
Open Access, Volume 10
A case report of probable cortical basal ganglia degeneration misdiagnosed as Parkinson’s disease
Jing Li1*; Miao Yu2; Mengru Lu3
1Department of Neurology, Guangxi Medical University Cancer Hospital, Nanning, Guangxi, China.
2Department of Neurology, Weifang People’s Hospital, Weifang, Shandong, China.
3Department of Neurology, The Second Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, China.
Jing Li
Department of Neurology, Guangxi Medical University Cancer Hospital, Nanning, Guangxi, China.
Email: 12765990@qq.com
Received : May 02, 2024,
Accepted : May 28, 2024
Published : May 31, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Cortical Basal Ganglia Degeneration (CBD) is a relatively rare neurodegenerative change, because of the diversity of clinical features, it is easy to cause misdiagnosis.
Case report: In this paper, we report a case of probable corticobasal syndrome misdiagnosed as Parkinson’s disease and summarize CBDS clinically and radiologically in order to provide a basic understanding of CBDS to the majority of neurologists.
Conclusion: This study reports a case to further deepen our understanding of CBD. It also introduces the differentiation of Parkinson’s disease and reduces misdiagnosis.
Keywords: Cortico basal degeneration; Brady kinesia; Cortical dysfunction; Parkinson’s disease; Misdiagnosis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Li J (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Li J, Yu M, Lu M. A case report of probable cortical basal ganglia degeneration misdiagnosed as Parkinson’s disease. Open J Clin Med Case Rep. 2024; 2249.
Introduction
Cortical Basal Ganglia Degeneration (CBD) is currently considered to be a rare neurodegenerative disease characterized by pathological tau deposition, neuronal loss, ballooning, and glial degeneration in atrophic cerebral cortex and subcortical regions (including the substantia nigra and striatum) [1]. On CBD magnetic resonance, the majority showed asymmetric cortical atrophy in the frontal, temporal, and parietal lobes of the brain. Typical MRI findings are asymmetric cortical atrophy in the premotor area, supplementary motor area and posterior cingulate gyrus, and middle frontal lobe [2]. In this paper, we report a case of CBD misdiagnosed as Parkinson’s disease to summarize its clinical manifestations and imaging features, and have some experience in encountering such diseases in the future.
Case Report
The patient, a 75-year-old male, was admitted due to «stiffness of the left upper limb and slow movement for four years». Four years ago, the patient complained of stiff left shoelaces and slow movement without falling. The symptoms aggravated gradually and flexibility decreased steadily. In November 2020, the patient visited a local hospital and was diagnosed with «Parkinson’s disease». When the patient took Madopar, he felt a certain but subtle effect. Since then, the patient had been undergoing treatment for «Parkinson’s disease». In the recent one year, he experienced a muscle tension disorder of left upper limb. However, since the onset of the disease, the patient had no hyposmia, no dream-enacting behavior, conscious memory loss, no orthostatic dizziness, no hallucinations, auditory hallucinations or other phenomena, no urinary incontinence, fecal constipation, normal sleep, and no significant weight loss. The patient had a 5-year history of hypertension, with a maximum blood pressure of 180/105 mmHg. He took Amlodipine Tablets 5 mg on a regular basis and had fair blood pressure control. Additional medical history was unremarkable. The patient denied having similar medical history in the family. Nervous system: Normal vital signs, NEWS1 score, clear mind, answering the questions correctly, normal upper and lower vision, cranial nerve examination (-), soft neck, no resistance, normal muscle strength and increased muscle tension of the left upper limb, normal muscle tension of the left lower limb, left limb muscle tension disorder, left hand apraxia, normal muscle tension and muscle strength of the right side, less stable left finger-nose test, clumsy rapid rotation movement of the left side, normal heel-shin test, left cortical sensory disturbance, left limb, pathological signs (-). Anti-glomerular basal ganglia antibody (-), T-Sport (-), ENA antibody spectrum (-), double-stranded DNA quantification, glycosylated hemoglobin was normal, urination, HIV, RPR, TPPA, vitamin B12, folic acid, hepatitis virus screening (-), anticardiolipin antibody (-), coagulation, euthyroidism, infectious disease screening, tumor markers, calcitonin and antinuclear antibodies, blood routine, liver and kidney function, electrolytes, myocardial enzyme spectrum, ceruloplasmin were all normal, and blood lipid panel was not significantly abnormal. No Tau protein-related gene mutation. Magnetic resonance imaging: (Figure1A-E). Residual urine 26 ml, standing decubitus pulse pressure difference <10 mmHg, MMSE 24 points (university education level), MoCA 20 points, UPDRS III part 36 points, no anxiety and depression state. The PET-CT results revealed that the patient had FDG hypometabolism in the right precentral gyrus and hypometabolism in the left cerebellum. There was abnormal deposition of tau in striatum, thalamus, midbrain and pons, and parietal cortex. He also had decreased DaT (Dopamine Transporter) in the right anterior and posterior putame.
Diagnosis
Cortical Basal Ganglia Degeneration (CBD), the diagnosis of CBD disease, is generally considered the gold standard for pathological diagnosis, but because cases cannot be taken owing to limited conditions, it is deemed to be probable CBD according to the current diagnostic criteria for CBD in China [3-6].
Treatment and follow-up
After admission, the patient was given Madopar 0.25 g po tid, Vitamin B6 10 mg po tid, and Selegiline 1 mg po at noon of 1 morning. Madopar was noted to be 1.5 hours apart from the diet. During follow-up after 1 month, the symptoms were slightly improved than before.
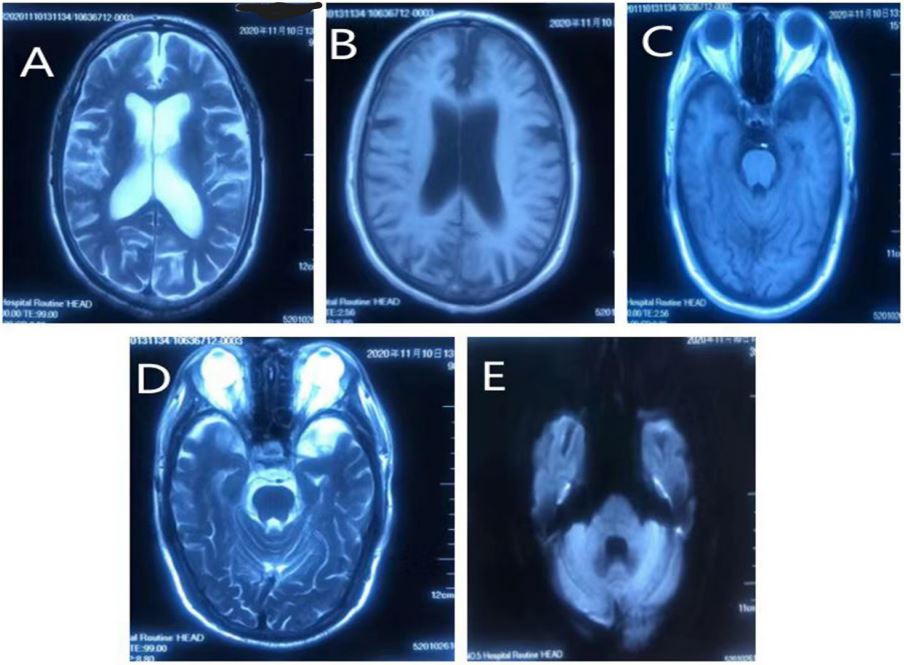
Figure 1: (A)MRI T2 (B) MRI T1 (C) MRI T1 (D) MRI T2 (E) MRI DWI
Figure 1A-E shows that the right brain atrophy is more significant than the left.
Availability of data and materials.
Discussion
Clinical presentation of CBD is characterized by different combinations of motor symptoms, some of which are associated with higher cortical lesions. It is mainly characterized by Parkinson-like symptoms combined with dystonia and myoclonus. Levodopa is ineffective in most patients and, in very few cases, mild to moderate remission may occur after levodopa therapy. However, remission occurs for a short time, and the after-effect is poor. Higher cortical symptoms are mainly changes such as conceptual apraxia, aphasia, cortical sensory disturbances, cognitive dysfunction, visuospatial disturbances, foreign limbs, and frozen gait [7,4]. Therefore, it is easily misdiagnosed as Parkinson’s disease in the early stages. Positron Emission Tomography (PET) examination showed that glucose metabolism (FDG) was low in the frontal lobe (including superior frontal gyrus, middle frontal gyrus, inferior frontal gyrus, and precentral gyrus), parietal lobe (including superior parietal lobule, parietal lobule, angular gyrus, supramarginal gyrus, and precuneus), occipital lobe (middle occipital gyrus), temporal lobe (including middle temporal gyrus, inferior temporal gyrus, transverse temporal gyrus, and shuttle gyrus), insula, and thalamus of the severely affected limb in CBD patients. On the contrary, glucose metabolism (FDG) was relatively high in the ipsilateral precentral gyrus, postcentral gyrus, hippocampus, insula, putamen, cerebellum, paracentral lobule, and pons. Dopamine Transporter (DAT) imaging can reveal reduced DaT in the asymmetric cortex and basal ganglia of CBD patients [8,5]. PET-tau imaging can detect Tau deposition in the cortex and basal ganglia of CBD patients [9,6]. The PET-CT in our patient revealed FDG hypometabolism in the right precentral gyrus and the left cerebellum, which is in line with the aforementioned reports. Furthermore, the abnormal tau deposition in striatum, thalamus, midbrain, and pons, as well as in the parietal cortex was consistent with previous findings. In addition, the reported DaT metabolism in this case was very characteristic, with DaT decreased in the anterior and posterior parts of the right putamen. Therefore, a probable CBD diagnosis was considered in this case. There is no effective treatment, and the average survival years of CBD has been reported to be 5-7 years [10,7], based primarily on symptomatic treatment. However, certain CBD patients can respond effectively to levodopa, and those who do not respond to levodopa can be treated with an increased dose of compound levodopa of 1.0 g/d, which can be discontinued after two months if no significant improvement is noted [4,8]. Botulinum toxin administered intramuscularly alleviates muscle tension disorders [5,9]. Recently, it has been shown that repetitive transcranial magnetic stimulation may improve the quality of life of CBD patients [10].
Conclusion
In clinical work, if motor disorders develop in unilateral limbs and last for more than three years, patients with severe limb asymmetry must be examined for cortex function, such as the presence or absence of apraxia, foreign limbs, and cortical compound sensory disorders. Patients with CBD are easily misdiagnosed as having PD in the early stages. Therefore, more meticulous inquiry and differential diagnosis involving the combined CBD and PD diagnostic criteria are required. If conditions permit, PET-CT is a feasible option for further differentiation.
Declarations
Availability of data and materials: The datasets used during the present study are available from the corresponding author on reasonable request.
Authors’ contributions: JL and YU designed the study and wrote the manuscript. MRL contributed to the manuscript revision. JL and YU contributed to the collection of clinical information.
Ethics approval: The Guangxi Medical University Review Board provided ethical approval for this study.
Patient consent for publication: The written consent to publish was obtained from the patient.
Declaration of interest’s statement: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Informed consent: Verbal informed consent was obtained from all subjects before the study.
Additional information: No additional information is available for this paper.
References
- Saranza GM, Whitwell JL, Kovacs GG, Lang AE. Corticobasal degeneration. Int Rev Neurobiol. 2019; 149: 87-136.
- Armstrong MJ. Diagnosis and treatment of corticobasal degeneration. Curr Treat Options Neurol. 2014; 16(3): 282.
- Constantinides VC, Paraskevas GP, Paraskevas PG, Stefanis L, Kapaki E. Corticobasal degeneration and corticobasal syndrome: A review. Clin Park Relat Disord. 2019; 1: 66-71.
- Mille E, Levin J, Brendel M, et al. Cerebral Glucose Metabolism and Dopaminergic Function in Patients with Corticobasal Syndrome. J Neuroimaging. 2017; 27(2): 255-261.
- Albrecht F, Bisenius S, Morales Schaack R, Neumann J, Schroeter ML. Disentangling the neural correlates of corticobasal syndrome and corticobasal degeneration with systematic and quantitative ALE meta-analyses[J]. npj Parkinson’s Disease, 2017, 3(1): 12.
- Lagarde J, Olivieri P, Caillé F, Gervais P, Baron JC, et al. [18F]-AV-1451 tau PET imaging in Alzheimer’s disease and suspected non-AD tauopathies using a late acquisition time window. J Neurol. 2019; 266(12): 3087-3097.
- Lamb R, Rohrer JD, Lees AJ, Morris HR. Progressive Supranuclear Palsy and Corticobasal Degeneration: Pathophysiology and Treatment Options[J]. Current Treatment Options in Neurology, 2016, 18(9): 42.
- Armstrong MJ. Diagnosis and treatment of corticobasal degeneration. Curr Treat Options Neurol. 2014; 16(3): 282.
- Morelet A, Gagneux-Lemoussu L, Brochot P, Ackah-Miezan S, Colmet-Daage JF, et al. Tonic dystonia: an uncommon complication of reflex sympathetic dystrophy syndrome. A review of five cases. Joint Bone Spine. 2005; 72(3): 260-262.
- Koga S, Josephs KA, Aiba I, Yoshida M, Dickson DW. Neuropathology and emerging biomarkers in corticobasal syndrome [published online ahead of print, 2022 Jun 13]. J Neurol Neurosurg Psychiatry. 2022; 93(9): 919-929.
