
Open Access, Volume 10
Blast from the past. It is possible to diagnose a myocardial infarction without testing from serum troponin
Yazid Kashquosh; Hesham Atwan; Sorcha Mildiner; Stephen Malnick*
Department of Internal Medicine C, Kaplan Medical Center, Hebrew University of Jerusalem, Rehovot 76100, Israel.
Stephen Malnick
Department of Internal Medicine C, Kaplan Medical Center, Hebrew University of Jerusalem, Rehovot
76100, Israel.
Email: stephen@malnick.net
Received : Apr 04, 2024,
Accepted : May 10, 2024
Published : May 20, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Malnick S (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Kashquosh Y, Atwan H, Mildiner S, Malnick S. Blast from the past. It is possible to diagnose a myocardial infarction without testing from serum troponin. Open J Clin Med Case Rep. 2024; 2240.
Introduction
The diagnosis of acute myocardium infection is typically that of anginal type chest pain accompanied by ECG changes and an increase in serum troponin levels. However, there are often atypical presentations, especially in women. We present a case of a middle-aged woman with severe prolonged vomiting in whom the diagnosis of myocardial function was not made at the initial presentation.
Case Presentation
A 55-year-old female, presented with severe diarrhea and intense vomiting. The sudden exacerbation of gastrointestinal symptoms included profuse diarrhea and vomiting up to 10 times a day. This resulted in an acute kidney injury and the serum creatinine level increased to 4.75 mg/dL. Following five days of hospitalization for rehydration both intravenously and subsequently orally, the patient was discharged feeling well with a serum creatinine of 0.88 mg/dL. Her previous medical history included well-controlled ulcerative colitis, hypothyroidism, impaired glucose tolerance, hyperlipidemia, and hypertension as components of the metabolic syndrome.
Due to prolonged weakness during the subsequent two weeks she was referred to our unit at Kaplan Medical Center. Symptoms included occasional vomiting, weakness, and loss of appetite. She had no chest pain or dyspnea. On admission, physical examination revealed stable vital signs, normal heart sounds without murmurs, equal breath sounds, and no peripheral edema. Laboratory investigations showed normal hemoglobin and leukocyte counts, normal CRP levels, but elevated liver enzymes, urea, and non-HDL cholesterol levels (Table 1).
An ultrasound of the abdomen was performed in view of the elevation of the serum transaminases. The liver appeared normal but there was a suspicion of a pancreatic cyst. An abdominal CT scan did not show a pancreatic cyst but did detect a pericardial effusion. She therefore was referred for a transthoracic echocardiogram that revealed new-onset heart failure with hypokinesia in the inferior and septal walls and an ejection fraction of 45%, in addition to a moderate pericardial effusion. Coronary angiography revealed normal coronary arteries. The patient was discharged home on standard therapy consisting of bisoprolol, aspirin, atorvastatin and dapaglifozin.
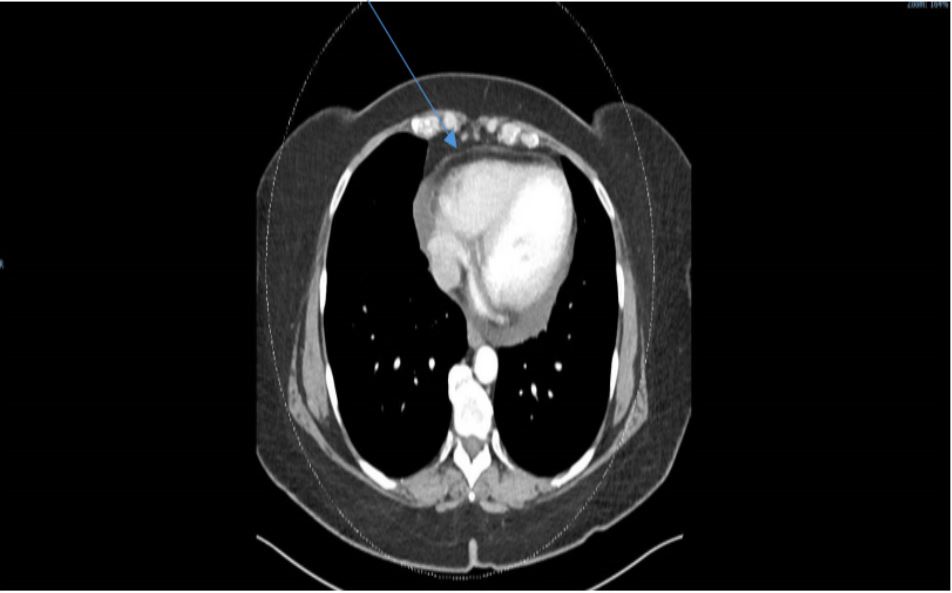
Figure 1: CT scan of the chest revealing a pericardial effusion (arrow)
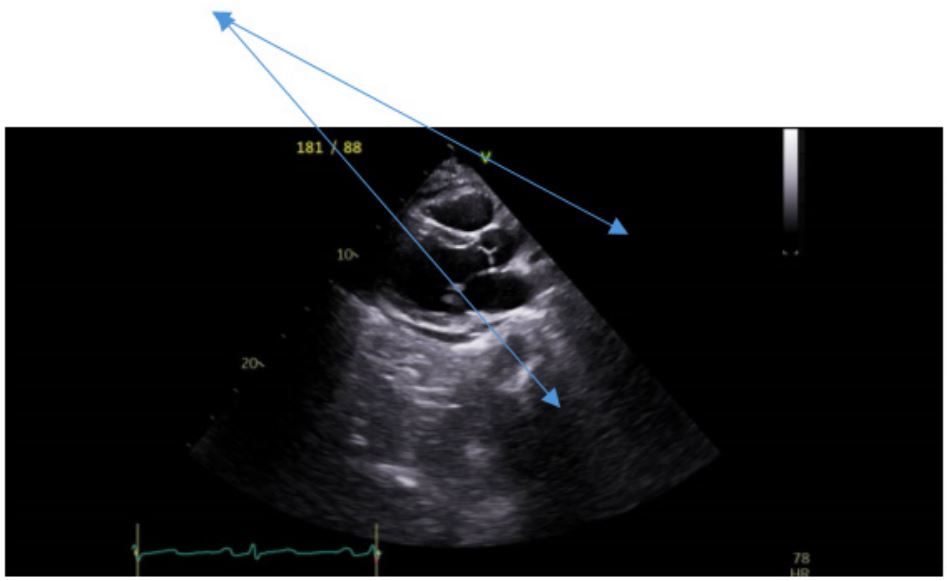
Figure 2: Transthoracic echocardiogram revealing a pericardial effusion (arrow).
Table 1: Clinical values.
| Date | 22/02 | 25/02 | 08/03 | 10/03 | 14/03 |
|---|---|---|---|---|---|
| AST (u/l) | 66 | 60 | 144 | 71 | 45 |
| ALT (U/L) | 33 | 27 | 125 | 93 | 62 |
| GGT (U/L) | 125 | 111 | 107 | ||
| LDH (U/L) | 415 | 453 | 247 | 153 | 164 |
| CPK (U/L) | 1530 | 451 | |||
| Creatinine mg/dL | 4.7 | 2.7 | 0.88 | 0.62 | 0.6 |
| Urea mg/dL | 103 | 80 | 53 | 27 | 17 |
Discussion
We present a case of a 56-year-old woman who was admitted for investigation of weakness and abdominal pain. She was usually healthy with no regular medication. Two weeks prior to her admission she developed severe vomiting and acute renal failure with a serum creatinine of 4.1 mg/dL. This resolved following supportive treatment with iv fluids. A review of her laboratory tests showed an elevation in her serum transaminases together with an increase in CKMB and a subsequent increase in LDH (Table 1). Abdominal imaging by ultrasound and CT scan was normal but did detect a pericardial effusion 1. At this stage transthoracic echocardiogram was carried out (Figure 2), which detected inferior and apical hypokinesia together with an ejection fraction that was reduced to 45% and a pericardial effusion. Coronary angiography revealed normal coronary arteries.
The diagnosis of myocardial infarction can sometimes be very difficult. For women the symptoms are much less specific than the classic symptoms experienced by men. This phenomenon has been termed the Yentel syndrome [1]. We do not think the complaint of such severe vomiting were due to the myocardial infarction but that the resulting volume depletion was the trigger for both the cardiac and renal injuries.
Laboratory enzyme determinations have for many years been employed to assist in the diagnosis of myocardial infarction. The classic picture is of an AST elevated more than the liver specific ALT together with an increase in the level of CPK MB. Subsequently there is a decline in the level of AST and an increase in the level of LDH. In this case serum troponin was not requested in the emergency room of the first hospital and the diagnosis of myocardial infarction was not made. At the time of admission to our medical center, the enzymes had normalized, and serum troponin levels were normal. This pattern of changes in enzymes is well known to physicians who were trained in the pre troponin era. A quick survey of 30 residents in the Department of Medicine in our Medical Center together and four fellows in cardiology showed that none of these physicians were aware of this enzymatic pattern. The general rule appears to be that troponin is required to diagnose a myocardial infarction and BNP is required to diagnose cardiac failure. Determination of the AST and ALT may also have prognostic importance [2].
Due to apical hypokinesia and hypokinesia, cardiac angiography was performed with no evidence found of coronary artery disease. We postulate that the severe fluid loss was the trigger for decreased perfusion in one of the coronary arteries, although there is no evidence to support this. There could have been acute myopericarditis but the degree of uncontrolled vomiting and severe fluid loss resulting in a serum creatinine of 9 mg/dL is unusual.
This case has been used as a teaching moment in our department. The AST ALT and CPK elevation needs to be reintroduced to the younger generation of physicians. In poorer countries serum troponin may not always be available. In our medical center, the cost of a troponin is 5 times that of serum transaminases.
We think this case is important to show to the physicians in training that a myocardial infarction can be diagnosed without determining the serum troponin level. It is also relevant for physicians from the developed world who may travel tom poorer countries to work.
References
- Healy, B. The Yentl Syndrome. New England Journal of Medicine. 1991; 325: 274-276.
- Gao M, et al. Association of serum transaminases with short- and long-term outcomes in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. BMC Cardiovasc. Disord. 2017; 17: 1-8 (2017).
