
Open Access, Volume 10
Forestier disease: A possible cause of decannulation failure
Lanini Barbara*; Isabella Romagnoli; Elisa Chellini; Alessandro Giuseppe Calabrò; Barbara Binazzi; Stella Sani; Francesco Gigliotti
Pulmonary Rehabilitation Unit, IRCCS Fondazione Don Carlo Gnocchi, Via di Scandicci 269, 50143 Firenze, Italy.
Lanini Barbara
Pulmonary Rehabilitation Unit, IRCCS Fondazione Don Carlo Gnocchi, Via di Scandicci 269, Firenze, Italy.
Email: blanini@dongnocchi.it
Received : Apr 03, 2024,
Accepted : May 06, 2024
Published : May 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Barbara L (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Barbara L, Romagnoli I, Chellini E, Calabrò AG, Binazzi B, Sani S, Gigliotti F, et al. Forestier disease: A possible cause of decannulation failure. Open J Clin Med Case Rep. 2024; 2238.
Introduction
Diffuse Idiopathic Skeletal Hyperostosis (DISH) [1] also known as Forestier disease, is a noninflammatory, systemic skeletal disease of unknown aetiology. DISH is a common but underdiagnosed disease that is usually observed in elderly people and has been reported to affect up to 10% of patients over 65 years of age [2]. The diagnosis is primarily radiological characterised by the ossification of the anterior longitudinal ligament, with osteophytes formation along the spinal column of at least four contiguous vertebral bodies, a minimal degree of degenerative disc disease and absence of apophyseal joint ankylosis and sacroiliac joint fusion, erosions, or sclerosis [3]. DISH is usually asymptomatic but may compress the posterior wall of the aero digestive tract and lead to dysphagia, globus, hoarseness, stridor, dyspnea and neurological problems. Although dysphagia is not uncommon among the presenting symptoms of DISH, dysphonia and stridor are rarely reported. Cervical hyperostosis in patients with DISH is responsible for 17%-28% incidence of dysphagia, and about 8% of patients failed to respond to conservative treatment and surgical excision through an anterior cervical approach was required [3]. Many studies have been conducted on the surgical approach [4] and anaesthetic evaluation of patients with DISH [5]. Less known are the difficulties in weaning from the tracheostomy tube in these patients, especially when the diagnosis of DISH is unknown.
Case Presentation
A 78-year-old man was admitted to the high Intensity Pulmonary Rehabilitation Unit of the Don Gnocchi Foundation in Florence after a prolonged Intensive Care Unit hospitalisation due to sepsis started from lower limbs erysipelas. At the intensive care unit the patient underwent multiple orotracheal intubation for recurrent sepsis before a tracheostomy tube was placed. The medical history of the patient included diabetes mellitus, arterial hypertension, ischemic heart disease and dyslipidemia.
At the admission to rehabilitation unit, the patient was alert oriented and mnesic, overweight, bedridden, wearing a tracheostomy tube and a nasogastric feeding tube. Neurologic examinations were normal, cervical spine range of motion was decreased in extension and flexion without no reported pain during movement and no tenderness over the spinous processes.
The patient underwent a multidisciplinary customised rehabilitation program aimed at weaning from the tracheostomy tube, restoring oral feeding and recovering motor impairments. The program was carried out by pulmonologists, speech and swallow therapists and respiratory therapists. According to previous literature on tracheostomy tube removal, [6,7] swallowing assessment was combined with the pathophysiological assessment of respiratory function (airway patency and cough). At the first logopaedic evaluation, the patient immediately tolerated the tracheostomy tube with deflated cuff with stable peripheral O2 saturation and clinical monitoring. The blue dye test performed with a speaking valve showed an immediate inhalation with cough. No swallowing act could be elicited either spontaneously or on request. A swallowing retraining program was therefore set up and feeding was continued through a gastrostomy tube.
With the aim of promoting weaning, the tracheostomy tube was replaced with a smaller calibre one. The subsequent blue dye test for the evaluation of oral-nasal-pharyngeal secretion management, performed with the speaking valve, was negative. Due to the inability to swallow semi-solid boluses, artificial nutrition was anyway continued via gastrostomy. With capped cannula the patients showed an effective cough and stable arterial blood gases breathing room air but during sleep multiple obstructive apnoea were detected.
Due to the lack of improvement in swallowing function, a fiberoptic endoscopic evaluation was performed (Figure 1): a severe anteriorization of the posterior pharyngeal wall was coming into contact with the epiglottis with consequent reduction of the lumen and marked stagnation of secretions. To investigate the causes of pharyngeal stenosis, an x-ray of the cervical spine was performed (Figure 2). The x-ray showed anterior cervical osteophytes at C3, C4, C5 and C6; therefore, computed tomography was carried out (Figure 3). Osteophytic alterations with a tendency towards bridging fusion in the C2-C5 tract was described. Coarse ossification of the anterior longitudinal ligament with evidence of a spur shaping an acute angle at the level of the epiglottis, significantly imprinted the posterior wall of the hypopharynx and determined a clear focal reduction in the calibre of the lumen. The diagnosis of ankylosing spondylitis, infection and malignancy were ruled out and Forestier Disease was confirmed.
The relevant reduction in the calibre of the hypopharynx (Figure 1) advised against the removal of the cannula. For these reasons the patient was discharged at home with total enteral nutrition via gastrostomy and wearing a phonatory valve also during sleep. Upon discharge the motor impairment was fully restored and the patient was able to walk independently. The evaluation for surgical treatment of DISH was scheduled given the patient’s clinical stability.
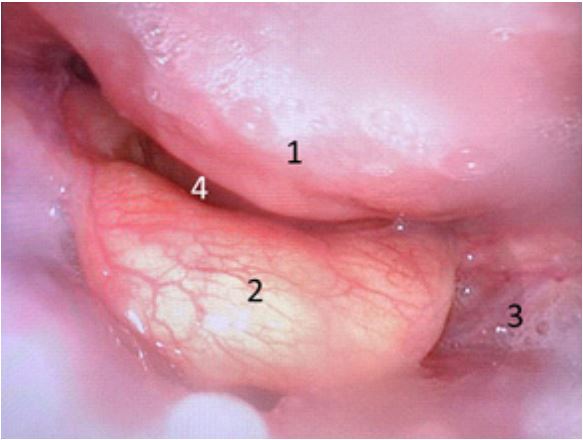
Figure 1: Fiberoptic endoscopic evaluation. 1: posterior
pharyngeal wall, 2: epiglottis, 3: stagnation of secretions,
4: lumen.
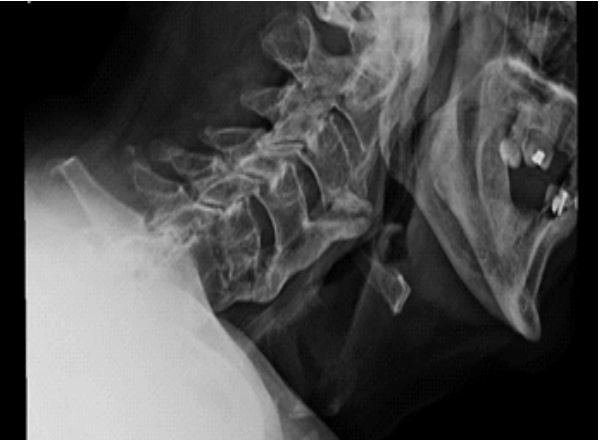
Figure 2: Cervical X ray.
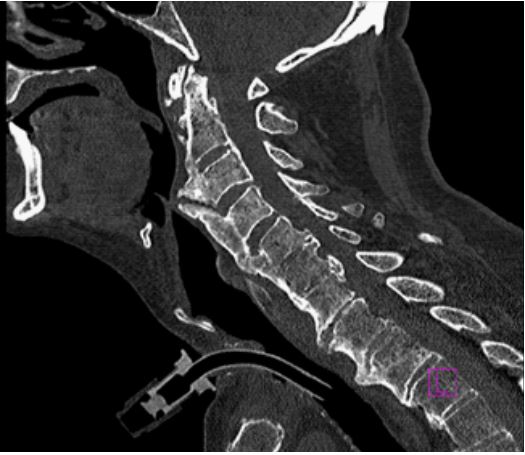
Figure 3: Computed Tomography.
Conclusion
Given the high incidence of asymptomatic DISH, radiography of the cervical spine should be considered in selected cases of difficult weaning from the tracheostomy tube.
Acknowledgements: We acknowledge Paola Graziani for fiberoptic endoscopic evaluation.
References
- Zarei M, Golbakhsh M, Rostami M, Moosavi M. Dysphonia, stridor and dysphagia caused by diffuse idiopathic skeletal hyperostosis: Care report and review of literature. Adv Biomed Res. 2020; 9: 47-50. https://doi.org/10.4103/abr.abr_50_20
- Matan AJ, Hsu J, Fredrickson BA, Management of respiratory compromise caused by cervical osteophytes: A case report and review of the literature. Spine J. 2002; 2: 456-9. https://doi.org/10.1016/s1529-9430(02)00205-x
- Mader R, Verlaan JJ, Buskila D. Diffuse idiopathic skeletal hyperostosis: clinical features and pathogenic mechanisms. Nat Rev Rheumatol. 2013; 9: 741-50. https://doi.org/10.1038/nrrheum.2013.165
- Maiuri F, Cavallo LM, Corvino S, Teodonno G, Mariniello G. Anterior cervical osteophytes causing dysphagia: choice of the approach and surgical problems. J Craniovertebr Junction Spine. 2020;11(4): 300-309. https://doi.org/10.4103/jcvjs.JCVJS_147_20
- Xu M, Liu Y, Yang J, Liu H, Ding C. Ossification of the cervical anterior longitudinal ligament is an underdiagnosed cause ofdifficult airway: a case report and review of the literature. BMC Anesthesiol. 2020; 20(1): 161. http://doi.org/10.1186/s12871-020-01077-9
- Garuti G, Reverberi C, Briganti A, Massobrio M, Lombardi F, et al. Swallowing disorders in tracheostomised patients: A multidisciplinary/multiprofessional approach in decannulation protocols. Multidiscip Respir Med. 2014; 9: 36-46. https://doi.org/10.1186/2049-6958-9-36
- Lanini B, Binazzi B, Romagnoli I, Chellini E, Pianigiani L, et al. Tracheostomy decannulation in severe acquired brain injury patients: The role of flexible bronchoscopy, Pulmonology. 2021; 1: S2531-0437(21)00115-X. https://doi.org/10.1016/j.pulmoe.2021.05.006.
