellent response to nivolumab and early clinical improvement after progression to a first line of cisplatin-gemcitabine, refractoriness to a second line based on axitinib, and progression to a third line with carboplatin and paclitaxel. The immunohistochemical study of the primary tumor also demonstrated high expression of PD-L1.
A deeper understanding of the biology of this tumor is essential to improve the prognosis of these patients. Given its low incidence, the most effective strategy to expand knowledge of this pathology is a multi-institutional effort.
Conclusion
RCDCC is a rare subtype of non-clear cell renal carcinoma with an aggressive course. The application of more sophisticated molecular techniques has enabled us to gain a deeper insight into the disease’s origin and identify potential avenues for therapeutic intervention. This treatment option could be aviable approach for the management of metastatic RCDC.
References
- Suarez C, Marmolejo D, Valdivia A, Morales-Barrera R, Gonzalez M, et al. Update in collecting duct carcinoma: Current aspects of the clinical and molecular characterization of an orphan disease. Front Oncol. 2022; 12: 970199.
- Sui W, Matulay JT, Robins DJ, James MB, Onyeji IC, et al. Collecting duct carcinoma of the kidney: Disease characteristics and treatment outcomes from the National Cancer Database. Urol Oncol. 2017; 35(9): 540.e13-540.e18.
- Milowsky MI, Rosmarin A, Tickoo SK, Papanicolaou N, Nanus DM. Active chemotherapy for collecting duct carcinoma of the kidney: a case report and review of the literature. Cancer.2002; 94(1): 111-6.
- Procopio G, Testa I, Iacovelli R, Grassi P, Verzoni E, et al. Treatment of collecting duct carcinoma: current status and future perspectives. Anticancer Res. 2014; 34(2): 1027-30.
- Vanderbruggen W, Claessens M, De Coninck V, Duchateau A, Gevaert T, et al. Collecting duct renal cell carcinoma: A single centre series and review of the literature. Cent European J Urol.2022; 75(3): 252-6.
- Oudard S, Banu E, Vieillefond A, Fournier L, Priou F, et al. Groupe d’Etudes des tumeurs uro-génitales). prospective multicenter phase II study of gemcitabine plus platinum salt for metastatic.
- Sheng X, Cao D, Yuan J, Zhou F, Wei Q, et al. Sorafenib in combination with gemcitabine plus cisplatin chemotherapy in metastatic renal collecting duct carcinoma: A prospective, multicentre, single-arm, phase 2 study. Eur J Cancer. 2018; 100: 1-7.
- Malouf GG, Compérat E, Yao H, Mouawad R, Lindner V, et al. Unique transcriptomic profile of collecting duct carcinomas relative to Upper Tract urothelial carcinomas and other kidney carcinomas. Sci Rep. 2016; 6: 30988.
- Choueiri TK, Fay AP, Gray KP, Callea M, Ho TH, et al. PD-L1 expression in nonclear-cell renal cell carcinoma. Ann Oncol. 2014; 25(11): 2178-84.
- Rimar KJ, Meeks JJ, Kuzel TM. Anti-programmed death receptor 1 blockade induces clinical response in a patient with metastatic collecting duct carcinoma. Clin Genitourin Cancer. 2016; 14(4): e431-4.
- Mizutani K, Horie K, Nagai S, Tsuchiya T, Saigo C, et al. Response to nivolumab in metastatic collecting duct carcinoma expressing PD-L1: A case report. Mol Clin Oncol. 2017.
- Yasuoka S, Hamasaki T, Kuribayashi E, Nagasawa M, Kawaguchi T, et al. Nivolumab therapy for metastatic collecting duct carcinoma after nephrectomy: A case report: A case report. Medicine (Baltimore). 2018; 97(45): e13173.
