
Open Access, Volume 10
Omental hydatid cyst in pregnant women: A rare localization
Yasmine Ben Ali
Hopital Farhat Hached, Tunisia.
Yasmine Ben Ali
Hospital Farhat Hached, Tunisia.
Email: benali07yasmine@gmail.com
Received : Apr 05, 2024,
Accepted : May 03, 2024
Published : May 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Hydatid cysts are a public health problem in endemic areas. It mainly affects the liver and lung. Omental involvement is rare, accounting for less than 1% of hydatid localizations. We report a rare case of 26-yearold pregnant women presented for abdominal pain and feeling of mass in the pelvic area for 6 months. The physical examination showed an abdominal distention and tenderness in the right iliac fossa. Omental hydatid cyst was suspected on ultrasound and confirmed by magnetic resonance imaging and management was done with cystectomy.
Keywords: Hydatid cyst; Omentum; Pregnant woman; Surgery; Case report.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Ben Ali Y (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Ben Ali Y. Omental hydatid cyst in pregnant women: A rare localization. Open J Clin Med Case Rep. 2024; 2237.
Introduction
Hydatidos is a disease caused by the development in the human body of the larval form of a small dog taenia: Echinococcus granulosus [1] Tunisia, a traditional breeding country, remains one of the countries most infested by Echinococcosis granulosus. Hepatic and pulmonary involvement predominates, but the cyst can affect all organs [2]. Omental hydatid cysts are rare and misleading, accounting for less than 1% of hydatid localizations [2,3]. We report an observation of omental hydatid cyst in pregnant women with clinical presentation, imagery findings and pathologic characteristics.
Observation
A 26 years old female patient, resident of rural area; presented with dull pelvic pain of 6 months duration with no anorexia, nausea, vomiting, weight loss, fever or lethargy; followed by abdominal swelling. she had no other medical history; delivered a baby 2 years ago by normal vaginal delivery. The date of the last period was unknow.
Clinical examination showed an abdominal distention; she had tenderness in the right iliac fossa. The pelvic ultrasonography revealed a 13×11 cm well-defined, heterogeneous solid-cystic cyst with no internal flow at colour doppler imaging situated in the pouch of Douglas (Figure 1) also, an accidental discovery of a 20 weeks pregnancy.

Figure 1: The MRI: showed a 13×11 cm well-circumscribed,
multiloculated cystic that can be in favor of a peritoneal or
ovarian hydatic cyst (Figure 2).
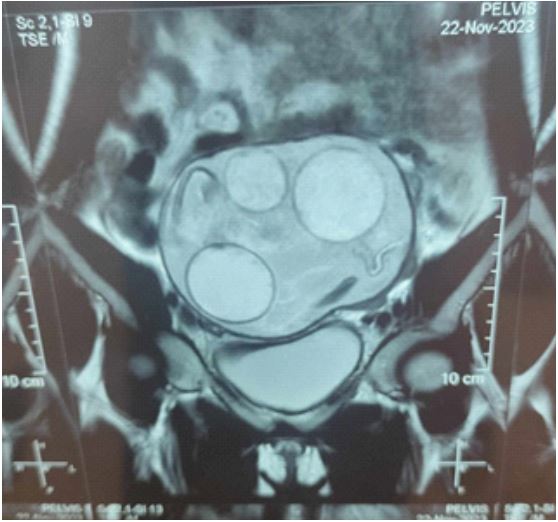
Figure 2: Anti-echinococcus antibodies (IHA) screen
was negative.
The fact that the patient was pregnant, and the uterus had caused a mass effect on the cyst, which can increase the risk of its rupture and cause anaphylaxis. We decided to operate the patient. We proceed to a midline laparotomy, exploration showed a huge cyst measuring 150* 130 mm in rising from the omentum complicated with omental torsion (Figures 3,4) so that we performed omental detorsion and cystectomy. Cyst was sent for histopathologic examination and the abdominal cavity was washed with 10% hypertonic saline. Progress was good, ultrasound showed an evolutive pregnancy and the patient was discharged two days later.
Pathological examination confirmed the diagnosis of hydatid cyst (Figures 5,6).
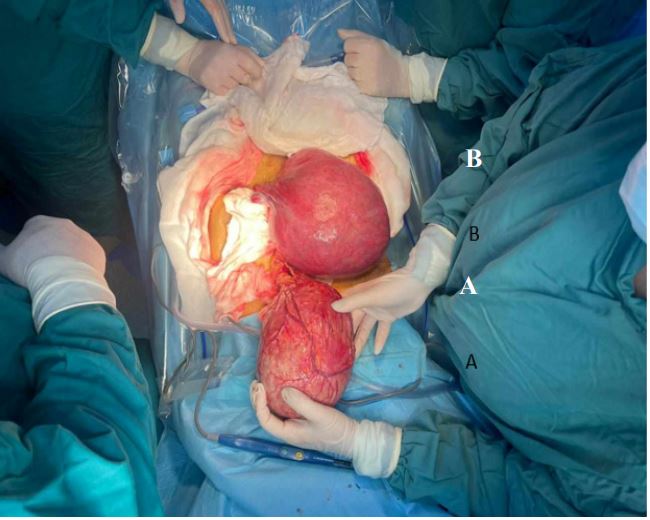
Figure 3: A: The gravid uterus. B: The hydatid cyst.
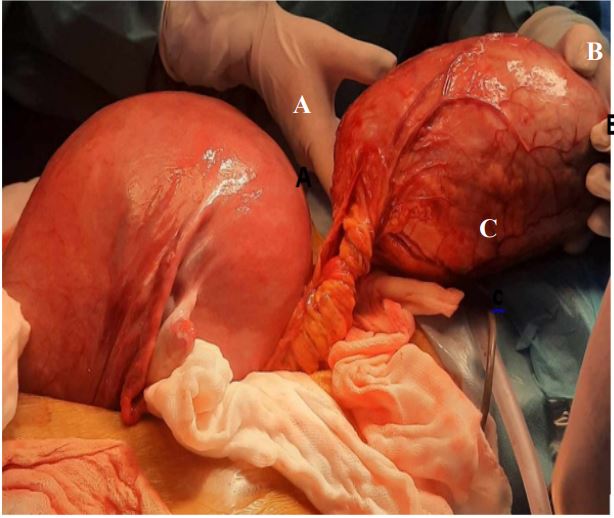
Figure 4: A: The gravid uterus. B: The hydatid cyst. C: Epiploon.

Figure 5: Daughter cysts.

Figure 6: The graviploon.
Discussion
Hydatid cyst is a parasitic disease caused that is a public health problem in endemic areas, particularly around the Mediterranean basin [1]. Hydatid cysts are generally found in liver and lungs, according to literature rare localizations Can be identified such as in ovaries, skeleton, kidney, brain, etc. Omentum most likely less than 1% some cases were reported but we can’t find substantial references and sufficient data [2-4].
Hydatid cyst of omentum is extremely rare, and is due to contamination via the hematogenous route, suggesting a rupture of the pulmonary or hepatic filter by the parasite to gain access to the general circulation [1].
Symptoms of echinococcosis granulosus infection depends on the site, the size and the evolutionary stage of the cysts cycle. So that Patient can be asymptomatic, present with abdominal pain, vomiting nausea, abdominal distention due to mass effect or with more severe condition such as anaphylactic shock due to cyst rupture [5].
Computed tomography and ultrasonography contribute to the diagnostic process [5]. The most characteristic ultrasonographic signs of hydatid cysts are the presence of one or more peritoneal cysts, preferentially located in the sloping region. The contents of these cysts are anechogenic or slightly echogenic, and the proligeral membrane may be visualized within the cyst when detached ‘snake sign’ [6].
Magnetic Resonance Imaging (MRI) is considered the gold standard for assessing large, problematic or ambiguous cysts. MRI typically shows a T1-hypointense, T2-hyperintense lesion with peripheral hypointensity related to the fibrous capsule. Diagnosis is facilitated by the observation of daughter cysts and intracystic membranes [7].
Due to it different evolutionary stages a hydatid cyst may be assimilated to numerous differential diagnosis such as cystic retroperitoneal masses (dermoid cysts), tubercular abscesses or pyogenic abscesses. If necessary, magnetic resonance imaging can be used to make a differential diagnosis [5].
Biological examinations are limited to hydatid serology. It is of great diagnostic value in the event of a positive. However, in extra-hepatic localizations, biology, and in particular hydatid serology, is not always sensitive (30-70%) [1].
Hydatid cyst in pregnant women essentially poses a problem of therapeutic attitude in relation to the timing and the choices of the go to procedure.
May we mention that the pregnancy itself as it develops will put on additional abdominal pressure and may cause catastrophic complications as it can weaken the cyst, cause it the fistulise or even rupture which in the short run can be fatal (anaphylactic shock).
In the absence of complications requiring urgent treatment, the second trimester is considered the best time to operate on a pregnant woman, due to the lower risk of miscarriage (0 vs. 12% in the first trimester) and premature delivery (5-8% vs. 30% in the third trimester) [8].
Treatment of choice for hydatid cysts is total cystectomy without contamination. The association of antiparasitic therapy to surgical management in pregnant women still controversial in literature because of its embryotoxic effect confirmed in animals [9,10].
Conclusion
Hydatidosis is a very common parasitosis in Tunisia, and can develop in any organ of the body, which means that doctors should consider this diagnosis in the event of a cystic tumour of any organ in a patient living in an endemic zone. Finally, we must stress the importance of primary prevention of this disease, in order to reduce its incidence in our country.
References
- Yadav SK, Ruchal A, Gaurav B, Bhattarai B, Khatiwada P, et al. Retroperitoneal hydatid cyst challenging the diagnosis: Case report with review of literature. Int J Surg Case Rep. 2023; 114: 109106.
- Bellil S, Limaiem F, Bellil K, Chelly I, Mekni A, et al. Épidémiologie des kystes hydatiques extrapulmonaires: 265 cas en Tunisie. Médecine Mal Infect. 2009; 39(5): 341‑3.
- Eckert J, Deplazes P. Biological, Epidemiological, and Clinical Aspects of Echinococcosis, a Zoonosis of Increasing Concern. Clin Microbiol Rev. 2004; 17(1): 107‑35.
- Salamone G, Licari L, Randisi B, Falco N, Tutino R, Vaglica A, et al. Uncommon localizations of hydatid cyst. Review of the literature. Il G Chir - J Ital Surg Assoc. août 2016; 37(4): 180.
- Belouad M, Benlghazi A, Allaoui M, Benali S, Bouhtouri Y, et al. Kyste hydatique pelvien primitif, une localisation inhabituelle: A propos d´un cas. PAMJ - Clin Med. 2022; 9(5). https: //www.clinical-medicine.panafrican-med-journal.com/content/article/9/5/full
- Brunetti E, Tamarozzi F, Macpherson C, Filice C, Piontek MS, et al. Ultrasound and Cystic Echinococcosis. Ultrasound Int Open. 2018; 4(3): E70‑8.
- El Alaoui O, Jelti O, Lachkar A, Abdeljaouad N, Yacoubi H. Primary Hydatid Cyst of the Gluteal Muscle: A Case Report. Cureus. 16(1): e51629.
- Rachad M, Fdili FZ, Slimani O, Chaara H, Bouguern H, et al. La rupture intra péritonéale d’un kyste hydatique au cours de la grossesse: A propos d’un cas rare. Pan Afr Med J. 2012; 11. https: //www.ncbi.nlm.nih.gov/pmc/articles/PMC3283012/
- Gul M, Younis I, Rathinavelu B, Ben Ghashir NS, Seeli RK, et al. Management of Hydatid Cysts in Pregnancy: A Report of Two Cases and a Review of Literature. Cureus. 15(10): e46425.
- Tekin AF, Yilmaz H, Kara T, Seçkin E, Aybay MN, et al. A very rare case: Hydatid cyst surrounding uterus and magnetic resonance imaging findings in the pregnant patient. Radiol Case Rep. 2019; 14(2): 168‑70.
