
Open Access, Volume 10
Acute-onset heart failure and diabetes mellitus: A multicenter database analysis
Mohamed Alrayyashi1 ; Mohammed Uddin2*; Tanveer Mir1 ; Waqas Qureshi4 ; Sheikh Mujeeb3
1Internal Medicine, Wayne State University Medical Center, Detroit MI, USA.
2Cardiovascular Disease, Detroit Medical Center, Wayne State University, Detroit, MI, USA.
3Interventional Cardiology, The University of Massachusetts, Worcester, MA, USA.
4Division of Cardiology, Promedical Medical Center, Toledo, Ohio, USA.
Mohammed Uddin
Division of Cardiology, Wayne State University, School of Medicine, USA.
Email: eh5589@wayne.edu
Received : Apr 16, 2024,
Accepted : May 15, 2024
Published : May 20, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Background: Literature regarding outcomes of acute Heart Failure with reduced Ejection Fraction (HFrEF) and acute Heart Failure with preserved Ejection Fraction (HFpEF) in patients with Diabetes Mellitus (DM) is still evolving.
Objective: To study clinical outcomes and all-cause mortality of acute HFrEF and acute HFpEF in DM patients.
Methods: Data from the National Emergency Department Sample (NEDS), which constitutes 20% of Emergency Departments (ED) within the United States (US), was analyzed for hospitalizations related to acute HF and DM using the International Classification of Diseases-10 (ICD-10) codes.
Results: Out of the total 1,479,716 adult acute HF encounters (mean age 69.7±14.9 years, 47.3% females) recorded for the years 2016-2018, 803,308 (54.3%) were acute HFrEF-related, with 317,517 (39.5%) DMrelated, while 481,985 (32.5%) were acute HFpEF-related, with 195,945 (40.6%) DM-related. The HFrEF and HFpEF with DM group had higher multi-organ complications including NSTEMI, Acute Kidney Injury (AKI), and AKI requiring hemodialysis. However, the mortality for both HFrEF and HFpEF subgroups were higher compared to DM (5% vs 4.8% and 3.5% vs 3%, respectively, p<0.001). HFrEF with DM groups had higher cardiac procedures including stress test, coronary angiography, and PCI (29.9% vs 24.8%, 19% vs 15.4%, and7.6% vs 7%, respectively; p<0.001) compared to their counterparts. Similarly, HFpEF with DM groups also had higher cardiac interventions including stress test, coronary angiography, and PCI (19% vs 17.1%, 8.1% vs 7.1%, and 2.6% vs 2.1%, respectively; p<0.001) compared to their counterparts.
Conclusion: HFrEF and HFpEF complicated by DM did not show a significant worsening in mortality rates. Given higher ischemic evaluation associated with DM, we suggest more randomized trials to evaluate if procedures had any mortality benefits.
Keywords: Acute Heart Failure with Reduced Ejection Fraction (HFpEF); Acute Heart Failure with preserved Ejection Fraction (HFpEF); Diabetes Mellitus (DM); All-cause mortality; Percutaneous Coronary Intervention (PCI); Coronary Artery Bypass Grafting (CABG).
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Amandeep S (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Amandeep S. Pericardial effusion and impaired diastolic cardiac function as a result of a giant colonic diverticulum. Open J Clin Med Case Rep. 2024; 2241.
Introduction
Heart Failure (HF) and Diabetes Mellitus (DM) form a few of the major healthcare burdens in the United States (US) and worldwide. Patient with DM have a 2-fold increase in the risk of developing both variants of HF [1]. It is known that DM is associated with increased fatty acid use by the myocardium, decreased glucose use, increased myocardial oxygen consumption, and decreased cardiac efficiency [1]. According to the CDC, in 2018 there was a prevalence of 34.2 million American living with DM, causing an excess of $327 billion to the American Health system [2]. The National Health and Nutrition Examination Survey 2013-2016 reported that heart failure had a prevalence of 6.2 million patients in the United States, which was higher than 5.7 million for the years 2009-2012 [3,4]. For the year 2015, from amongst the top 10 causes of death in the United States, diabetes mellitus was the 7th and heart failure was the 9th leading etiology. These trends continued in subsequent years.
The ADVANCE trial (target HbA1c of 6.5%) showed that intensive glycemic control did not cause any reduction in macrovascular events [5]. Furthermore, the ACCORD trial showed that a target HbA1c of 6% had an increase in mortality by 22% [6]. A prospective study reported high rates of mortality and complications associated with acute Heart Failure with preserved Ejection Fraction (HFpEF) and acute Heart Failure with reduced Ejection Fraction (HFrEF); however, the studies were small [7]. The Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) study was done for patients who had new-onset heart failure exacerbation, or acute on chronic heart failure [8].
Data regarding the clinical complications, cardiovascular procedures and mortality outcomes in patients with acute HFpEF and acute HFrEF in conjunction with DM could provide information for improving outcomes. Therefore, we aimed to evaluate these factors for the years 2016-2018 from the National Emergency Department Sample (NEDS) database.
Methods
Study population and inclusion criteria
This is an observational cohort study of patients hospitalized for acute HF during the years 2016- 2018 in the NEDS database. NEDS has records of patients who present to the emergency department. The information of patients who get admitted to inpatient services is retained for each emergency encounter. The NEDS constitutes an approximately 20% sample of hospital-owned Emergency Departments (ED) in the United States (US) [6]. Using a stratified, random sampling design, a sample of hospital-owned emergency departments from the United States participating in both the State Inpatient Databases (SID) and the State Emergency Department Databases (SEDD) was selected, and 100% of the ED visits the selected hospital-owned emergency departments were retained. Hospitals were included in the NEDS sample based on geographic region (northeast, mid-west, west, or south), location (urban or rural), teaching status (teaching or non-teaching), ownership (public, private not for profit, private for-profit), and trauma center designation. A total of 950 emergency departments were included in the NEDS. From each selected EDs, all visits were included, which amounted to more than 33 million unweighted visits each year. Patients with age <18 years at the time of presentation were excluded from the study. The study was exempt from institutional review board evaluation however it was performed according to the ethical criteria set up by Healthcare Cost and Utilization Project (HCUP) [6].
Study definitions
Acute HF was defined by International Classification of Diseases-10 (ICD-10) codes of «I50.811», «I50.21», «I50.31», «I50.20», «I50.41» and «I50.40». Patients younger than 18 years (n=1,858) were excluded. Acute HF was further divided into acute HFpEF using ICD-10 code «I50.31” and acute HFrEF using ICD-10 codes «I50.21» and “I50.23». Based on the exclusion, 1,479,910 patients with acute HF were identified. Out of these, 480,157 were acute HFPEF and 462,613 were acute HFREF making a national prevalence of 32.4% and 31.3% respectively among acute HF hospitalizations. Data was verified for patients of chronic heart failure or acute on chronic HF using ICD-10 codes “I50.22», «I50.32», «I50.813», «I50.23», «I50.33», «I50.42», «I50.43», and «I50.42». No patients were identified using these codes which confirmed that only new-onset acute heart failure patients were included in the study. Details of ICD codes utilized to identify various complications are given in the supplementary file.
Patient and hospital characteristics
Baseline patient demographic characteristics (age, sex, insurance payer) were extracted. Diagnostic codes were used to identify hypertension, diabetes mellitus, hyperlipidemia, obesity, smoker, Peripheral Vascular Disease (PVD), chronic kidney disease, fluid or electrolyte imbalance, liver disease, chronic obstructive pulmonary disease, congenital heart disease, drug abuse, cancer, prior myocardial infarction, prior coronary artery bypass grafting, history of coronary artery disease, alcohol use, hemodialysis, hypothyroidism, smoking, and chronic obstructive pulmonary disease, were extracted using ICD-10 codes. Elixhauser comorbidity index codes were also used to extract comorbidities [7]. Cardiovascular procedures including Percutaneous Coronary Intervention (PCI, coronary artery bypass grafting (CABG), implantable defibrillator, Permanent Pacemaker (PPM), coronary angiography, and Mechanical Circulatory Support (MCS) were extracted using the CD-10 Procedural Classification System (PCS) codes (Supplementary file). We extracted complications associated with each sub-types of HF with and without DM. Complications included mortality, angina, Non-ST Elevated Myocardial Infarction (NSTEMI), ST-Elevated Myocardial Infarction (STEMI), Acute Kidney Injury (AKI), Ventricular Tachycardia/Fibrillation (VT/VF), intracardiac conduction block, cardiogenic shock, Pulmonary Embolism (PE), septic shock, and admission to Intensive Care Unit (ICU). All complications were generated using ICD-10 codes (supplementary file).
Outcomes
The primary outcome of the analysis was all-cause mortality during hospitalization for acute HFpEF and HFrEF complicated by DM. We also evaluated clinical complications, 30-day readmission rates, and cardiac procedures performed among patients with acute HFpEF and acute HFrEF encounters associated with DM.
Statistical methods
Categorical variables were expressed as weighted values along with percentages and continuous variables were expressed as mean ± standard deviation if the variable was not skewed and as median with 25th and 75th percentiles otherwise. Descriptive statistics were performed for demographics and comorbidities which were stratified by the acute HFpEF and acute HFrEF and were compared with the rest of the population. We used the survey statistical method to perform a weighted analysis. Pearson’s chi-square test was used to compare categorical variables and linear regression was used to compare continuous variables. We calculated mortality for acute HFpEF and acute HFRrEF. We extracted complications associated with acute HFpEF and HFrEF. The proportions were compared using the Chi-square test.
All analyses were weighted analyses. Statistical analysis was performed using STATA version 16.1 (College Station, Texas). All p values were 2-sided, with a significance threshold of p<0.05.
Results
Out of the total 1,479,716 acute HF patients (mean age 69.7±14.9 years, 47.3% females) were recorded in NEDS for the years 2016-2018, 803,308 (54.3%) had acute HFrEF while 481,985 (32.5%) had acute HFpEF (Figure 1).
When comparing the two major groups of HFrEF vs HFpEF, the prevalence of ischemic heart disease was higher among HFrEF 109,118 (13.6%) vs 38,783 (8.1%), also noticed higher PCI 88,859 (11.1%) vs 41,401 (8.6%) and higher CABG 83,812 (10.4%) vs 39,701 (8.2%) in the HFrEF group. The comparison has been provided in Table 1.
On subgroup analysis, 317,517 (39.5%) of the total acute HFrEF encounters were complicated by DM. The acute HFrEF with DM were males with a higher prevalence of hypertension, hyperlipidemia, prior history of MI, prior PCI, and prior CABG. Medicare was the primary payor across all groups. Baseline characteristics are provided in Table 1.
On subgroup analysis, 195,945 (40.6%) of the total acute HFpEF encounters were complicated by DM. Patients with acute HFpEF with DM were more likely to be elderly, females with a higher prevalence of hypertension, hyperlipidemia, prior stroke, and prior MI. Medicare was the primary payor across all groups. Baseline characteristics are provided in Table 2.
Clinical complications
The HFrEF with DM group had higher multi-organ complications including NSTEMI (14.6% vs 12.9%; p-value<0.001), Acute Kidney Injury (AKI) (29.3% vs 26.2%; p-value<0.001), AKI requiring hemodialysis (10.5% vs 6.7%; p-value<0.001) when compared to HFrEF group only. Other fewer complications associated with acute HFREF are given in Table 3.
Similarly, the HFpEF with DM group had higher multi-organ complications including NSTEMI (8.4% vs 7.4%; p-value<0.001), Acute Kidney Injury (AKI) (33.1% vs 28.1%; p-value<0.001), AKI requiring hemodialysis (8.8% vs 5.5%; p-value<0.001) when compared to HFpEF group only. Other complications associated with acute HFpEF and DM are given in Table 4.
Mortality analysis
Out of 1,479,716 total acute onset HF encounters, the overall all-cause mortality was 55,403 (3.7%) during the hospitalizations. On subgroup analysis, the all-cause mortality for HFrEF only was higher as compared to HFrEF with DM (5% vs 4.8%; p<0.001) while the all-cause mortality for HFpEF only was higher as compared to HFpEF with DM (3.5% vs 3%; p<0.001).
Cardiac procedure analysis
HFrEF with DM groups had higher cardiac procedures including stress test, coronary angiography, and PCI (29.9% vs 24.8%, 19% vs 15.4%, and7.6% vs 7%, respectively; p<0.001) compared to their counterparts. Similarly, HFpEF with DM groups also had higher cardiac interventions including stress test, coronary angiography, and PCI (19% vs 17.1%, 8.1% vs 7.1%, and 2.6% vs 2.1%, respectively; p<0.001) compared to their counterparts. Other procedural data are presented in Supplementary Table 1 and Table 2.
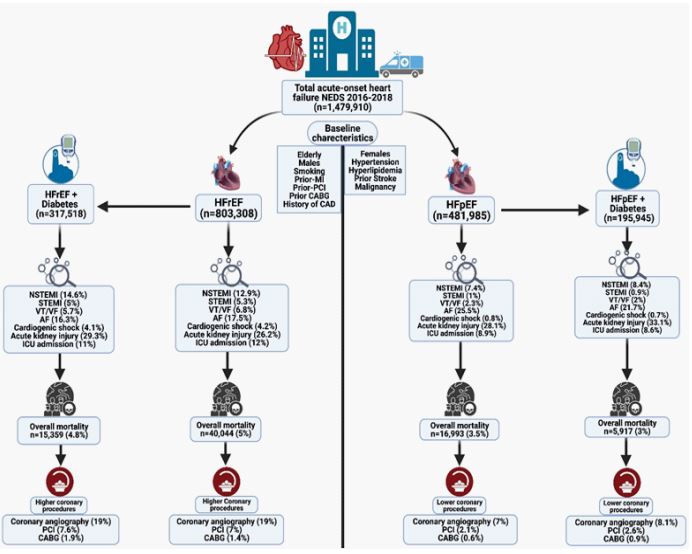
Figure 1: Graphic abstract, created with BioRender.com
Discussion
Metabolic alterations associated with DM have been recognized since the 1970s as a distinct pathway in the onset and progression of HF, independent of atherosclerotic cardiovascular disease [9-11]. Our study utilizes the multicenter database to retrospectively evaluate both subtypes of acute onset HF both alone and with DM. The most salient findings of our study were as follow: 1) Compared to patients with acute HFrEF or acute HFpEF alone, those with acute HFrEF or HFpEF with DM had significantly higher rates of AKI, AKI needing hemodialysis, and NSTEMI 2) Acute HFrEF or HFpEF with DM subgroups also exhibited higher rates of undergoing PCI or CABG 3) DM was not associated with worsening overall mortality in patients with both HFrEF and HFpEF and 4) HFrEF with and without DM was associated with more complications and worse outcomes than HFpEF with and without DM.
Acute heart failure with reduced ejection fraction and diabetes mellitus
This study added results to the controversial evidence available in literature about the impact of diabetes on complications and prognosis amongst patients admitted with acute HF. In our study, approximately one-third of patients hospitalized with HFrEF had diabetes. We observed a higher rate of AKI and AKI needing hemodialysis amongst patients who had HFrEF with diabetes compared to HFrEF alone. Kidneys in patients with DM are characterized by severe inflammation, athero- and arteriosclerosis, and glomerular damage. Thus, the kidneys are more prone to damage from ischemic injury during HFrEF exacerbations [12]. This endorsed the findings by others [13-16].
Hyperglycemia-accelerated atherosclerosis is the most common cause of HF in people with DM [17]. De Groote et. al evaluated 1,246 patients with left ventricular dysfunction and aimed to use diabetic status as a prognostic indicator in heart failure patients, finding DM to be an independent predictor of cardiovascular mortality in patients with ischemic heart disease compared to patients without ischemic heart disease (HR=1.43 [1.03;1.98] P=0.03 vs HR=0.46 [0.23;0.88], P=0.02) [18]. We found that HFrEF with DM was associated with higher rates of known ischemic heart disease, development of NSTEMI during the hospitalization, as well as increased rates undergoing PCI or CABG during the hospitalization.
We found improved mortality rates in patients with HFrEF with DM compared to HFrEF alone. This is analogous to the findings by others who reported a comparable prognosis in HFrEF with DM and HFrEF alone [17,19]. However, these finding contrasts previous studies. A retrospective Scottish population study found poorer prognostic outcomes after 1-year follow-up of patients with HF with DM compared to HF alone [20]. DIAMOND-CHF (Danish Investigations of Arrhythmia and Mortality on Dofetilide in Congestive Heart Failure) was a large Danish trial with >5,000 patients reporting higher 1-year mortality rates among patients with HF with DM than HF alone [21].
A potential reason for these discrepancies is a higher rate of undergoing PCI and CABG, procedures which are known to have mortality benefit, amongst the HFrEF with DM cohort compared to the HFrEF alone cohort. This is corroborated by our study as well, which finds HFrEF with DM group underwent more PCI and CABG than HFrEF alone.
Table 1: Baseline characteristics of Heart Failure with Reduced Ejection Fraction (HFrEF) only in comparison to HFrEF with Diabetes Miletus (DM).
| Variables | HFrEF (n=803,308) | HFrEF + DM (n=317,518) | P value |
|---|---|---|---|
| Age, Years | 68.8±14.9 | 72.7±13.9 | <0.001 |
| Female | 326,676 (40.7%) | 126,490 (39.8%) | <0.001 |
| Male | 476,632 (59.3%) | 191,027 (60.2%) | <0.001 |
| Medicare | 504,281 (64.4%) | 208,465 (67.4%) | <0.001 |
| Medicaid | 105,668 (13.5%) | 39,317 (12.7%) | <0.001 |
| Private Insurance | 132,632 (16.9%) | 48,556 (15.7%) | <0.001 |
| Self-Pay | 39,400 (5%) | 12,838 (4.2%) | <0.001 |
| Urban Hospital | 749,247 (93.3%) | 297,488 (93.7%) | 0.002 |
| Teaching Hospital | 518,911 (64.6%) | 207,202 (65.2%) | <0.001 |
| Hypertension | 642,901 (80%) | 284,028 (89.4%) | <0.001 |
| Hyperlipidemia | 326,337 (40.6%) | 163,413 (51.5%) | <0.001 |
| Smoking | 154,185 (19.2%) | 50,745 (16%) | <0.001 |
| Intravenous drug use | 11,981 (1.5%) | 3,351 (1.1%) | <0.001 |
| History of Stroke | 68,081 (8.5%) | 31,672 (10%) | <0.001 |
| Prior MI | 109,118 (13.6%) | 51,656 (16.3%) | <0.001 |
| Prior PCI | 88,859 (11.1%) | 44,672 (14.1%) | <0.001 |
| Prior CABG | 83,812 (10.4%) | 45.013 (14.2%) | <0.001 |
| Family History of CAD | 54,457 (6.8%) | 20,729 (6.5%) | <0.001 |
MI: Myocardial Infarction; PCI: Percutaneous Coronary Intervention; CABG: Coronary Artery Bypass Grafting; CAD: Coronary Artery Disease.
Table 2: Baseline characteristics of Heart Failure with Preserved Ejection Fraction (HFpEF) only in comparison to HFpEF with Diabetes Miletus (DM).
| Variables | HFpEF (n=481,985) | HFpEF + DM (n=195,945) | P value |
|---|---|---|---|
| Age, Years | 68.5±13.6 | 71.7±13.3 | <0.001 |
| Female | 287,297 (59.6%) | 111,641 (57%) | <0.001 |
| Male | 194,688 (40.4%) | 84,304 (43%) | <0.001 |
| Medicare | 369,329 (77.9%) | 146,674 (76.3%) | <0.001 |
| Medicaid | 34,125 (7.2%) | 16,230 (8.4%) | <0.001 |
| Private Insurance | 58,173 (12.3%) | 24,604 (12.8%) | <0.001 |
| Self-Pay | 11,796 (2.5%) | 4,700 (2.4%) | <0.001 |
| Urban Hospital | 454,229 (94.2% | 184,667 (94.2%) | 0.002 |
| Teaching Hospital | 287,761 (59.7%) | 11,991 (60.2%) | <0.001 |
| Hypertension | 414,768 (86%) | 181,666 (92.7%) | <0.001 |
| Hyperlipidemia | 214,021 (44.4%) | 105,287 (53.7%) | <0.001 |
| Smoking | 63,324 (13.1%) | 23,312 (11.9%) | <0.001 |
| Intravenous drug use | 5,604 (1.2%) | 2,022 (1%) | <0.001 |
| History of Stroke | 46,893 (9.7%) | 20,172 (10.3%) | <0.001 |
| Prior MI | 38,783 (8.1%) | 18,620 (9.5%) | <0.001 |
| Prior PCI | 41,401 (8.6%) | 20,843 (10.6%) | <0.001 |
| Prior CABG | 39,701 (8.2%) | 20,555 (10.5%) | <0.001 |
| Family History of CAD | 27,355 (5.7%) | 11,165 (5.7%) | <0.001 |
MI: Myocardial Infarction; PCI: Percutaneous Coronary Intervention; CABG: Coronary Artery Bypass Grafting; CAD: Coronary Artery Disease.
Table 3: Clinical complications associated with Heart Failure with Reduced Ejection Fraction (HFrEF) only in comparison to HFrEF with Diabetes Miletus (DM).
| Complications | HFrEF (n=803,308) | HFrEF + DM (n=317,518) | P value |
|---|---|---|---|
| Mortality | 40,044 (5%) | 15,359 (4.8%) | <0.001 |
| Atrial Fibrillation | 140,747 (17.5%) | 51,807 (16.3%) | <0.001 |
| VT/VF | 54,302 (6.8%) | 18,080 (5.7%) | <0.001 |
| NSTEMI | 103,462 (12.9%) | 46,365 (14.6%) | <0.001 |
| STEMI | 42,272 (5.3%) | 15,808 (5%) | <0.001 |
| Acute kidney Injury | 210,245 (26.2%) | 93,174 (29.3%) | <0.001 |
| AKI needing Hemodialysis | 53,734 (6.7%) | 33,353 (10.5%) | <0.001 |
| Cardiogenic Shock | 33,818 (4.2%) | 13,043 (4.1%) | <0.001 |
| Pulmonary Embolism | 28,087 (3.5%) | 9,161 (2.9%) | <0.001 |
| Infective Endocarditis | 5,270 (0.6%) | 1,571 (0.5%) | <0.001 |
| Sepsis | 87,176 (10.9%) | 34,847 (11%) | <0.001 |
| Septic Shock | 32,731 (4.1%) | 12,056 (3.8%) | <0.001 |
| ICU admission | 96, 150 (12%) | 34,788 (11%) | <0.001 |
| Mechanical Ventilation | 69,112 (8.6%) | 26,327 (8.3%) | <0.001 |
NSTEMI: Non-ST Elevated Myocardial Infarction, STEMI; ST-Elevated Myocardial Infarction, VT/VF: Ventricular Tachycardia/ Fibrillation; ICU: Intensive Care Unit.
Table 4: Clinical complications associated with Heart Failure with Preserved Ejection Fraction (HFpEF) only in comparison to HFpEF with Diabetes Miletus (DM).
| Complications | HFpEF (n=481,985) | HFpEF + DM (n=195,945) | P value |
|---|---|---|---|
| Mortality | 16,993 (3.5%) | 5,917 (3%) | <0.001 |
| Atrial Fibrillation | 122,975 (25.5%) | 42,610 (21.7%) | <0.001 |
| VT/VF | 10,910 (2.3%) | 3,906 (2%) | <0.001 |
| NSTEMI | 35,882 (7.4%) | 16,429 (8.4%) | <0.001 |
| STEMI | 4,640 (1%) | 1,816 (0.9%) | <0.001 |
| Acute kidney Injury | 135,590 (28.1%) | 64,924 (33.1%) | <0.001 |
| AKI needing Hemodialysis | 26,539 (5.5%) | 17,165 (8.8%) | <0.001 |
| Cardiogenic Shock | 4,019 (0.8%) | 1,486 (0.7%) | <0.001 |
| Pulmonary Embolism | 16,146 (3.3%) | 5,340 (2.7%) | <0.001 |
| Infective Endocarditis | 3,915 (0.8%) | 1,192 (0.60%) | <0.001 |
| Sepsis | 58,821 (12.2%) | 22,977 (11.7%) | <0.001 |
| Septic Shock | 14,827 (3.1%) | 5,216 (2.7%) | <0.001 |
| ICU admission | 42,860 (8.9%) | 16,797 (8.6%) | <0.001 |
| Mechanical Ventilation | 29,148 (6.1%) | 12,531 (6.4%) | <0.001 |
NSTEMI: Non-ST Elevated Myocardial Infarction, STEMI; ST-Elevated Myocardial Infarction, VT/VF: Ventricular Tachycardia/ Fibrillation; ICU: Intensive Care Unit.
Acute heart failure with preserved ejection fraction and diabetes mellitus
HFpEF is emerging as a significant clinical problem for patients with DM. Current data suggests that between 30% and 40% of patients with HFpEF have coexisting DM. The Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist Trial (TOPCAT) found that HFpEF with DM was associated with an increased risk for cardiovascular death [23]. In a post-hoc analysis from the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) study, HFpEF with diabetes was associated with a twofold increased risk of cardiovascular death or heart failure hospitalization [24]. Similarly, in the Irbesartan in Heart Failure with Preserved Ejection Fraction Trial (I-PRESERVE) study, HFpEF with DM had a 1.75-fold increased risk of cardiovascular death [25].
However, our study demonstrated that HFpEF with DM was not associated with a worse overall mortality. This again could be explained by higher rates of undergoing PCI and CABG amongst the HFpEF with DM cohort compared to the HFrEF alone cohort, highlighting survival benefits of early intervention amongst patients admitted for HFpEF.
Acute heart failure with reduced and preserved ejection fraction
The OPTIMIZE-HF registry reported mortality rates of (3.8%) in HFrEF which was similar to our study (4.4%) [8]. Gomez-Soto et al expanded on this data and found that acute HFrEF was associated with greater mortality rates compared to acute HFpEF patients amongst 267,231 patients in Spain (p<0.05) [26]. Our study validated this and found an increase in all-cause mortality in acute HFrEF patients compared to acute HFpEF (5.7% vs 3.5%, P<.0001).
High mortality among acute HFrEF is a multifactorial process: Patients with acute HFrEF have a higher comorbidity profile, higher rates of complications, and a higher number of ICU admissions compared to acute HFpEF patients (15% vs 8.9%, P<.0001) and exhibit higher rates of known ischemic cardiac events compared to patients with acute HFpEF, as has been validated previously [27-29].
Since the incidence of diabetes in HF patients is likely to further increase in the future, this will become a major health care problem with high morbidity and mortality as well as high costs for society [29]. Therefore, it is important to recognize diabetes in patients with HF. For that reason, more future clinical research is required for medical treatment and early coronary intervention on diabetics with HF.
Our study has multiple strengths. First, it represents the whole population of the United States. Secondly, a significant number of hospitalizations are recorded yearly for acute heart failure with significant mortality. This gives us rich epidemiological data that allows us to accurately compare subgroups with HF and DM as we have demonstrated. There are mortality benefits from screening tests for ischemic cardiomyopathy including stress tests and coronary angiography. However, the rates of undergoing stress tests and coronary angiography are dismal. This would suggest that there needs to be improvement in rates of procedures for cardiac ischemic work-up.
Study limitations
Our study has several limitations. First, this is a retrospective, observational study, and inference regarding causation should be made with caution as controlling for comorbidities is challenging. Also, we relied on reported ICD-10 codes to identify diagnoses to perform our analysis. The national emergency database is an administrative database that could be subject to inaccurate over-coding or underreporting of some comorbid diagnoses. There is also an absence of important information related to patients’ physical examination, medications, and laboratory results. We could not evaluate the time to coronary interventions and ischemic work up. We could not take into consideration echocardiography or radiography. A significant number of acute new onset heart failure was recorded as non-specific which we could not classify under HFpEF and HFrEF. Also, there could be some chances of selection bias for procedures. However, NEDS and the codes used in this study have been applied in multiple clinical studies and can be considered a highly reliable database. Given the large cohort analyzed in this study this minimizes the limitation.
Conclusion
The present analysis shows that although DM was associated with higher rates of cardio-renal complications including AKI, AKI requiring HD, and NSTEMI within both subtypes of HF population studied. Also, the rate of the ischemic evaluation was relatively higher in DM with HF subgroups. More importantly, we found that the all-cause mortality rate was not higher in patients with DM within both subtypes of HF, which suggest importance of early intervention. Given higher cardiac procedures performed in patients with associated DM, more clinical trials will be needed to work on the hypothesis generated.
References
- Kenny HC, Abel ED. Heart Failure in Type 2 Diabetes Mellitus. Circulation research. 2019; 124(1): 121-141. https://doi.org/10.1161/CIRCRESAHA.118.311371.
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020. Atlanta, GA: Centers for Disease Control and Prevention, U.S. Dept of Health and Human Services. 2020.
- Benjamin EJ, Muntner P, Alonso A, et al. Heart disease and stroke statistics-2019 update: A report from the American Heart Association. Circulation. 2019; 139(10): e56-e528.
- Members WG, Lloyd-Jones D, Adams RJ, et al. Executive summary: heart disease and stroke statistics-2010 update: A report from the American Heart Association. Circulation. 2010; 121(7): 948-954.
- Heller SR. ADVANCE Collaborative Group. A summary of the ADVANCE Trial. Diabetes care. 2009; 32(Suppl 2): S357-S361. https://doi.org/10.2337/dc09-S339
- Action to Control Cardiovascular Risk in Diabetes Study Group, Gerstein HC, Miller ME, Byington RP, Goff DC, Bigger JT, et al. Effects of intensive glucose lowering in type 2 diabetes. The New England journal of medicine. 2008; 358(24): 2545-2559. https://doi.org/10.1056/NEJMoa0802743.
- Spinar J, Parenica J, Vitovec J, et al. Baseline characteristics and hospital mortality in the Acute Heart Failure Database (AHEAD) Main registry. Critical Care. 2011; 15(6): R291. doi:10.1186/cc10584.
- Greenberg BH, Abraham WT, Albert NM, et al. Influence of diabetes on characteristics and outcomes in patients hospitalized with heart failure: A report from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). American Heart Journal. 2007; 154(2): 277.e1-277.e8. doi:https://doi.org/10.1016/j.ahj.2007.05.001.
- Kong MG, Jang SY, Jang J, et al. Impact of diabetes mellitus on mortality in patients with acute heart failure: A prospective cohort study. Cardiovasc Diabetol. 2020; 19: 49. https://doi.org/10.1186/s12933-020-01026-3.
- Echouffo-Tcheugui JB, Xu H, DeVore AD, Schulte PJ, Butler J, et al. Temporal Trends and Factors Associated with Diabetes Mellitus Among Patients Hospitalized with Heart Failure: Findings from Get with The Guidelines-Heart Failure Registry. Am Heart J. 2016; 182: 9-20. 10.1016/j.ahj.2016.07.025
- Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, et al. Hyperglycemia: An Independent Marker of in-Hospital Mortality in Patients with Undiagnosed Diabetes. J Clin Endocrinol Metab. 2002; 87(3): 978-82.
- Sandesara, Pratik, et al. Cardiorenal Syndrome: Classification, Pathophysiology, Diagnosis, and Treatment Strategies: A Scientific Statement from the American Heart Association. Diabetes Care. 2017; 41: 150-155. https://doi.org/10.2337/dc17-0755.
- Hertzberg D, Sartipy U, Holzmann MJ. Type 1 and Type 2 Diabetes Mellitus and Risk of Acute Kidney Injury After Coronary Artery Bypass Grafting. Am Heart J. 2015; 170(5): 895-902.
- Rhee CM, Kalantar-Zadeh K. Diabetes Mellitus: Complex Interplay Between Metformin, AKI and Lactic Acidosis. Nat Rev Nephrol. 2017; 13(9): 521-2.
- Arbel Y, Fuster V, Baber U, Hamza TH, Siami FS, et al. Incidence, Determinants and Impact of Acute Kidney Injury in Patients with Diabetes Mellitus and Multivessel Disease Undergoing Coronary Revascularization: Results from the FREEDOM Trial. Int J Cardiol. 2019; 293:197-202.
- Patschan D, Müller GA. Acute Kidney Injury in Diabetes Mellitus. Int J Nephrol. 2016; 2016: 6232909.
- Targher G, Dauriz M, Tavazzi L, et al. IN-HF Outcome Investigators. Prognostic impact of in-hospital hyperglycemia in hospitalized patients with acute heart failure: results of the IN-HF (Italian Network on Heart Failure) outcome registry. Int J Cardiol. 2016; 203: 587-593.
- De Groote P, Lamblin N, Mouquet F, Plichon D, McFadden E, et al. Impact of diabetes mellitus on long-term survival in patients with congestive heart failure. Eur Heart J. 2004; 25(8): 656-62. doi: 10.1016/j.ehj.2004.01.010. PMID: 15084370.
- Jan C van den Berge, Alina A Constantinescu, Hendrik J Boiten, Ron T van Domburg, Jaap W Deckers, et al. Short- and Longterm Prognosis of Patients with Acute Heart Failure with and Without Diabetes: Changes Over the Last Three Decades. Diabetes Care. 2018; 41(1): 143-149.
- MacDonald MR, Jhund PS, Petrie MC, et al. Discordant short- and long-term outcomes associated with diabetes in patients with heart failure: importance of age and sex: a population study of 5.1 million people in Scotland. Circ Heart Fail. 2008; 1: 234-241
- Meagher P, Adam M, Civitarese R, Bugyei-Twum A, Connelly KA. Heart Failure with Preserved Ejection Fraction in Diabetes: Mechanisms and Management. Can J Cardiol. 2018; 34(5): 632-643. doi: 10.1016/j.cjca.2018.02.026.
- Sandesara, Pratik B, et al. The Prognostic Significance of Diabetes and Microvascular Complications in Patients with Heart Failure with Preserved Ejection Fraction. Diabetes Care. 2017; 41: 150-155. https://doi.org/10.2337/dc17-0755.
- MacDonald MR, Petrie MC, Varyani F, et al. CHARM Investigators. Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur Heart J. 2008; 29: 1377-1385.
- Kristensen SL, Mogensen UM, Jhund PS, et al. Clinical and echocardiographic characteristics and cardiovascular outcomes according to diabetes status in patients with heart failure and preserved ejection fraction: A report from the Irbesartan in Heart Failure with Preserved Ejection Fraction Trial (I-Preserve). Circulation. 2017; 135: 724-735.
- Gomez-Soto FM, Andrey JL, Garcia-Egido AA, et al. Incidence and mortality of heart failure: A community-based study. International Journal of Cardiology. 2011; 151(1): 40-45. doi:https://doi.org/10.1016/j.ijcard.2010.04.055
- Van der Vleuten PA, Rasoul S, Huurnink W, et al. The importance of left ventricular function for long-term outcome after primary percutaneous coronary intervention. BMC cardiovascular disorders. 2008; 8(1): 1-7.
- Hashmi KA, Abbas K, Hashmi AA, et al. In-hospital mortality of patients with cardiogenic shock after acute myocardial infarction; impact of early revascularization. BMC Research Notes. 2018; 11(1): 721. doi:10.1186/s13104-018-3830-7
- Kelly DJ, Gershlick T, Witzenbichler B, et al. Incidence and predictors of heart failure following percutaneous coronary intervention in ST-segment elevation myocardial infarction: The HORIZONS-AMI trial. American Heart Journal. 2011; 162(4): 663-670. doi:https://doi.org/10.1016/j.ahj.2011.08.002
- Baliga V, Sapsford R. Review article: diabetes mellitus and heart failure-an overview of epidemiology and management. Diab Vasc Dis Res. 2009; 6: 164-171.
