
Open Access, Volume 10
Total patellectomy in a dog: Long term outcome
Krystalli Androniki1*; Vorloka A1 ; Papaefthymiou SK1 ; Patsikas MN2 ; Prassinos NN1
1Surgery & Obstetrics Unit, Companion Animal Clinic, School of Veterinary Medicine, Faculty of Health Sciences, Aristotle University, Thessaloniki, Greece.
2Imaging and Diagnostic Laboratory, School of Veterinary Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, Greece.
Krystalli Androniki
School of Veterinary Medicine, Aristotle University of Thessaloniki, 11 St. Voutyra str. GR-54627 Thessaloniki, Greece.
Tel: +30-2310994499;
Email: andronikikr@yahoo.gr
Received : Apr 16, 2024,
Accepted : May 17, 2024
Published : May 20, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Patellectomy alters stifle biomechanics and has been demonstrated to result in degenerative joint lesions and to increase the force required for its extension. A 3-year-old male dog was admitted with right hindlimb lameness due to a penetrating wound in the stifle. After exploratory arthrotomy, diagnosis of straight patellar ligament avulsion and patellar fracture was established. In three months, the dog underwent three surgeries to repair the straight patellar ligament, drainage of the stifle, and total patellectomy. Antimicrobial and anti-inflammatory drugs were administered. Restriction of activity and physiotherapy were also advised. Patellectomy was performed because the patella was no longer adhered to its adjacent soft tissues and appeared to be necrotic. Follow-up information for seven years showed mild lameness in the affected limb and a body attempt to substitute the patella.
Keywords: Dog; Patella; Patellar ligament; Patellectomy; Stifle joint.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Androniki K (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Androniki K, Vorloka A, Papaefthymiou SK, Patsikas MN, Prassinos NN. Total patellectomy in a dog: Long term outcome. Open J Clin Med Case Rep. 2024; 2244.
Introduction
The patella is an ossification in the tendon of insertion of the quadriceps muscle group. It participates in the extensor mechanism of the stifle together with the quadriceps muscle group, trochlear groove, patellar ligament, and tibial tuberosity. Physiologic alignment of these structures, with normal gliding articulation of the patella and trochlea, are essential for smooth and efficient movement of the stifle during its extension [1].
The main indication for patellectomy is patellar fracture [2]. Total (TP) or Partial (PP) patellectomy should be considered if the fragment size or type preclude fixation. Fragments to be discarded are carefully excised with a scalpel or removed with rongeurs, avoiding where possible additional damage to the soft tissues. The extensor apparatus is obviously weakened in this area and will probably lengthen or fail if not protected. The area of TP is ‘snugged up’ with Bunnell type or mattress sutures. Where the most proximal fragment is preserved the soft tissues can be protected with a temporary wire prosthetic ligament. Further support may be provided by a strip of fascia lata, which remains attached proximal to the previous position of the patella, is reflected distally and is sutured to the peri patellar soft tissues and tibial crest [3].
The effect of TP or PP on the function of the stifle is a matter of controversy [2]. Removal of the patella consistently alters stifle biomechanics and has been demonstrated to result in degenerative joint lesions and to increase the force required for its extension [3,4]. In an experimental study in rabbits, early and severe arthritic changes were recorded in the femoral condyles after TP [5]. Also, in human literature, TP permanently decreases quadriceps muscle strength by one-third and reduces stifle stability [6]. Furthermore, in an experimental comparison between PP and TP, after the former, the alterations in the articular surface of the extensor apparatus and the articular cartilaginous surface of the patella and femoral condyles never equaled those noted in animals after TP; the abnormal alterations after PP are far less extensive [7]. However, poor detailed information regarding TP in dogs is available.
Case History
A 3-year-old male, crossbreed Collie, weighing 33 kg, was admitted with a right hind limb non weight bearing lameness. Twelve hours prior, the dog had fallen from a three m height, and a sharp wooden pole had penetrated his right stifle. The owner carefully removed the wooden pole, applied povidone-iodine (Betadine, Mundipharma AG, Switzerland, solution) on the wound, and administered amoxicillin (Amoxil, Glaxo Smith Kline, Greece, 30 mg/kg, per os, bolus). On orthopedic examination, the complaints of the owner were confirmed. The right stifle was painful on manipulation, and a penetrating wound in the craniolateral side of the joint was also observed. The patella was lying more proximally than normal, and the straight patellar ligament was not palpable. The results of complete blood count and routine serum biochemistry tests were normal, except WBCs which were scaled down. Radiographic examination of both stifles showed proximal displacement of the right patella and comminuted fracture of its distal pole (Figure 1). Diagnosis of straight patellar ligament rupture or avulsion and patellar fragmentation of the right limb was established, and exploratory stifle arthrotomy was performed.
After lateral arthrotomy, the stifle was thoroughly inspected and was copiously lavaged with warm normal saline. A focal erosion of the articular cartilage was observed on the lateral side of the lateral condyle. The distal pole of the patella was fractured into several pieces that were removed (Figure 1). The straight patellar ligament was avulsed from the patella, and two loops of orthopedic wire (1.2 mm) were used for its repair. Each loop was passed through a transverse drill hole in the tibial crest and then around the patella’s lateral, proximal, and medial side (first loop) or the proximal side of the patella and on its cranial surface in figure-of-eight configurations (second loop). In the proximal side of the patella, the wires were passed through the tendon of insertion of the quadriceps muscle. Also, before the tightening of the second wire loop, several horizontal mattress sutures (propylene 0) were placed between the proximal free end of the ligament and the soft tissues in the cranial surface of the patella (Figure 2). A Penrose tube was placed in the surgical site. Postoperatively, a combination of amoxicillin plus clavulanic acid (Synulox, Zoetis, Belgium, 20 mg/kg, BID, per os, for six days) and clindamycin (Zodon, Ceva, France, 10 mg/kg, BID, per os, for 3 weeks), and also a non-steroidal anti-inflammatory drug (Rimadyl, Zoetis, England, 2 mg/kg, BID, per os, for two weeks) was administered. The activity was strictly restricted for six weeks. An Elizabethan collar was applied until suture removal. The dog was not hospitalized due to his aggressive behavior. Unfortunately, the dog did not sustain the collar, and according to the owner, two days later, the Penrose tube was “totally” removed by the dog. Also, the restriction of the dog was impossible, therefore the right hindlimb bore weight during the first 15 days. Three weeks postoperative, the dog was readmitted with persistent nonweight-bearing lameness and swelling of the right stifle. A residual piece of the Penrose tube into the joint was suspected. Plain radiographs of the right stifle revealed mildly increased synovial mass, periarticular soft tissue swelling, and position of the patella proximal to both loops of wire (Figure 4). A second surgery was performed. A large amount of sanguineous fluid was accumulated subcutaneously. Both loose wire loops were removed, but the other sutures were intact, maintaining contact between the patella and the ligament. A piece of the Penrose tube was found and removed. The joint was copiously lavaged with warm normal saline. Postoperatively, the previous antimicrobial and non-steroidal anti-inflammatory drugs were administered for a month. Restriction and physiotherapy were also advised.
The dog was re-evaluated two months later. The owner said that stifle swelling had recurred many times, followed by drainage of sanguineous fluid from a sinus in the lateral side of the joint. The limb did not bear weight during stifle swelling but was sound after fluid drainage. The dog was otherwise healthy. A third surgery was performed. A large amount of sanguineous fluid was accumulated subcutaneously, and a sample was collected for culture and sensitivity tests before evacuation. The patella was deprived of its adhesions to the adjacent soft tissues and appeared to be necrotic, so it was removed. The continuity of the patellar ligament with the tendon of insertion of the quadriceps muscle was maintained. After culturing the fluid in blood Agar, MacConkey Agar, Mannitol Salt Agar, and Bile Esculin Agar, microorganisms of Corynebacterium species were isolated and identified. The inhibition zone diameter of enrofloxacin was 20 mm. Enrofloxacin (Baytril, Bayer Animal Health GmbH, Germany 5 mg/kg, SID, per os) and firocoxib (Previcox Boehringer Ingelheim Vetmedica GmbH, Germany, 5 mg/kg, SID, per os) for 30 days were administered. Restriction and physiotherapy were also advised. One month after the TP, the dog presented with weightbearing lameness (3/5) (Table 1) in the right hind limb. Swelling of the stifle had not recurred. Six months later, the gait was improved (lameness 2/5). Plain radiographs of the right stifle showed less severe osteoarthritic changes than the previous examination. Seven years after patella removal, the owner declared that he was satisfied with the outcome and that only a mild lameness was observed. In clinical examination, the right front leg showed lameness of second degree (2/5), and the right stifle was unable to fully bend and stretch. Radiographic and computed tomographic examination of the right stifle demonstrated soft tissue swelling, osteophyte and enthesophyte formation, ossification of the straight patellar ligament, and a well-defined 0.5×0.7 cm bony structure located at the position of the removed patella.
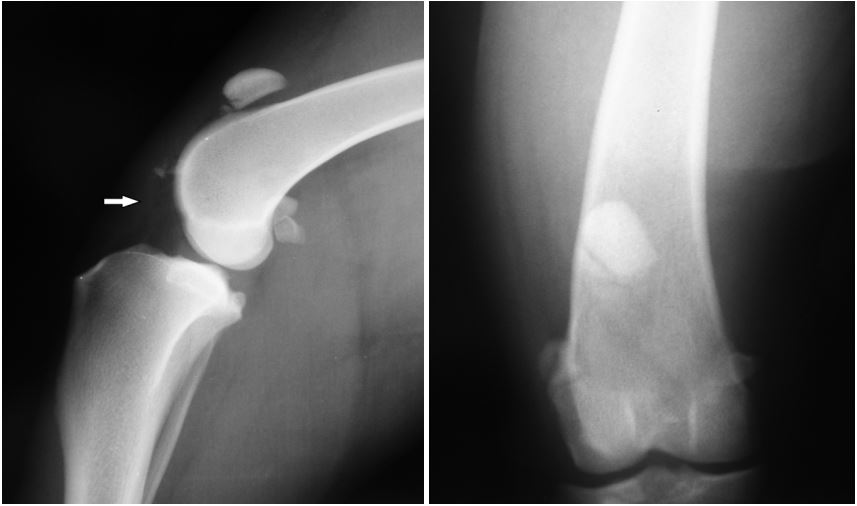
Figure 1: Lateral (A) radiograph of the right stifle showing proximal displacement of the patella, comminuted fracture of its distal pole and thickness of the straight patellar ligament (arrow). (B) Fragmented
bone pieces are located at the distal aspect of the displaced patella and cranially to the femoral trochlea.

Figure 2: Intraoperative photograph of comminuted fracture of the distal pole of the patella and crosssection of the patellar ligament.

Figure 3: Intraoperative photograph showing the suturing of the patellar ligament and placement of two metal
sutures to eliminate tension at the suture site.

Figure 4: Lateral (A) and craniocaudal (B) radiographs
of the right stifle after the use of two loops of orthopedic
wire for the repair of the avulsed straight patellar ligament. There is mildly increased synovial mass, periarticular soft tissue swelling and position of the patella proximal to both loops of wire.
Discussion
The patella is an essential component of the extensor mechanism, serving to alter the direction of the pull of the quadriceps mechanism, preserving even tension of the extensor mechanism during stifle extension, and acting as a lever arm, increasing the mechanical advantage of the quadriceps muscle group. The patella also protects the tendon of the quadriceps muscle group during movement, provides a greater surface area for the tendon to engage the trochlea of the femur, and provides cranial and rotary stability to the stifle joint in the extensor mechanism [8]. Due to above important functions of the patella, it is expected that after PP and especially TP, alter biomechanics of the stifle would develop osteoarthritic changes in the joint. It is impressive that the great value of the patella is depicted in the effort of the organism to create harder tissues (ossifications) along the patellar ligament to substitute its presence [7].
In PP, after the first month, the animals use their knees freely without any attempt to protect them. After PP, the alterations in the quadriceps apparatus predispose the knee joint to the slow development of degenerative alterations, which are progressive. On the other hand, after TP, a thickening and striation of the patellar bed and the formation of fibro cartilage and bone in the extensor apparatus manifested [7]. Although there is poor veterinary literature, from the long-term follow-up of our case, it seems that TP is a feasible salvage procedure for dogs. Also, in humans, TP gives good to excellent results [9], providing no ligamentous instability and no early arthrosis but only a decrease in extensor muscle strength to 75% of normal [10]. Patellar fractures are the main cause of patellectomy. Osteosynthesis is performed for most of them, while polar patellar fractures often produce fragments that are too small for fixation. These small fragments have little effect on the extensor apparatus or femoropatellar articulation and are resected [11]. In a limited series of canine patellar fractures, two dogs were successfully treated by PP [12], and degenerative joint disease developed in only one case considered clinically insignificant [13]. However, achieving the successful union of a portion of the patella or preserving a fragment large enough to contribute to the extensor mechanism typically results in better function than with patellectomy [2,10,14]. On the other hand, recent studies report excellent long-term clinical outcomes in dogs despite postoperative patellar fracture non-union [15,16]. In our case, initially, PP was performed due to comminuted fractures in the distal patellar pole, but after a few weeks, the patella became necrotic and detached from its soft tissue attachments, so TP was inevitable. Severe soft tissue trauma or infection of the stifle could be the cause of patellar rejection [17]. In humans, the best results are obtained when TP is performed through a longitudinal excision and in combination with reinforcement of the extensor mechanism [9]. In our case, quadriceps reconstructive surgery was avoided because the former patellar ligament avulsion had been managed surgically. Primary repair of patellar ligament rupture or avulsion is necessary to restore extensor function to the stifle. Due to the dog’s aggressive behavior, a double loop of orthopedic wire, one in a mattress and the other in a figure eight configuration, was used to relieve the tension in the ligament suture line. For the latter, several horizontal mattress sutures (propylene 0) were placed between the proximal free end of the avulsed ligament and the soft tissues in the cranial surface of the patella. This technique was preferred instead of a classical tendon suture passing through a transverse drilled tunnel in the fractured patellar to prevent its feather from weakening. External stabilization or other forms of stifle motion restriction (e.g., transarticular external skeletal fixation) was avoided for the joint to be functional to restore the femoropatellar articulation as soon as possible. Unfortunately, the dog was unable to be restricted, and although the wire loops were repositioned, the patellar ligament was restored. The prognosis for isolated patellar ligament rupture is fair to good, although many patients have a reduced stifle range of motion [14]. The abovementioned stifle problems were complicated by joint infection due to penetrating wounds. Unfortunately, proper management of the infection was impossible due to the administration of antimicrobial drugs by the owner, the aggressive behavior of the dog, and the incomplete removal of the drain tube by the latter. As a result, the drug therapy was blind and longstanding, combined with multiple surgical debridement. The presence of nonabsorbable sutures inside the joint favors the infection, but initially, they were necessary for the patellar ligament repair. Finally, despite the difficulties, the infection was eradicated. The satisfactory outcome may be attributed to the early beginning of the treatment, e.g., before extensive joint damage has occurred [18]. The prognosis for normal joint function varies and depends on the amount of cartilage that has been destroyed; however, most dogs with bacterial septic arthritis respond well to treatment and are free of clinical signs of the disease at follow-up [19,20]. TP is considered a last-chance procedure when all other alternatives have been exhausted [7]. In our case, TP was complicated with patellar ligament avulsion and joint infection, and the predictable stifle osteoarthritis resulted. However, follow-up after 7 years showed that TP is a feasible salvage procedure as it provides a satisfactory stifle function and only a mild degree of lameness. Interestingly, patellar ligament ossification was noticed, which was increased at the site of the rejected patella, representing its significance for the quadriceps extensor mechanism. This ligament ossification has been reported as a rare pathology that may be seen as a complication after TP in humans [21]. Worrel (1975) assumed that the palpable firm mass at the site of the patellectomy in four dogs was an ossific nucleus of a regenerating patella. This mass was smaller than the original patella and appeared as an oval radiopacity on radiographs [22].
The animals examined in the late stages exhibited a knobby configuration. The femoral condyles invariably showed advanced hypertrophic alterations, including marginal osteophytes, erosion of articular cartilage, and obliteration of the intercondylar area on the cranial surface of the femoral by bony and cartilaginous excrescences. Excision of the proximal or the distal patellar halves produce abnormal alterations, but these changes are far less extensive than those encountered following TP. However, even in this latter group, the changes were mildly progressive. It is reasonable to assume that if the animals had lived long enough, the alterations may reach sufficient magnitude to produce varying degrees of dysfunction [7].
Prosthetic replacement of the patella could be a promising alternative to TP in dogs. Indeed, according to an experimental study, no dogs with prosthetic patellar replacement displayed discernible functional disturbances, while all but one of the dogs with patellectomy developed pathological alterations in the patellar bed of the femur and showed lameness [20]. In our case, stifle infection, multiple adhesions in the original patellar site, and financial restrictions remove this technique as a possibility.
Conclusion
In conclusion, TP seems to be a feasible salvage procedure, especially in complicated comminuted patellar fractures in dogs. Though the development of osteoarthritis is inevitable, the long-term clinical outcome in this case is satisfactory.
Conflicts of interest: There was no grant or other financial support provided for this study. There are also no conflicts of interest to declare.
References
- JK Roush. Canine patellar luxation, Vet Clin North Am Small Anim Pract. 1993; 23: 855-868.
- VA Mittal. A case for partial patellectomy, J Postgrad Med. 1995; 41: 31-33.
- SJ Langley-Hobbs. The patella, fabellae and popliteal sesamoids, in: T.J. Gemmill, D.N. Clements (Eds.), Manual of Canine and Feline Fracture Repair and Management, BSAVA, Gloucester. 2016; 353-362.
- H Kaufer. Mechanical function of the patella, J Bone Joint Surg Am. 1971; 53(8): 1551-1560. https:// DOI:10.2106/00004623-197153080-00007.
- L Qin, KS Leung, CW Chan, LK Fu, R Rosier. Enlargement of remaining patella after partial patellectomy in rabbits, Med Sci Sports Exerc. 1999; 31(4): 502-506. https:// DOI:10.1097/00005768-199904000-00002.
- M Milankov, N Miljkovic, M. Stankovic, Treatment of the knee stiffness caused by partial patellectomy- Technical tricks, Indian J Med Sci. 2005; 59: 534-537.
- AF Depalma, JJ Flynn. Joint changes following experimental partial and total patellectomy, J Bone Joint Surg Am. 1958; 40(2): 395-413.
- K Hayashi, J Lansdowne, L Dejardin. Patellar luxation in dogs, in: M.J. Bojrab, E. Monnet (Eds.) Mechanisms of disease in small animal surgery, third ed., Teton New Media, Jackson. 2010; 1936-1953.
- E Cavaignac, R Pailhe, N Reina, M Wargny, J Bellemans, et al. Total patellectomy in knees without prior arthroplasty: A systematic review, Knee Surg Sports Traumatol Arthrosc. 2014; 22(12): 3083-3092. https:// DOI:10.1007/s00167-014-3012-7.
- S. Cantin, C. Laroche, P. Lavallee, J.M. Lessard, Patellectomy: results of a long-term follow-up, Can J Surg. 1993; 36(5): 461-463. https:// PMID: 8221403.
- RH Denny, SJ Butterworth. The Stifle, in: A Guide to Canine and Feline Orthopaedic Surgery, fourth ed., Blackwell Science, Oxford. 2000; 512-553.
- A Carb. A partial patellectomy procedure for transverse patellar fractures in the dog and cat, J Am Anim Hosp Assoc. 1975; 11: 649-657.
- R.A.S. White, Bilateral patellar fracture in a dog, J Small Anim Pract. 1977; 18(4): 261-265. https://doi.org/10.1111/j.1748-5827.1977.tb05880.x.
- MP Kowaleski, RJ Boudrieau, A Pozzi. Stifle joint, in: S.A. Johnston, KM Tobias, (Eds.), Veterinary Surgery Small Animal, second ed., Elsevier, St Louis. 2018; 1071-1168.
- B Cruciani, D Gagnon, M Freire, X Montasell. Excellent long-term clinical outcome in a young athletic dog following surgical complications of a comminuted patellar fracture and patellar ligament rupture, Can Vet J. 2021; 62: 945-950.
- M Sprocatti, E Kvale, M Solano. Combined internal fixation and transarticular external skeletal fixation to treat traumatic patellar fractures in five dogs, N Z Vet J. 2022; 70: 119-127. DOI: 10.1080/00480169.2021.1963872
- Κ Hayashi, KS Schulz, TW Fossum. Management of specific fractures, in: Fossum TW, (Ed.), Small Animal Surgery, fifth ed., Elsevier, Philadelphia. 2019; 1036-1133.
- D. Bennett, D.J. Taylor, Bacterial infective arthritis in the dog, J Small Anim Pract. 1988; 29(4): 207-230. https://doi.org/10.1111/j.1748-5827.1988.tb02278.x.
- RH Denny, SJ Butterworth. Infective (Septic) Arthritis. in: A Guide to Canine and Feline Orthopaedic Surgery, fourth ed., Blackwell Science, Oxford. 2000; 73-76.
- KS Schulz, K Hayashi, TW Fossum. Diseases of the Joints. in: T.W. Fossum (Ed.), Small Animal Surgery, fifth ed., Elsevier, Philadelphia. 2019; 1134-1279.
- H Cakici, O Hapa, K Ozturan, M Guven, I Yucel. Patellar tendon ossification after partial patellectomy: a case report, J Med Case Rep. 2010; 4: 47.
- RV Worrell. A comparison of patellectomy with prosthetic replacement of the patella, Clin Orthop Relat Res. 1975; 111: 284-289. https://DOI:10.1097/00003086-197509000-00037.
