
Open Access, Volume 10
Hepatoid adenocarcinoma of the lung: New perspectives? A case report and review of the existing literature
Fabian Junker1 ; Fidelis A. Flockerzi2 ; Frank Langer1
1Department of Thoracic and Cardiovascular Surgery, Saarland University Medical Center, Homburg/Saar, Germany.
2Institute of Pathology, Saarland University Medical Center, Homburg, Saar, Germany.
Frank Langer
Department of Thoracic and Cardiovascular Surgery, Saarland University Medical Center, Kirrberger
Straße 100 66424 Homburg/Saar, Germany.
Email: frank.langer@uks.eu
Received : Apr 26, 2024,
Accepted : May 23, 2024
Published : May 31, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Hepatoid adenocarcinoma of the lung is a very rare primary malignancy of the lung which shows histopathological characteristics of hepatocellular carcinoma and is associated with a poor prognosis. Currently, there is no established treatment for hepatoid adenocarcinoma of the lung.
Case report: We report the case of a 66-year-old woman who presented with unspecific pulmonary symptoms and was later diagnosed with hepatoid adenocarcinoma of the lung. The patient was treated with a combination of different therapies including surgery, immunotherapy, chemotherapy and radiation therapy. The patient died 22 months after diagnosis and the following autopsy revealed several metastases. Death was caused by a combination of circulatory failure paired with respiratory insufficiency, pneumonia and multiple pulmonary embolisms.
Review: We created a virtual patient collective of 52 cases including our own. Analysis revealed male sex, smoking and advanced age as potential risk factors for hepatoid adenocarcinoma. Patients who were treated with a surgical approach survived longer than patients who received medically-based therapies.
Discussion: Hepatoid adenocarcinoma should be considered as a potential differential diagnostic for patients who initially present with unspecific symptoms and clinical signs of a progressed malignant pulmonary disease. The diagnostic process of hepatoid adenocarcinoma is quite heterogenous.
Therefore, a standardised histopathological examination should be established to avoid misdiagnosis. As the hepatoid adenocarcinoma of the lung is a rare entity, there is no established treatment so far.
Conclusion: The establishment of an international register for hepatoid adenocarcinoma of the lung could lead to earlier detection of this rare malignancy and could help to develop new treatment options.
Keywords: Hepatoid adenocarcinoma; Hepatoid adenocarcinoma of the lung; Primary malignancies of the lung; Rare malignancies; Thoracic oncology; Thoracic surgery.
Abbreviations: AFP: α-Fetoprotein; ALK: Anaplastic Lymphoma Kinase; CT: Computer Tomography/tomogram; CK7: Cytokeratin 7; EGFR: Epidermal Growth Factor Receptor; HepPar1: Hepatocyte-Paraffin 1; HAC: Hepatoid Adenocarcinoma; HAL: Hepatoid Adenocarcinoma of the Lung; HAS: Hepatoid Adenocarcinoma of the Stomach; Ki67: Kiel 67; NTRK: Neurotrophic Tyrosine Receptor Kinase; RET: Rearranged During Transfection; ROS1: ROS Protooncogene 1; TTF-1: Thyroid Transcription Factor-1; UICC/AJCC: Union for International Cancer Control/American Joint Committee on Cancer.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Langer F (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Junker F, Flockerzi FA, Langer F. Hepatoid adenocarcinoma of the lung: New perspectives? A case report and review of the existing literature. Open J Clin Med Case Rep. 2024; 2246.
Introduction/Background
Hepatoid Adenocarcinoma of the Lung (HAL) is a rare malignancy which presents morphologic features of hepatocellular carcinoma but is primarily located in the lung. However, clinical presentation of the patients is similar to patients suffering from more common subtypes of pulmonary adenocarcinoma. To detect HAL, elevated levels of Alpha-Fetoprotein (AFP) can be a potential diagnostic hint, but biopsy and histopathologic analysis remains the gold standard [1]. HAL was first described as its own entity by Ishikura et al. in 1990 [2]. Compared to other histopathologic subtypes of pulmonary adenocarcinomas, the incidence of HAL is very low. Despite the low number of cases worldwide, it seems that HAL shows a poorer prognosis compared to usual adenocarcinoma of the lung, but it still lacks an established therapeutic standard as well as reliable prognostic factors [3]. The pathogenesis of this tumour entity remains unknown [3]. There is a lack of empirical evidence as there is no official database for hepatoid adenocarcinoma, especially of the lung. Additionally, there is no established therapeutic standard for HAL and there are no validated prognostic factors for HAL [3,4].
For diagnosis, histopathological examination [4] including immunohistochemical analysis for Cytokeratin 7 (CK7), thyroid Transcription Factor-1 (TTF-1) and Hepatocyte-Paraffin 1 (HepPar1) is mandatory. Pulmonary metastasis of hepatocellular carcinoma must be ruled out using appropriate imaging modalities [5].
To our knowledge, we are presenting one of the few reported cases of HAL in Germany as this type of malignancy is mainly found in Asia [5,6].
Case Report
A 66-year-old Caucasian female ex-smoker, who was first diagnosed with HAL in December 2020, presented with a history of invasive lobular breast carcinoma in 1996 and was treated with breast conserving surgery as well as radiotherapy. The only other known comorbidity was arterial hypertension. She had a smoking history of 40 pack-years but stopped smoking in 2018. At that time, her presenting symptoms were a swelling of her left dorsal thoracic wall and a weight loss of 10 kg within 6 weeks. She initially presented to an orthopaedic clinic with excruciating pain and was referred to our university hospital for a possible sarcoma. The following diagnostic procedures revealed a tumour, suspicious of malignancy, in her left lung with an involvement of the adjacent thoracic wall. The necessary disease staging did not reveal any further tumours, especially, there was no indication of a potentially malignant liver lesion in her radiological examinations.
To differentiate between metastasis of previously known mamma carcinoma, a post-radiogenic malignancy caused by her previous treatment and primary lung cancer, a CT-guided biopsy was performed; the following histopathologic analysis confirmed non-small cell cancer without immunophenotype of breast carcinoma.
Supposing primary lung cancer, resection including the lingula and the left ventral thoracic as well as the dorsal thoracic tumour and the dorsal thoracic wall was performed. Although the malignancy had already progressed, the interdisciplinary tumour board made the decision for surgical resection with the goal of a palliative treatment and reduction of the patient’s pain. The decision was in accordance with German guidelines at that time as it was recommended to plan an individual approach for palliative care patients [7]. The surgical procedure was successful in relieving the patient’s symptoms and a complete in sano resection of the tumour was achieved. Histologic analysis revealed hepatoid morphology and positivity of the tumour cells for Hepar1 and CK7, leading to the diagnosis of HAL.
In summary, lung cancer stage group was IVa according to UICC/AJCC.
The patient received an adjuvant chemotherapy (carboplatin and paclinab) as well as immunotherapy (pembrolizumab) as a second line therapy. The adjuvant therapy was in accordance with German guidelines at that time [7]. She was diagnosed with stable disease in June 2021 and received a maintenance therapy (pembrolizumab) as well as radiotherapy of mediastinal lymph nodes as the surgical specimen showed indications of lymphatic metastasis.
The patient presented again in September 2021 due to a swelling next to the surgical site. CT scans confirmed disease progression in form of soft tissue metastasis of the anterior thoracic aperture as well as an increase in reactive change of the left interlobular fissure. In consequence of the progress, the patient received second line chemotherapy (docetaxel and nintedanib) [7]. The patient died 22 months after the first diagnosis. The following autopsy revealed metastasis in abdominal and cervical lymph nodes as well as bone metastasis (iliac crest) (Figure 1) resulting in malignancy-related toxic circulatory failure in combination with respiratory insufficiency, pneumonia and pulmonary embolisms (Figure 1).
Histology
Postoperative pathological examination confirmed advanced tumour stage (pT4, pN1) with lymphand hemangioinvasion. All resection margins were tumour-free. In histological analysis, tumour cells were arranged in nests and stripes, closely resembling hepatoid growth pattern (Figure 2A). The tumour cells showed anisonucleosis, enlarged nuclei and hyperchromasia (Figure 2A). Immunohistochemically, CK7- positive tumour cells were TTF1-negativ in nuclei but showed weak cytoplasmic staining of TTF1 (Figure 2B). 50-60% of the tumour cells were positive for Ki67. Interestingly, tumour cells were positive for Hepatocyte and they showed a weak positive staining for AFP (Figure 2E). NapsinA was negative. Less than 1% of tumour cells were positive for PDL-1. Molecular analysis showed no mutations in genes for BRAF, EGFR, KRAS, ALK, ROS1, RET and NTRK (Figure 2).
Additionally, tumour cells were positive for E-cadherin but negative for estrogen receptor and GATA3. Histopathological examination made a recurrence of the lobular mamma carcinoma unlikely.
Review of Literature
We conducted a review of the existing literature regarding hepatoid adenocarcinoma of the lung. Therefore, we searched PubMed (last updated 05/08/2023) using the keywords “hepatoid adenocarcinoma of the lung” and “hepatoid adenocarcinoma lung”. We filtered the results for free full text availability and articles in English language. We reviewed the literature and used it to create a virtual collective of patients. We excluded case reports from data bases that diagnosed the HAL in retrospect or that reported different locations of the hepatoid adenocarcinoma than the lung. Overall, we included 52 cases from which 51 have already been published as well as our own case. Furthermore, we restricted our analysis to survival analysis (Kaplan-Meier as imbedded in GraphPad Prism 8) and descriptive as well as analytic statistics using IBM SPSS statistics. We deemed the data unsuitable for further statistic tests as the data quality and availability was severely restricted in some cases.
The majority of cases (for cases see Table 1) were male patients (88.5%) whereas only 11.5% were female. Smoking status was only available in 44 cases, but the analysis showed that most of the patients (63.5%) had a smoking history. The patients age ranged from 26 to 78 years at the time of diagnosis, the median being 63 years (mean age was 60.35 years). There was no consistent report of any specific molecular markers like PDL-1 or EGFR. However, in 42.3% of all included cases an elevation of AFP in the patient’s serum was measured ranging from 1.0 ng/ml to a maximum of 97561.0 ng/ml with a median of 2473.5 ng/ ml. The average concentration of AFP was 10762.92 ng/ml.
For survival analysis only cases reporting time of survival as well as death or continued survival of the subject were included. Cases reporting survival were censored for the analysis and cases which did not report a therapy were excluded for the comparison of different therapies.
As Figure 3A shows, survival after diagnosis rapidly decreases with a median survival of only 15 months after diagnosis. After 24 months, only about 30% of all patients are still alive. Figure 3B shows the difference in the patient’s survival after exclusively surgical therapy (N=9) or a combined therapy of different therapeutic modalities including surgery or interventional, radiotherapy, chemotherapy, immunotherapy as well as targeted therapies (N=35) and therefore represents a rather heterogenous group. There is no significant difference between both groups (P value>0.05), however the median survival in the “surgery only” collective is 34 months whereas in the “combined therapies” collective the median survival is only 14 months after diagnosis.

Figure 1: Depiction of metastasis and primary tumour.
Right neck: cervical lymph node metastasis.
Chest: primary lesion is marked on both sides.
Abdomen: abdominal lymph node metastasis (pN3).
Pelvis: bone marrow metastasis in illiac crest (pM1b).
Right neck: cervical lymph node metastasis.
Chest: primary lesion is marked on both sides.
Abdomen: abdominal lymph node metastasis (pN3).
Pelvis: bone marrow metastasis in illiac crest (pM1b).

Figure 2: Histology of hepatoid adenocarcinoma of the lung. Magnification 200x. Scale bar 50 µm.
A) Nested structures of neoplastic cells with nuclear atypia in the lung mimicking hepatocellular carcinoma. Hematoxylin-Eosin (HE)-staining.
B) Neoplastic cells with weak cytoplasmatic staining of thyreoid transcription factor-1 (TTF1) (as it is seen in hepatocytes). In the right lower part, local pneumocytes show nuclear staining for TTF1. TTF1immunohistochemistry.
C) Neoplastic cells with cytoplasmatic staining of Hepatocyte. Hepatocyte-Paraffin 1 (HepPar1) immunohistochemistry.
D) Neoplastic cells with cytoplasmatic staining of cytokeratin (CK7). Cytokeratin7 immunohistochemistry.
E) Neoplastic cells with staining of alpha-fetoprotein (AFP). AFP-immunohistochemistry.
A) Nested structures of neoplastic cells with nuclear atypia in the lung mimicking hepatocellular carcinoma. Hematoxylin-Eosin (HE)-staining.
B) Neoplastic cells with weak cytoplasmatic staining of thyreoid transcription factor-1 (TTF1) (as it is seen in hepatocytes). In the right lower part, local pneumocytes show nuclear staining for TTF1. TTF1immunohistochemistry.
C) Neoplastic cells with cytoplasmatic staining of Hepatocyte. Hepatocyte-Paraffin 1 (HepPar1) immunohistochemistry.
D) Neoplastic cells with cytoplasmatic staining of cytokeratin (CK7). Cytokeratin7 immunohistochemistry.
E) Neoplastic cells with staining of alpha-fetoprotein (AFP). AFP-immunohistochemistry.
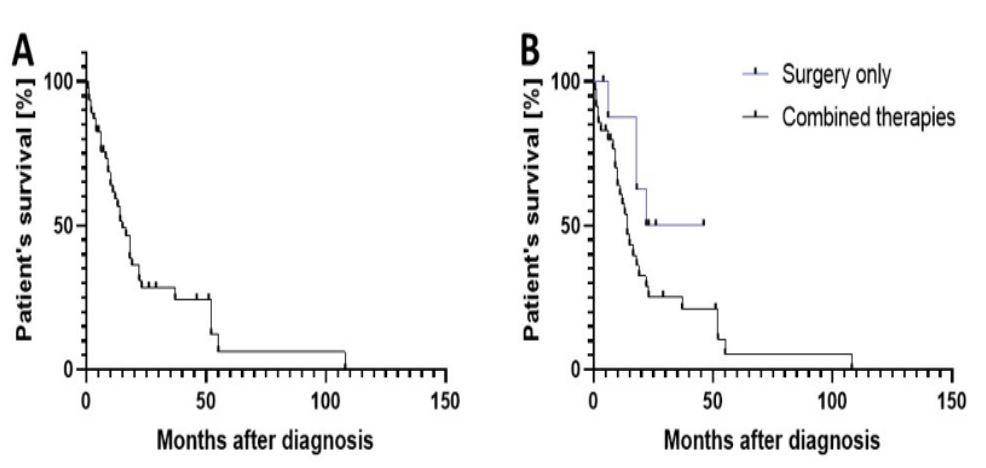
Figure 3: Patient survival
A) Overall survival of enclosed patients in relation to the time in months after diagnosis (N=47).
B) Survival compared between a “Surgery only” and “Combined therapies” group (N=44) .
A) Overall survival of enclosed patients in relation to the time in months after diagnosis (N=47).
B) Survival compared between a “Surgery only” and “Combined therapies” group (N=44) .
Table 1:Results of previous cases.
| Sex | Age [years] |
Smoking Status |
Staging | AFP [ng/ml] | Ki67 [%] | Treatment | Outcome | Survival [months] |
Reference |
|---|---|---|---|---|---|---|---|---|---|
| M | 51 | Y | IIIB | 1.3 | / | ST, RT, CT | D | 14 | 1 |
| M | 52 | Y | IV | / | / | ST, RT, CT | D | 37 | |
| M | 64 | Y | IV | 1 | / | ST, RT, CT | D | 10 | |
| M | 54 | Y | IV | / | / | RT, CT | D | 108 | |
| M | 60 | Y | IV | 4410 | / | RT, CT | D | 1 | |
| M | 61 | Y | IA | n | / | ST, RT | D | 6 | 2 |
| M | 47 | Y | IV | n | / | ST | D | 4 | 3 |
| M | 59 | Y | IB | n | 20 | ST | S | 23 | 4 |
| M | 53 | N | / | 3296 | 20 | ST, RT, CT, TT | S | 29 | 5 |
| M | 69 | / | IB | 4497 | / | ST, RT, CT | S | 51 | 6 |
| M | 64 | / | IV | 181 | / | RT, CT, TT, IT | D | 11 | 7 |
| F | 65 | N | IV | 6818 | / | RT, CT, TT | D | 52 | 8 |
| M | 43 | Y | / | / | / | RT, CT, IT | / | / | 9 |
| M | 70 | Y | IV | n | / | RT, CT, TT | D | 9 | 10 |
| M | 70 | Y | IIIA | n | / | ST | D | 18 | 11 |
| F | 62 | Y | IIIA | 9010 | / | ST, RT, CT, IT | D | 14 | 12 |
| M | 61 | / | IIIA | n | / | RT, CT | D | 55 | 13 |
| M | 54 | / | IV | n | / | RT, CT | D | 3 | 14 |
| M | 71 | Y | IIIC | 79480 | 80 | ST, RT, TT | D | 1 | 15 |
| M | 55 | Y | / | 1651 | / | CT, IT | D | 9 | 16 |
| M | 61 | Y | / | n | / | ST, IT | D | 22 | |
| M | 49 | N | / | 221 | / | / | / | / | |
| M | 67 | Y | / | n | / | / | D | 6 | |
| M | 70 | Y | / | / | / | / | / | / | 17 |
| M | 70 | Y | / | / | / | / | / | / | |
| M | 67 | Y | IIIB | n | / | ST, RT | D | 13 | 18 |
| M | 40 | Y | IIIB | 213 | / | CT | D | 23 | 19 |
| M | 74 | Y | IV | n | / | RT | D | 2 | |
| M | 52 | N | IV | n | / | CT | D | 8 | |
| M | 65 | Y | IV | n | / | CT | D | 0.5 | |
| M | 67 | Y | IV | / | / | / | / | / | |
| M | 26 | N | IV | 77.7 | / | CT | D | 2 | |
| M | 63 | / | / | / | / | / | D | 4 | 20 |
| M | 54 | Y | / | 13.7 | / | CT, IT | S | 4 | 21 |
| M | 55 | Y | IV | 9238 | 40 | CT, IT | S | 13 | 22 |
| F | 67 | N | / | / | / | CT, IT | D | 10 | 23 |
| F | 61 | / | / | / | / | ST, RT, CT | S | 5 | |
| M | 78 | Y | III | / | 60 | ST, IT | S | 5 | |
| M | 70 | Y | III | / | 30 | ST | D | 18 | 24 |
| M | 66 | Y | / | n | / | / | D | 0.5 | 25 |
| M | 63 | / | III | n | / | ST | D | 6 | 26 |
| M | 48 | Y | / | 6238 | / | RT, CT | D | 16.5 | 27 |
| M | 60 | / | II | 1210 | / | ST, CT | D | 15 | 28 |
| M | 66 | Y | / | / | / | ST | S | 46 | 29 |
| M | 64 | N | / | / | / | ST | S | 26 | |
| M | 64 | N | / | 20.15 | / | ST | S | 23 | |
| M | 63 | N | / | 8.32 | / | ST, CT | D | 18 | |
| M | 65 | Y | / | 5820 | 70 | ST, CT, IT | S | 12 | 30 |
| M | 41 | Y | II | / | 60 | RT | D | 12 | 31 |
| M | 66 | Y | IV | 97561 | / | CT | D | 19 | 32 |
| F | 65 | N | IV | 6818 | / | CT, IT | D | 52 | 33 |
| F | 66 | Y | IVA | / | 50-60 | ST, RT, CT, IT | D | 22 | Own case |
M: male, F: female, Y: smoker, N: non-smoker, n: reported as normal AFP, ST: surgical therapy, RT: radiotherapy, CT: chemother- apy, IT: immunotherapy, TT: targeted therapy, S: patient still alive at time of publication, D: patient deceased before publication, /: information not available because not reported in initial paper, patient lost to follow-up or patient declined treatment.
Discussion
The case we presented shows typical histopathological features of HAL including typical immunohistochemical phenotype (positivity for HepPar1, CK7 and AFP) [8]. A primary hepatocellular carcinoma was excluded using radiology (lifetime) and post mortem autopsy. The advanced tumour stage at the time of diagnosis as well as fast tumour progression are typical characteristic of HAL [4]. However, most patients present with unspecific symptoms at the time of diagnosis as seen in our case, so diagnosis of HAC should be standardised to avoid misdiagnosis [1,3]. The review of Li et al. might be a guide for future guidelines on histopathological diagnosis [1]. However, Agaimy et al. found different sets of molecular markers which are associated with hepatoid adenocarcinoma and TTF-1 negative adenocarcinomas in general. There is a need for further research to determine if the entity of non small cell lung cancer described by Agaimy et al. is a subtype of HAL or another type of a primary lung malignancy with a hepatic differentiation [6].
In accordance with the available data, we are suggesting that risk factors might be male sex as well as a history of smoking and age which are general risk factors for adenocarcinoma of the lung [1,9]. Therefore, we suggest that HAL should be considered as a possible differential diagnosis for patients in an advanced tumour stage at the time of diagnosis. In terms of treatment, a primarily surgical treatment might be superior to combined therapies for limited and locally progressed HAL when it comes to patient survival. A similar treatment is suggested in the current and in the previous German guideline for the treatment of pulmonary adenocarcinoma for patients in limited stages of their disease [7,10]. Similar to German guidelines for pulmonary adenocarcinoma, Li et al. found evidence that surgical treatment might be the best therapeutic approach in early stages of HAL and that the therapeutic success might be increased using an adjuvant therapy [1]. The fact that surgery is the preferred treatment option in early stages of the disease might explain why patients who were treated with surgery only had a better prognosis than patients with a combined therapeutic approach as the latter is the option for a progressed stage of disease. However, there is no conclusive evidence for targeted therapies or immunotherapies as a therapeutic option for hepatoid adenocarcinoma, but they might be a treatment option for patients in progressed stages of their disease, like chemotherapy and radiation therapy are today [1,11]. It should be noted that Hepatoid Adenocarcinoma of the Stomach (HAS) and HAL both have a rather poor prognosis and that therefore the prognosis does not depend on the specific subtype of hepatoid adenocarcinoma [1,11].
Current therapeutic approaches for HAL and HAS are similar and show similar results. Therefore, both subtypes might profit of a treatment which is focused on treating hepatoid adenocarcinoma rather than a treatment which is focussed on treating specific subtypes [1,11].
However, the heterogeneous quality of case reports or series describing HAL severely limits the possible extend of data extraction. Thus, it limits the quality of all conclusions that were determined using the data.
Conclusion
Therefore, we suggest the establishment of an international register for rare tumour entity to establish reliable tumour markers with the purpose of detecting tumours in earlier stages and to allow further molecular analysis to achieve new therapeutic approaches.
Declarations
Conflict of interest: None.
Funding: None.
Ethical treatment of patient: The patient consented to all medical procedures as well as to the use of her personal data for research purposes.
Acknowledgements: F.J. drafted and reviewed the manuscript and conducted the review, F.F. reviewed the manuscript and performed pathology, F.L. reviewed the manuscript and was the consulting clinician. All authors approved the final version of the manuscript for publication.
References
- Li M, Fan Y, Lu H. Hepatoid Adenocarcinoma of the Lung. Technol Cancer Res Treat SAGE Publications. 2021; 20.
- Ishikura H, Kanda M, Ito M, Nosaka K, Mizuno K. Hepatoid adenocarcinoma: A distinctive histological subtype of alpha-fetoprotein-producing lung carcinoma. Virchows Arch a Pathol Anat Histopathol Virchows Arch a Pathol Anat Histopathol. 1990; 417: 73-80.
- Chen Z, Ding C, Zhang T, He Y, Jiang G. Primary Hepatoid Adenocarcinoma of the Lung: A Systematic Literature Review. Onco Targets Ther Dove Press. 2022; 15: 609.
- Lei L, Yang L, Xu YY, Chen HF, Zhan P, et al. Hepatoid adenocarcinoma of the lung: An analysis of the Surveillance, Epidemiology, and End Results (SEER) database. Open Medicine De Gruyter. 2021; 16: 169.
- Mao J-X, Liu C, Zhao Y-Y, Ding G-S, Ma J-Q, Teng F, et al. Merged hepatopulmonary features in hepatoid adenocarcinoma of the lung: A systematic review. Am J Transl Res e-Century Publishing Corporation. 2021; 13: 898.
- Agaimy A, Fuchs F, Moskalev EA, Sirbu H, Hartmann A, et al. SMARCA4-deficient pulmonary adenocarcinoma: clinicopathological, immunohistochemical, and molecular characteristics of a novel aggressive neoplasm with a consistent TTF1neg/CK7pos/HepPar-1pos immunophenotype. Virchows Arch Virchows Arch. 2017; 471: 599-609.
- Ukena D, Schönfeld N. Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): Prävention, Diagnostik, Therapie und Nachsorge des Lungenkarzinoms, Lang- version 1.0, 2018. AWMF-Registernummer: 020/007OL. 2018.
- Yan J, Wei Q, Jian W, Liu J, Tang H, et al. A fine decision tree consisted of CK5/6, IMP3 and TTF1 for cytological diagnosis among reactive mesothelial cells, metastatic adenocarcinoma of lung and non-lung origin in pleural effusion. Int J Clin Exp Pathol eCentury Publishing Corporation. 2014; 7: 5810.
- Schabath MB, Cote ML. Cancer Progress and Priorities: Lung Cancer. Cancer Epidemiol Biomarkers Prev NIH Public Access. 2019; 28: 1563.
- Langer T. Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): Prävention, Diagnostik, Therapie und Nachsorge des Lungenkarzinoms, Kurzversion 2.1, 2022,. AWMF-Registernummer: 020-007OL. 2022.
- Xia R, Zhou Y, Wang Y, Yuan J, Ma X. Hepatoid Adenocarcinoma of the Stomach: Current Perspectives and New Developments. Front Oncol Frontiers Media SA. 2021; 11.
- Haninger DM, Kloecker GH, Bousamra M, Nowacki MR, Slone SP. Hepatoid adenocarcinoma of the lung: report of five cases and review of the literature. Mod Pathol. 2014; 27(4): 535-542. doi: 10.1038/MODPATHOL.2013.170.
- Ayub A, Nunez Lopez O, Booth A, Okereke I. Pulmonary hepatoid adenocarcinoma. J Thorac Cardiovasc Surg. 2019; 158(4): e139-e140. doi: 10.1016/J.JTCVS.2019.06.023
- Kuan K, Khader SN, El Hussein S. Hepatoid adenocarcinoma of the lung. Diagn Cytopathol. 2019; 47(8): 831-833. doi: 10.1002/DC.24195
- Sun JN, Zhang BL, Li LK, Yu HY, Wang B. Hepatoid adenocarcinoma of the lung without production of α-fetoprotein: A case report and review of the literature. Oncol Lett. 2016; 12(1): 189-194. doi: 10.3892/OL.2016.4559
- Chen H fei, Wang W xian, Li X liang, et al. Hepatoid Adenocarcinoma of the Lung with EGFR Mutation and the Response to Tyrosine Kinase Inhibitors. J Thorac Oncol. 2019; 14(10): e217-e219. doi: 10.1016/J.JTHO.2019.04.032
- Motooka Y, Yoshimoto K, Semba T, et al. Pulmonary hepatoid adenocarcinoma: report of a case. Surg Case Rep. 2016; 2(1). doi: 10.1186/S40792-0160129-6.
- Gavrancic T, Park YHA. A novel approach using sorafenib in alpha fetoprotein-producing hepatoid adenocarcinoma of the lung. J Natl Compr Canc Netw. 2015; 13(4): 387-391. doi: 10.6004/JNCCN.2015.0054
- Basse V, Schick U, Guéguen P, et al. A Mismatch Repair-Deficient Hepatoid Adenocarcinoma of the Lung Responding to Anti-PDL1 Durvalumab Therapy Despite no PD-L1 Expression. J Thorac Oncol. 2018; 13(7): e120-e122. doi: 10.1016/J.JTHO.2018.03.004
- Wang C, Xu G, Wu G, et al. Hepatoid Adenocarcinoma of The Lung Metastasizing to The Gingiva. Onco Targets Ther. 2019; 12: 8765-8768. doi: 10.2147/OTT.S222974
- Khozin S, Roth MJ, Rajan A, et al. Hepatoid carcinoma of the lung with anaplastic lymphoma kinase gene rearrangement. J Thorac Oncol. 2012; 7(11). doi: 10.1097/JTO.0B013E3182697A23
- Tonyali O, Gonullu O, Ozturk MA, Kosif A, Civi OG. Hepatoid adenocarcinoma of the lung and the review of the literature. J Oncol Pharm Pract. 2020; 26(6): 1505-1510. doi: 10.1177/1078155220903360
- Valle L, Thomas J, Kim C, et al. Hepatoid adenocarcinoma of the lung metastasizing to the tonsil. Mol Clin Oncol. 2017; 6(5):705-707. doi: 10.3892/MCO.2017.1215
- Grossman K, Beasley MB, Braman SS. Hepatoid adenocarcinoma of the lung: Review of a rare form of lung cancer. Respir Med. 2016; 119: 175-179. doi: 10.1016/J.RMED.2016.09.003
- Qian GQ, Yin FY, Li GX, Chu JG. Hepatoid adenocarcinoma of the lung. QJM. 2016; 109(9): 619-620. doi: 10.1093/QJMED/HCW107
- Li J, Qi H, Xu B, et al. Genomic Profiles of a Patient of Pulmonary Hepatoid Adenocarcinoma with High AFP Level: A Case Report. Front Oncol. 2019; 9. doi: 10.3389/FONC.2019.01360
- Zhuansun Y, Bian L, Zhao Z, et al. Clinical characteristics of Hepatoid adenocarcinoma of the lung: Four case reports and literature review. Cancer Treat Res Commun. 2021; 29. doi: 10.1016/J.CTARC.2021.100474
- Laraqui Houssein Y, Derqaoui S, Khouloud R, et al. Hepatoid Adenocarcinoma of the Lung: A Rare Form of Lung Cancer. Clin Pathol. 2022; 15. doi: 10.1177/2632010X221088961
- Chen Z, Ding C, Zhang T, He Y, Jiang G. Primary Hepatoid Adenocarcinoma of the Lung: A Systematic Literature Review. Onco Targets Ther. 2022; 15: 609627. doi: 10.2147/OTT.S364465
- Pasricha S, Grover S, Kamboj M, et al. Hepatoid adenocarcinoma of lung: A diagnostic challenge - Series of six cases with histopathological, predictive molecular and PD. L1 assessment. Indian J Pathol Microbiol. 2021; 64(1): 128-131. doi: 10.4103/IJPM.IJPM_334_20
- Chen JX, Lyu LL, Zhu WH, Chen XY, Zheng L. Hepatoid adenocarcinoma of the lung accompanied with multiple systemic metastases. Chin Med J (Engl). 2020; 134(2): 237-238. doi: 10.1097/CM9.0000000000000963
- Lagos GG, Feldman JL, Saqi A, Shu CA. Hepatoid Adenocarcinoma of the Lung Responsive to Frontline Combination Chemotherapy With Immunotherapy: Case Report. JTO Clin Res Rep. 2020; 2(2). doi: 10.1016/J.JTOCRR.2020.100130
- Xu SZ, Zhang XC, Jiang Q, Chen M, He MY, Shen P. Alpha-fetoprotein-producing hepatoid adenocarcinoma of the lung responsive to sorafenib after multiline treatment: A case report. World J Clin Cases. 2022; 10(28): 10236-10243. doi: 10.12998/WJCC.V10.I28.10236
- Bonis A, Dell’Amore A, Verzeletti V, et al. Hepatoid Adenocarcinoma of the Lung: A Review of the Most Updated Literature and a Presentation of Three Cases. J Clin Med. 2023; 12(4). doi: 10.3390/JCM12041411
- Yang K, Jiang H, Li Q. Primary pulmonary hepatoid adenocarcinoma: A case report and review of the literature. Medicine. 2019; 98(14). doi: 10.1097/MD.0000000000015053
- Cavalcante LB, Felipe-Silva A, Campos FPF de, Martines JA dos S. Hepatoid adenocarcinoma of the lung. Autops Case Rep. 2013; 3(1): 5-14. doi: 10.4322/ACR.2013.002.
- Yao Y, Guan X, Bao G, Liang J, Li T, Zhong X. Whole-exome sequencing and bioinformatics analysis of a case of non-alphafetoprotein-elevated lung hepatoid adenocarcinoma. Front Pharmacol. 2022; 13. doi: 10.3389/FPHAR.2022.945038
- Che YQ, Wang S, Luo Y, Wang JB, Wang LH. Hepatoid adenocarcinoma of the lung: Presenting mediastinal metastasis without transfer to the liver. Oncol Lett. 2014; 8(1): 105-110. doi: 10.3892/OL.2014.2064
- Shi YF, Lu JG, Yang QM, et al. Primary hepatoid adenocarcinoma of the lung in Yungui Plateau, China: A case report. World J Clin Cases. 2019; 7(13): 17111716. doi: 10.12998/WJCC.V7.I13.1711
- Sun H, Li X, Zhang J, Liu Y. Clinicopathological features and genomic profiles of hepatoid adenocarcinoma of the lung: Report of four cases. Pathol Res Pract. 2022; 229. doi: 10.1016/J.PRP.2021.153652
- Xu K, Gao J, Feng L, Fang Y, Tang X. A case report of pulmonary hepatoid adenocarcinoma: Promoting standardized diagnosis and treatment of the rare disease. Front Immunol. 2023; 14. doi: 10.3389/FIMMU.2023.1203876
- Wang W, Li G. Radiotherapy of Pulmonary Hepatoid Adenocarcinoma with Intrahepatic Hemangioma: A Case Report. Onco Targets Ther. 2020; 13: 1194711955. doi: 10.2147/OTT.S275340
- Muroyama Y, Tamiya H, Tanaka G, et al. Alpha-Fetoprotein-Producing Lung Hepatoid Adenocarcinoma with Brain Metastasis Treated with S-1. Case Rep Oncol. 2020; 13(3): 1552-1559. doi: 10.1159/000511763
- Chen L, Han X, Gao Y, et al. Anti-PD-1 Therapy Achieved Disease Control After Multiline Chemotherapy in Unresectable KRASPositive Hepatoid Lung
- Adenocarcinoma: A Case Report and Literature Review. Onco Targets Ther. 2020; 13: 4359-4364. doi: 10.2147/OTT.S248226.
