
Open Access, Volume 10
Solitary fibrous tumor of the prostate: Case report and review of the literature
M El Ouazzani1*; A Nebgui2; H Rachidi1; I Boujguenna1; K Rabbani2; A Louzi2; H Rais1; A Belbachir1
1Department of Pathology, Med VI University Hospital, Marrakesh, Morocco.
2Department of General Surgery, Med VI University Hospital, Marrakesh, Morocco.
M El Ouazzani
Department of pathology, Med VI university hospital, Marrakesh, Morocco.
Email: meryem.el.ouazzani.88@gmail.com
Received : Mar 20, 2024,
Accepted : May 07, 2024
Published : May 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Solitary Fibrous Tumor (SFT), typically found in the pleura, is exceptionally rare in the prostate. We present the case of a 54-year-old man with prostatic SFT, initially revealed as an abdominopelvic mass. Subsequent investigations shown a vascular tumor. The pathological examination found a 23 cm tumor originating from the prostate, composed of short spindle-shaped and polygonal cells with mild nuclear atypia. Occasional mitoses were observed, with vascular invasion. Immunohistochemically, the tumor cells strongly expressed CD34 and STAT6. The maximum Ki-67 labeling index for the tumor cells was 4%. This case report has highlighted one of the rare occurrences of solitary fibrous tumor. A comprehensive microscopic examination paired with an immunohistochemical analysis will be necessary to establish an accurate diagnosis.
Keywords: Solitary fibrous tumor; Prostate; Immunohistochemistry.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © El Ouazzani M (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: El Ouazzani M, Nebgui A, Rachidi H, Boujguenna I, Rabbani K, Louzi A, Rais H, et al. Solitary fibrous tumor of the prostate: Case report and review of the literature. Open J Clin Med Case Rep. 2023; 2239.
Introduction
Solitary Fibrous Tumor (SFT) is a rare spindle cell neoplasm primarily found in pleural tissues [1]. However, there have been reports of extra-pleural occurrences in the past two decades [2]. While the origin and etiology of SFTs are uncertain, they are believed to originate from mesenchymal fibroblastic cells. The presence of SFT in the prostate is exceptionally rare, presenting a clinical challenge when distinguishing it from other spindle cell lesions in the prostate. We report a case of solitary fibrous tumor in the prostate of a 54-year-old patient.
Case Report
In December 2021, a 54-year-old diabetic man presented a pelvic discomfort. Clinical examination revealed a painless abdominopelvic mass measuring approximately 20 cm in length and 10 cm in height. The mass was mobile relatively to both superficial and deep tissue planes. An abdominopelvic CT scan revealed a heterogeneous abdominopelvic mass with regular contours, located centrally, and showing heterogeneous enhancement upon contrast medium administration.
The tumor was multinodular, arising from the prostate and causing displacement of large blood vessels. The tumor measures 23 × 21 × 15 cm (Figure 1). The mass displayed a homogeneous beige-white appearance, with a lobulated structure and no evidence of necrosis (Figure 2).
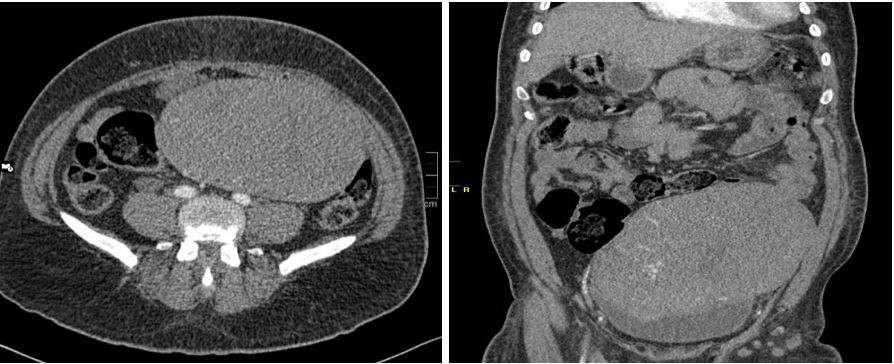
Figure 1: Imaging of prostatic SFT. Pelvic axial CT-scan detecting a medial massive mass lesion in pelvic
regions.

Figure 2: Macroscopic appearance: the mass was homogeneous beige-white, polylobed without necrotic
changes.
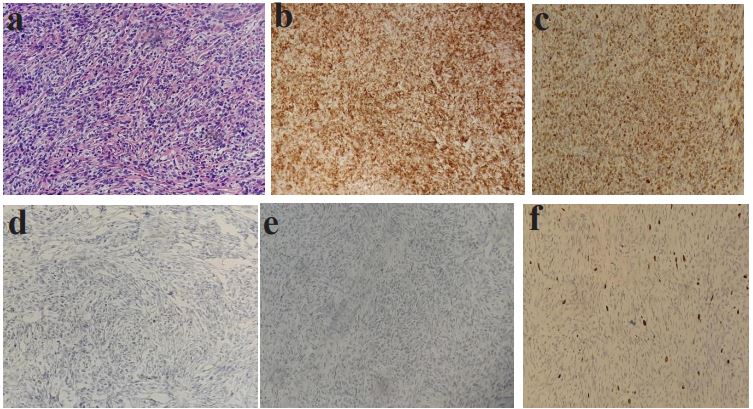
Figure 3: Prostatic SFT: histological aspects. (a) low-power view of a highly cellular area with characteristic ‘staghorn’ vessels (black arrows) (HE staining, original magnification ×40) (b) Tumor cells strongly express CD34 (CD34 immunodetection, original magnification ×100). (c) Tumor cells strongly expressmagnification ×100). (d) Absence of expression of large
cytokeratin. (e) Absence of expression of CD117. (f) Low expression of mitotic index Ki67 4%.
Histological examination revealed a mesenchymal proliferation with a fascicular appearance with varying cell density. It, occasionally, demonstrates a swirling patterns The cells were spindle-shaped with regular elongated nuclei lacking atypia and only occasional mitotic figures. The tumor exhibited a hyaline stroma containing numerous blood vessels, reminiscent of a hemangiopericytic vascular pattern (Figure 3). Immunohistochemical analysis showed strong expression of CD34 and STAT-6 by the tumor cells, with no expression of epithelial (pancytokeratin), smooth muscle (Desmin), or Schwann cell (PS100) markers. The final diagnosis was an SFT originating from the base of the prostate.
Discussion
Solitary fibrous tumor is a mesenchymal neoplasm originated from the mesothelial lining of tissues, primarily in the pleura and pericardium. It appears as a spindle-shaped cells dispersed in a highly vascularized stroma with abundant bundles of collagen fibers [3]. SFT can affect both men and women, with a median age of 40-60 years. Our patient presented with a painless abdominal mass, which is a common clinical presentation in cases of intraabdominal SFT [4]. Most extra-thoracic SFTs are benign, although they may recur or metastasize after complete surgical removal, even in the absence of histopathological malignancy features [5]. Criteria suggesting malignancy include tumor size (>50 mm), nuclear polymorphism, increased cellularity, elevated mitotic activity (>4 mitoses/10 fields), anaplasia, necrosis, and hemorrhage [6]. The definitive diagnosis is typically based on histopathological examination of surgical specimens, as biopsy fragments may not be as effective due to the heterogeneous appearance of the tumor [7]. Macroscopically, SFT often presents as a single, firm, oval mass with an encapsulated appearance, usually cleavable at its borders, pale grayish-pink in color, and may contain pseudocystic spaces [3]. Histologically, SFT exhibits variable zones of different cellular density, including areas rich in spindle cells, adipose regions, and highly vascularized sectors with arborized vessels, creating a hemangiopericytic appearance [3]. This wide spectrum of differential diagnosis presents a challenge. The main differential diagnosis includes other intra-abdominal mesenchymal tumors like Gastrointestinal Stromal Tumors (GIST), calcifying fibrous pseudotumor, neurofibroma, schwannoma, hemangiopericytoma, and desmoid tumors [9]. Immunohistochemistry plays a crucial role in distinguishing SFT from other entities [8]. The absence of Smooth Muscle Actin (SMA) or desmin markers helps to differentiate it from smooth muscle tumors. Epithelial markers (cytokeratin, epithelial membrane antigen), and S100 protein are typically negative in SFT, although focal cytokeratin expression has been reported in some malignant forms [9]. The negativity for CD117 helps to exclude Gastrointestinal Stromal Tumors (GIST), and CD34 is a consistently reliable marker for SFT, as seen in our case. A recent marker, anti-STAT6 antibody, is reported to be more specific for the diagnosis of SFT and rarely positive in other tumor types.
Benign SFTs typically exhibit slow progression and low recurrence rates (2-15%). The quality of surgical excision plays a critical role in recurrence prevention. The complete surgical excision is mandatory in the treatment of SFT.
Conclusion
Solitary fibrous tumors are exceptionally rare in the prostate and constitutes a significant diagnostic challenge in differentiating them from other extrapleural mesenchymal tumors. The pathologist's role is pivotal, providing key information regarding the tumor's benign or malignant nature. The immunohistochemical phenotype (STAT6+, CD34+) is crucial to confirm the diagnosis.
References
- Robinson LA: Solitary fibrous tumor of the pleura. Cancer Control. 2006; 13: 264-269.
- Vallat-Decouvelaere AV, Dry SM, Fletcher CD. Atypical and malignant solitary fibrous tumors in extrathoracic locations: Evidence of their comparability to intra-thoracic tumors. Am J Surg Pathol. 1998; 22: 1501-1511.
- Goldblum R, Folpe AL, Weiss SW. Soft tissue tumors of intermediate malignancy of uncertain type. In: Goldblum R, Folpe AL, Weiss SW (eds) Enzinger and Weiss’s soft tissue tumors. 6th edition. Elsevier Saunders USA. 2014; 1002-17.
- Park M, Araujo D. New insights into the hemangiopericytoma/solitary fibrous tumor spectrum of tumors. CurrOpin Oncol. 2009; 21: 327-31 9.
- England DM, Hochholzer L, McCarthy MJ. Localized benign and malignant fibrous tumors of the pleura. A clinicopathologic review of 223 cases. Am J Surg Pathol. 1989; 13: 640-5
- Chan JKC. Solitary fibrous tumor everywhere, and a diagnosis in vogue. Histopathology. 1997; 31: 568-76.
- Saint-Blancard P, Jancovici R. Tumeur fibreuse solitaire du rétropéritoine. Rev Med Interne. 2009; 30: 181-5
- Yoshida A, Tsuta K, Ohno M, et al. Immunohistochemistry is helpful in the diagnosis of solitary fibrous tumors. Am J Surg Pathol. 2014; 38: 552-9
- Cavazza A, Rossi G, Agostini L, et al. Cytokeratin positive malignant solitary fibrous tumour of the pleura: An unusual pitfall in the diagnosis of pleural spindle cell neoplasms. Histopathology. 2003; 43: 606.
