
Open Access, Volume 10
Pericardial effusion and impaired diastolic cardiac function as a result of a giant colonic diverticulum
Singh Amandeep*
Department of Emergency Medicine, Highland Hospital, 1411 East 31st Street, Oakland, CA 94602, USA.
Singh Amandeep
Department of Emergency Medicine, Highland Hospital, 1411 East 31st Street, Oakland, CA 94602, USA.
Email: amasingh@alamedahealthsystem.org
Received : Apr 05, 2024,
Accepted : May 13, 2024
Published : May 20, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Amandeep S (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Amandeep S. Pericardial effusion and impaired diastolic cardiac function as a result of a giant colonic diverticulum. Open J Clin Med Case Rep. 2024; 2241.
Short Report
This case report describes a Giant Colonic Diverticulum (GCD) found in association with a significant pericardial effusion and impaired cardiac function. A 63-year-old man presented to the Emergency Department with bilateral leg edema, mild dyspnea, and diarrhea. An echocardiogram demonstrated a large pericardial effusion and abnormal diastolic cardiac function. Abdominal imaging studies identified a 29 cm x 18 cm x 13 cm gas filled structure in the left upper quadrant concerning for GCD causing significant compression of the left lung and heart. Following surgical resection, the pericardial effusion resolved, cardiac function normalized, and the patient’s leg swelling improved. This is the first case report to record an association between GCD and pericardial effusion with impaired diastolic cardiac function.
Diverticulosis of the colon is a common and largely asymptomatic disease. 10-25% of patients develop acute diverticulitis [1], and commonly present to the emergency department with lower abdominal pain. A rare complication of this disease is the entrapment of gas and growth of a single outpouching into a Giant Colonic Diverticula (GCD), defined as an air-filled cystic diverticulum >4 cm in size [2]. This article describes a patient with a 29 cm x 18 cm x 13 cm GCD and diastolic dysfunction of the heart along with a large pericardial effusion, which resolved shortly after surgical resection of the GCD.
A 63-year-old man presented to the Emergency Department (ED) with several months of bilateral leg swelling and pain, loose stools, loss of appetite, and unintentional 15 lb. weight loss over 6 months. He denied any abdominal or back pain, nausea, vomiting, dizziness, or syncope. He did endorse some mild shortness of breath with exertion, but denied chest pain. He had no known medical problems. The patient had been homeless for about 2 years, and denied any alcohol or drug use. Vital signs were normal, and on exam, he was alert and oriented, his heart and lung exams were normal, and his abdomen was non-tender and not overtly distended. Abnormalities on exam included a small umbilical hernia and pitting edema in bilateral lower extremities. Lab workup included a complete blood count, comprehensive metabolic panel, liver function tests, thyroid studies, HIV test, and hemoglobin A1c. The only abnormal finding was anemia with a hemoglobin of 10.5 mg/dL. The patient was referred to a clinic for outpatient workup to include both an echocardiogram and colonoscopy given leg swelling and weight loss.
10 days later the patient returned to outpatient cardiology clinic for an echocardiogram and was noted to have a large pericardial effusion along with evidence of impaired relaxation of the left ventricle during diastole (Figure 1). Following transfer to the ED, he was noted to have a heart rate of 113 bpm and blood pressure of 129/70 mmHg; his respiratory rate, oxygen saturation and temperature were within normal limits. A chest x-ray ordered for his mild shortness of breath revealed a massively dilated, air-filled structure in the left upper quadrant with severe compression of the left lung and heart(Figure 2). A CT scan demonstrated massive dilation of a loop of bowel measuring 29 cm x 18 cm x 13 cm centered in the left upper quadrant with possible partial sigmoid volvulus (Figure 3).
Given risk for perforation, he was taken to the operating room the next morning for decompression and sigmoid colectomy with primary end-to-side rectosigmoid anastomosis. The operative time was prolonged due to extensive adhesions between the diverticulum and the spleen, diaphragm, stomach, and anterior abdominal wall. The pathology report describes a dilated portion of colon, consistent with a diverticulum; diverticulosis was present in the portion of resected colon, but there was no malignancy or dysplasia. He developed an anastomotic leak six days later, requiring conversion to end-colostomy. 12 days after surgery, a repeat echocardiogram showed significant resolution of the pericardial effusion and diastolic dysfunction; this was paralleled by improved in the patient’s leg swelling.
Diverticulosis of the colon is a common clinical entity affecting 35% of individuals over the age of 65 years in the Western world. First described in 1946 [2], GCD is a rare complication of diverticulosis that develops when herniation of the mucosa through the muscle wall leads to the development of a large airfilled cyst. The disease is typically limited to the sigmoid colon with over 90% of GCD localized to this area. Approximately 180 cases of GCD have been published [3], and a review of 135 patients found an overall 5% operative mortality and 28% complication rate [2]. The most frequent presenting symptoms of GCD are abdominal pain, nausea, vomiting, fever, altered bowel movement consistency and frequency, and melena [2]. The two most common complications of GCD are perforation and abscess formation. A 2% incidence of carcinoma has been reported within GCD.
This is the first reported case of GCD associated with bilateral leg swelling, diastolic dysfunction, and pericardial effusion. The improvement of diastolic dysfunction and resolution of the pericardial effusion after sigmoid colectomy suggest that the GCD caused mechanical compression severe enough to result in hemodynamic changes. There are two important learning points for emergency physicians in this case: 1) Use of echocardiography in patients with bilateral leg edema can occasionally lead to important diagnoses such as pericardial effusion 2) Mechanical compression from GCD can be associated with pericardial effusion.
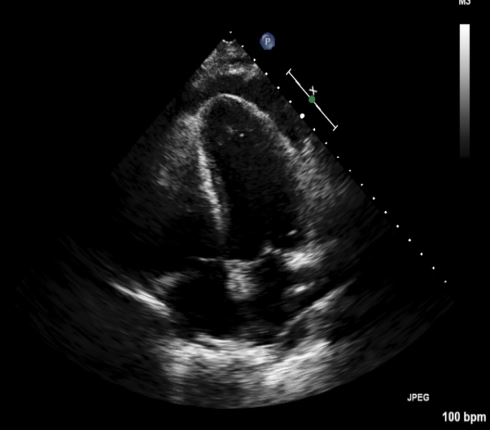
Figure 1: Clinical image.
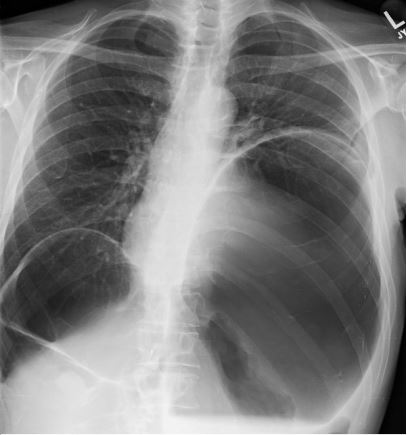
Figure 2: Clinical image.
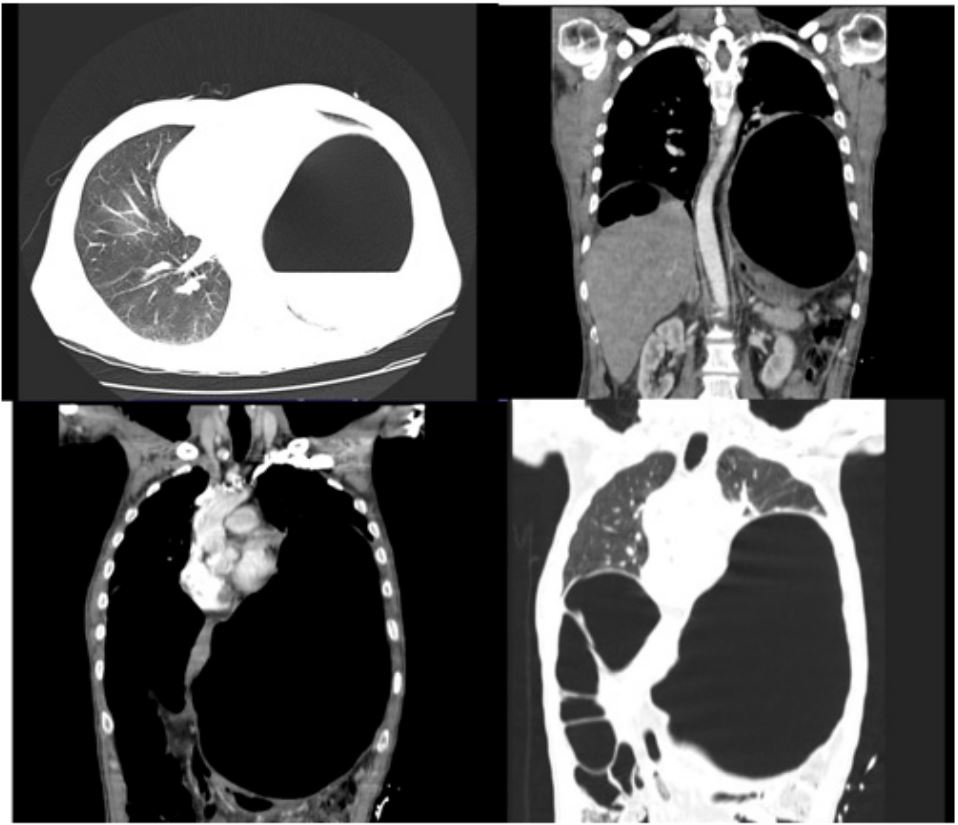
Figure 3: Clinical image.
References
- Parks TG. Natural history of diverticular disease of the colon. A review of 521 cases. British Medical Journal. 1969; 4: 639-642.
- Bonvin P, Bonte G. Diverticules géants du sigmoïde. Arch Mal Appar Dig Mal Nutr. 1946; 35: 353-5.
- Steenevoorde P, Vogelaar FJ, Oskam J, Tollenaar R. Giant Colonic Diverticula. Review of diagnostic and therapeutic options. Dig Surg. 2004; 21: 1-6.
- Durgakeri, P, Strauss P. Giant sigmoid diverticulum: A case report. Australasian Medical Journal. 2015; 8(3): 85-88.
